
Abstract
Purpose:
There is no clear evidence that high-power (HP) laser generators perform better than low-power (LP) ones in terms of lithotripsy outcomes. We aimed to perform a systematic review of literature to compare the efficacy outcomes of both HP and LP during ureteroscopic lithotripsy.
Materials and Methods:
A computerized bibliographic search of the Medline, Embase, and Cochrane databases was performed for all studies reporting perioperative outcomes of HP and LP lithotripsy. Using the methodology recommended by the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines, we identified 22 nonrandomized noncomparative retrospective studies published between 2015 and 2019 that were eligible for inclusion in this systematic review. Because of the lack of comparative studies, we decided to perform two separate meta-analytic syntheses for LP and HP studies, then we compared them using a Wald-type test.
Results:
Overall, the selected studies included 6403 patients. Study design, exposure assessment, selection criteria, and outcome of interest were heterogeneous. LP studies were more common (n = 17, 77%), whereas HP studies were more common in the latest inclusion period. Faster lithotripsy (32.9 minutes vs 63.9 minutes, p < 0.01) was observed in HP studies. However, stone volume resulted twofold higher (2604 mm3 vs 1217 mm3, p = 0.048) in LP studies. Pooled stone-free rate was similar in both LP and HP studies, 81% and 82%, respectively, p > 0.05. No difference in complication rate was observed between the two groups, p = 0.12.
Conclusions:
HP laser lithotripsy appears to require shorter operative time, with similar stone-free and complication rates as compared with LP traditional lithotripsy. However, when taking into account stone burden, this advantage seems to be lost, or at least not to be comparable with what observed in laboratory studies. Because of the lack of high-level comparative evidence, further clinical studies are needed to elucidate the benefits of using HP laser generators during ureteroscopic stone treatment.
Introduction
Ureteroscopy (URS) is the first choice procedure for ureteral and renal stones <20 mm according to international guidelines. 1,2 After the introduction of holmium:YAG (Ho:YAG) laser lithotripsy in 1992, 3 this technique became the gold standard for ablating stones during URS. During the past years, both clinical and laboratory studies led to a substantial agreement in the endourologic community regarding the optimal laser settings to be utilized to properly ablate urinary stones. 4 Taken together, this evidence suggests that it is possible to perform intracorporeal lithotripsy with low-power (LP, i.e., ≤35 W) laser devices. During recent years, high-power (HP) Ho:YAG laser generators (up until 120 W) began to appear on the market and routinely employed.
HP devices may achieve frequencies up to 80 Hz. Recent publications advocate that this setting will translate into higher efficiency 5,6 ; however, clinical data demonstrating superior lithotripsy outcomes are not available. Despite this, HP lasers gained widespread diffusion and are currently used by 45.2% of the urologist in the United States. Because of the lack of comparative evidence between LP and HP laser lithotripsy, we aimed to perform a systematic review of available clinical studies reporting either on LP or HP outcomes to obtain an indirect meta-analytic clinical comparison of these two different approaches in terms of both clinical efficiency and safety.
Evidence Acquisition
Search strategy
This systematic review was conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement. 7 A literature search was conducted on PubMed/Medline and Scopus in May 2018. The search strategy included the following terms: “Holmium laser” AND/OR “Lithotripsy, Laser”[Mesh] AND “Ureteroscopy”[Mesh]. We further applied “Humans,” “English language” and “2015–2019 time-period” filters.
Inclusion criteria
As recommended by the PRISMA guidelines, we used the population (P), intervention (I), comparator (C), and outcome (O) approach (PICO) to define study eligibility. 7 Reports were considered relevant to this systematic review if they compared adult patients (>18 years) found with upper urinary tract stone disease (P) treated with URS and either LP or HP Ho:YAG laser lithotripsy (C) to determine perioperative outcomes, namely operative time, complications, and stone-free rate. Studies including non-Ho:YAG laser energy sources, pediatric population, spinal deformities, renal malformations, transplanted kidneys, and semirigid ureteroscopes were not considered. For pragmatic reasons, we decided to include single-arm observational studies, because of the lack of comparative studies.
Systematic Review Process
After removing duplicate studies, two authors (F.P. and E.V.) carried out an independent review of 201 abstracts to select studies for full-text evaluation. Any disagreement about whether or not to include a study was resolved by consulting the senior author (O.T.). After applying inclusion criteria and panel selection, 22 articles were eventually included in this systematic review. 8 –29 Figure 1 shows the PRISMA flowchart describing the selection process that led to final selection of included studies.
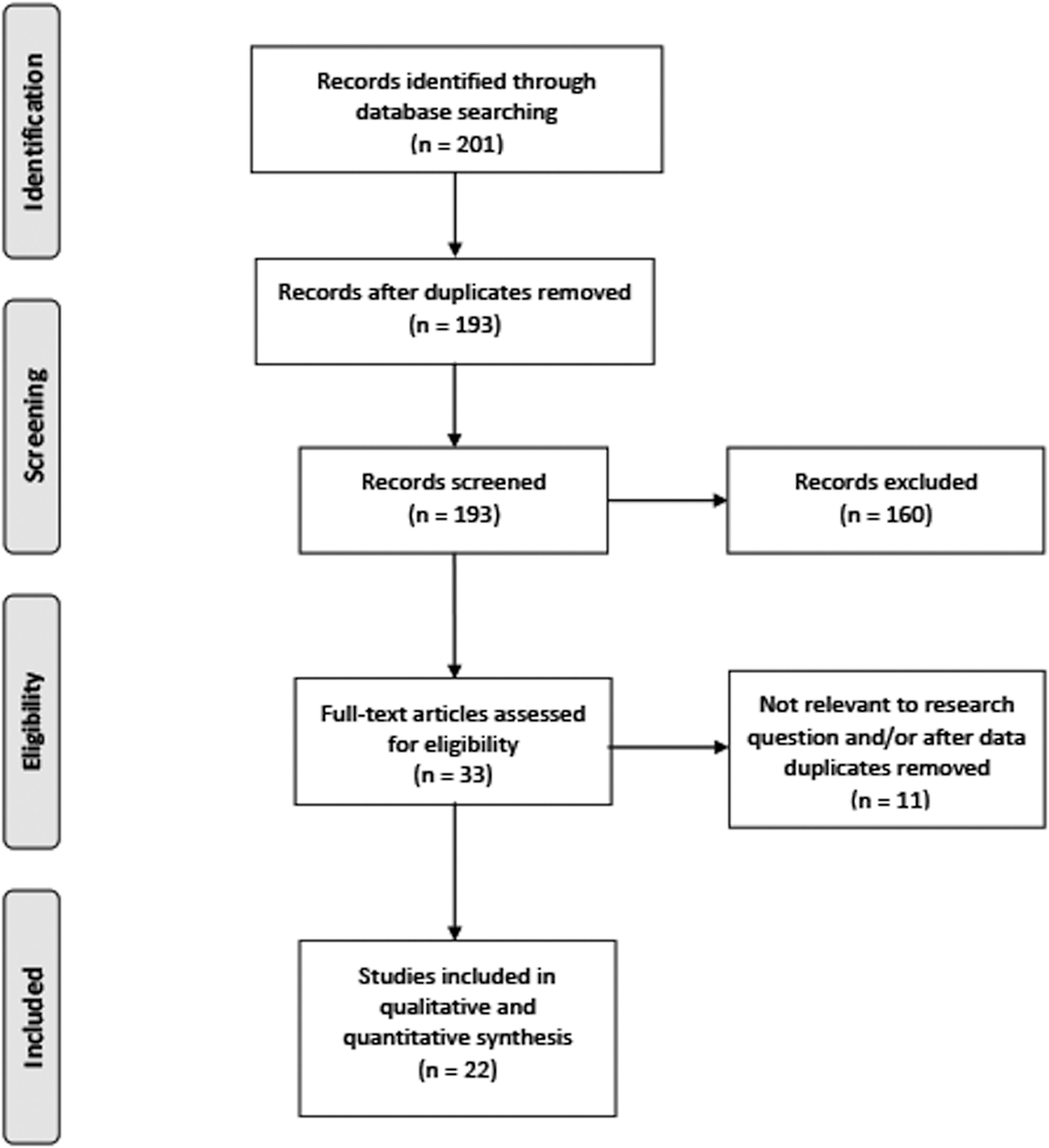
Preferred reporting items for systematic reviews and meta-analysis flow diagram showing the outcome of the initial and additional searches resulting in the full studies included in the review.
Data extraction
Data were independently extracted from all included studies by four authors (F.P., F.Q., S.S., and H.K.), who subsequently cross-checked them to ensure their accuracy. A standardized data extraction form was created a priori and used to collect study-level data, such as the study design, number of participants, and type of laser source (i.e., HP vs LP). The laser source was defined as LP whenever its declared power was ≤35 W. Then, patient-level data such as patient baseline characteristics (e.g., stone size and age) and perioperative variables (e.g., operative time and laser parameters) were considered. For those studies not reporting stone volume, we derived it using the spheroid formula. In case of studies reporting data on multiple groups, we considered only those groups of interest and fitting the inclusion criteria. Separated groups within the same study were treated independently during the meta-analytic process. Studies not reporting all the PICO outcomes were analyzed limitedly for available outcomes. Supplementary Table S1 displays how baseline characteristics and perioperative data were assessed in included studies.
Data analysis
A narrative synthesis of included studies was performed. Descriptive statistics were used to summarize extracted baseline characteristics data. Because of the lack of comparative studies, we decided to perform two separate meta-analytic syntheses, one for studies using LP and another one for HP generators, according to previously explained study design. 30,31 In brief, we pooled study estimates using random effects models, 32 since the meta-analytical approach we chose is a priori endowed with significant heterogeneity. 30 The I 2 statistic was used to estimate heterogeneity across studies. 31 A Wald-type test was used to compare the two separate estimates, with a significance level set at p = 0.05.
Risk of bias and level of evidence
Two reviewers (E.V. and F.P.) independently assessed the risk of bias (RoB) in individual studies. In absence of randomized control trial, the ROBINS-I tool represents the recommended bias-assessment procedure. 33 However, the ROBINS-I tool was developed for comparative observational study, which unfortunately is not available up to date according to the defined PICO. In consideration of the inherent design of this meta-analysis, we decided to precautionary assign a priori the highest possible level of bias to every included study.
Evidence Synthesis
Overall characteristics and quality of included studies
Table 1 shows the overall characteristics of included studies. No RCT was found. Except from one comparative observational study, 22 only observational noncomparative studies were selected during the systematic search process. 8 –21,23–29,34 Included studies contributed for a total of 6403 patients. The selected observational studies were heterogeneous in terms of study design, exposure assessment, selection criteria, and outcome of interest. The majority of included studies (17, 77%) were performed with an LP laser generator. Studies with HP generators were common during recent years, that is, after 2017 (4/6, 60%).
Studies Included in the Systematic Review
HP = high-power; LP = low-power.
Baseline characteristics and outcomes of interest in included studies
Table 2 reports the meta-analytic synthesis of baseline patient characteristics. No major differences were found between the HP and LP studies in terms of age at diagnosis and HU density (p > 0.05). Despite mean stone size was only marginally larger in LP studies (15.8 vs 12.9 mm, p > 0.05), estimated stone volume resulted twofold higher (2604.4 vs 1217.1 mm3, p = 0.048).
Meta-Analytic Synthesis of Patient Characteristics in the Included Studies
CIs = confidence intervals.
HP studies had shorter mean operative time (32.9 vs 62.7 minutes, p < 0.01; Fig. 2A). Pooled stone-free rate was similar in both LP and HP studies, 81% and 82%, respectively, p = 0.98 (Fig. 2B). No difference in complication rate was observed between the two groups, p = 0.12 (Fig. 2C).
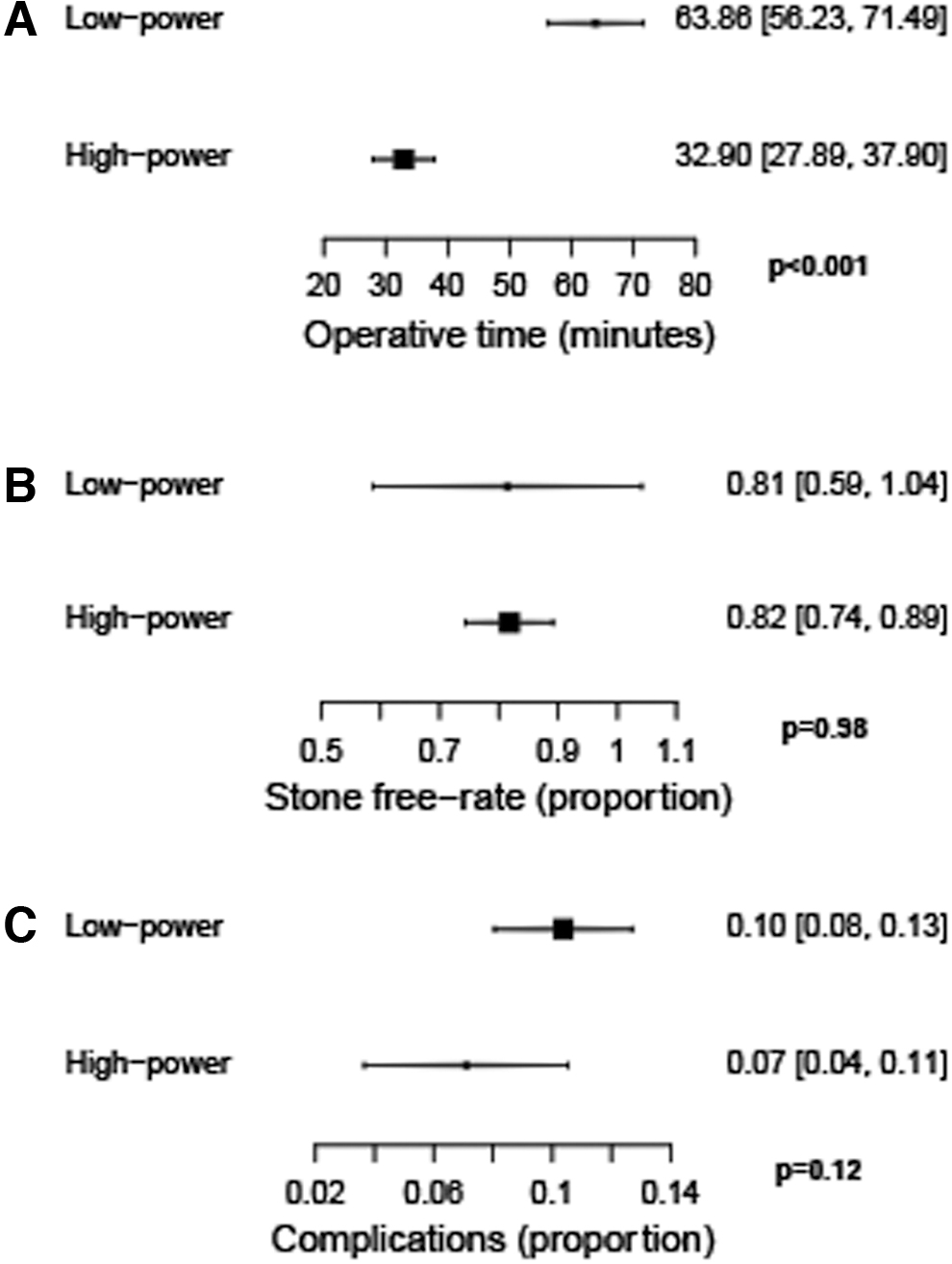
Meta-analytic outcomes of included studies.
Discussion
We performed a systematic review and meta-analysis of published studies to assess the advantage of using HP vs LP generators during ureteroscopic laser lithotripsy. Only one nonrandomized comparison was available, with the remaining studies being single-arm case series, having therefore a considerable RoB. LP lithotripsy resulted in twofold increased operative time. However, studies performed using LP laser generators included patients with significantly bigger stone volume, possibly introducing a confound factor capable of explaining this time difference. Stone-free rate was similar between the two different techniques. Because of the peculiar design of this meta-analysis, these findings should be taken cautiously.
Laser is one of the main players during intracorporeal lithotripsy, reason why the improvement of pulse delivery to the stone inevitably results in better surgical outcomes. The two main limitations of Ho:YAG laser-mediated stone ablation are the ability of producing thinner dust and working at faster speed. 35,36 Regarding the latter, HP laser generators allow to reach higher pulse repetition rates as compared with standard LP generators and may theoretically increase working speed. Thus, a 120 W laser generator, which is able to raise frequency up until 80 Hz, could lead to a fourfold reduction in laser-dependent time as compared with a standard 30 W generator, usually limited at 15–20 Hz. In laboratory-based studies, HP laser generators showed initial promising results. 37,38
Popcorning at high frequencies, that is, 80 Hz, produced smaller Begostone fragments with a shortest working time even as compared with 40 Hz in an in vitro model of renal calix 38 ; however, the authors of this study showed that a close contact should be kept with the stone when working at this speed, since at 2 mm distance four out of five laser pulses will miss the target.
Moreover, several factors of importance in the real life are not taken into account in the laboratory setting. At least three intervening factors derange the linear relationship between increased frequency and reduced operative time observed in the laboratory. First, the issue of quality of vision. The higher the frequency, the higher the motility of stones and fragments, the lower the quality of endoscopic view. Second, the issue of caliceal distensibility. Popcorning in the laboratory on a solid glass surface results in a more efficient process because of the fragments bouncing back after hitting the solid walls; however, caliceal distensible walls absorb more kinetic energy and reduce this bouncing effect. 39 Third, as a consequence, the issue of microbleedings. Hypothetically, faster popcorning speed can stochastically cause a higher number of fragments to hit the caliceal walls; this repeated microtraumatism could increase the risk of bleeding, which could further interfere with the quality of vision.
It was previously shown that HP is able to reduce laser only time by a half as compared with LP, 22 despite the possibility of having up to five times higher frequency and with an increased total amount of delivered energy. This point highlights again the issue of the efficiency in energy delivery when working at high frequencies. The extra amount of energy delivered by HP lasers ends up absorbed by the water, causing a rise in its temperature. HP lasers have been associated to dangerous increase in water temperature inside the kidney 40 –43 ; although this effect may be halted by high-flow irrigation, it is estimated that the irrigant flow needed to mitigate this effect would be so high (i.e., 300 cmH2O) to produce a rise in intrarenal pressure beyond the venous backflow threshold. 44 Intermittent laser firing 43,45 could limitate the increase in temperature, at the cost of inevitably increasing operative time and reducing then any benefits of high frequency.
Several limitations deserve to be mentioned. First, the lack of available comparative studies limits the overall level of evidence. Second, the included studies did not report the total amount of delivered energy, as well as the precise laser parameters used during the described procedures, limiting the overall appraisal of the two analyzed techniques in terms of efficiency; we believe that these data are fundamental to provide a fair comparison of HP and LP lithotripsy. Third, the heterogeneity of available reports: each study had its own way to assess the selected outcomes, rising therefore the RoB of this current report.
To the best of our knowledge, this review represents the first clinical comparison between HP and LP. Although HP laser lithotripsy appears to be noninferior to LP in terms of complications, HP did not show a clear advantage in terms of effectiveness.
Conclusions
This systematic review and meta-analysis show that HP laser lithotripsy appears to require shorter operative time, with similar stone-free and complication rates as compared with LP traditional lithotripsy. However, when taking into account stone burden, this advantage seems to be lost, or at least not to be comparable with what observed in laboratory studies. Because of the lack of high-level comparative evidence, further clinical studies are needed to elucidate the benefits of using HP laser generators during ureteroscopic stone treatment.
Footnotes
Author Disclosure Statement
Prof. Olivier Traxer is a consultant for Coloplast, Rocamed, Olympus, EMS, Boston Scientific, and IPG.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.