
Abstract
Introduction:
Cystoscopy is one of the most common procedures in outpatient urology. Although flexible cystoscopes are more tolerable, rigid cystoscopes have still been used in many clinics because of their lower costs, better visual performance, and easier handling. It can be difficult to achieve optimal relief of pain and anxiety during rigid cystoscopy. The aim of the present prospective randomized study was to evaluate the efficacy of hypnosis as an adjunct to routine local anesthesia in reducing pain and anxiety in rigid cystoscopy patients.
Materials and Methods:
Ninety male patients undergoing rigid cystoscopy for the first time were randomized into two groups: (1) Hypnosis Group (Group H) patients underwent cystoscopy with hypnotic communication as an adjuvant approach for periprocedural analgesia and anxiety, (2) Standard Care Group (Group SC) patients underwent cystoscopy with routine local anesthesia and lubrication as control group. The data were collected using visual analog scale (VAS) for pain, State-Trait Anxiety Inventory (STAI) for anxiety and hemodynamic parameters. Furthermore, a VAS was also completed by the urologist to assess his satisfaction.
Results:
Baseline characteristics, STAI, hemodynamic parameters, and recovery duration were statistically similar between the two groups. The procedure duration was shorter in Group H (p = 0.018). The postprocedural STAI and VAS scores of patients in Group H were significantly lower than those of Group SC (p = 0.006; p = 0.02, respectively). Heart rate and mean arterial pressure after positioning of the patient (p = 0.000; p = 0.004, respectively) and insertion of the cystoscope (p = 0.000; p = 0.000) were statistically lower in Group H, whereas baseline, postprocedural, and predischarge hemodynamic measurements were similar. Urologists were also more satisfied in Group H (p = 0.000).
Conclusion:
Hypnosis as an adjunct therapy to local anesthesia during rigid cystoscopy significantly reduces pain and anxiety, provides more stable hemodynamic conditions, shortens procedure duration, and thus appears attractive for pain and anxiety management.
Introduction
Cystoscopy, which is an outpatient procedure and essential diagnostic tool in urology, is commonly performed for bladder cancer detection and its follow-up. Of the two types of cystoscope, rigid and flexible, rigid cystoscopy is more invasive and, therefore, causes more discomfort. 1 Despite this, it still remains common in Turkey owing to its lower cost, more easy handling, and improved better visual performance. Consequently, relief of the pain and anxiety associated with rigid cystoscopy gains importance.
Hypnosis has an established tradition of reducing pain and emotional distress in so much that it was a popular anesthetic technique in surgical patients before the invention of chemical anesthesia. 2 Although the availability of chemical anesthetic and sedative agents in the 18th century reduced the use of hypnotism in surgery; clinical hypnotherapy and other psychologic interventions, such as psychoeducation and relaxation techniques, have been regaining popularity in the reduction of anxiety and pain in surgical and invasive procedure patients in the past years. 2 –4 Clinical hypnosis can be used as a stand-alone intervention or as an adjunct to usual anesthetic or sedative techniques.
Various anesthetic and anxiolytic approaches have been used to relieve urethral pain and anxiety about the pain during rigid cystoscopy. 5 –7 However, some of these approaches may be insufficient, whereas pharmacologic treatments can bring undesirable side effects, increased costs, and hospitalization times. Hypnosis is an effective, safe, noninvasive, and inexpensive tool for reducing the anxiety or pain, which can also be used as an adjunct to standard care. 2 This study was designed to investigate the hemodynamic and anxiolytic effects of hypnosis, as an adjunct to local anesthesia, which is standard care in our outpatient cystoscopy center, as well as its impact on patient and urologist satisfaction in rigid cystoscopy patients.
Materials and Methods
Patients
This prospective study was approved by the Numune Education and Research Hospital Ethical Committee and participants provided informed consent. Consolidated Standards of Reporting Trials (CONSORT) statement 2001 checklist items for randomized controlled study were used. The trial was conducted from July 2018 to January 2019. Adult male Turkish speaking patients with an American Society of Anesthesiologist Physical Status I − II and between the ages 18 and 78 years, undergoing rigid cystoscopy under local anesthesia at the outpatient cystoscopy center of Turkey Yüksek Ihtisas Education and Research Hospital were enrolled. In this center, complicated cystoscopy examinations were ceased and planned to be performed in operating room under sedation or general anesthesia. Patients were eligible for inclusion if they underwent rigid cystoscopy for the first time. Exclusion criteria for the patients were (1) a history of central nervous system disease, (2) treatment with analgesic or psychotropic medication, and (3) a major affective disorder or other psychiatric diagnosis. Computer-generated randomization was performed and patients were divided into two groups: (1) Hypnosis Group (Group H) patients underwent cystoscopy after a single hypnosis session as an adjuvant approach for periprocedural analgesia and anxiety, (2) Standard Care Group (Group SC) patients underwent cystoscopy with routine local anesthesia and lubrication and were used as control group.
Study protocol
A single hypnotherapist performed the hypnotic sessions who is certificated by Yıldırım Beyazıt University GETAT Education Center. Anxiety score assessments were carried out by another single experienced physician, who was not involved in the other processes. Chronologically, this investigator established contact with the patient before entering the cystoscopy room, evaluated the anxiety of the patient according to the State-Trait Anxiety Inventory (STAI) test (STAI-1). A hypnotic relaxation session with the hypnotic group patients was directed by the hypnotherapist immediately after the test. To eliminate the placebo effect of hypnosis, the same hypnotherapist had an interview with patients of Group SC for a similar period of time. This interview consists of information about the procedure and discharge conditions. Both the hypnosis and interview sessions were delivered to patients individually by the same therapist and were standardized to last 15 minutes. To set a single-blind design (for the urologist performing the cystoscopy), the STAI test and hypnotic session were performed in a separate room 10 minutes before the cystoscopy procedure. Demographic details and education levels of all patients were queried and recorded.
Cystoscopy was performed under direct vision by urologists familiar with the examination with rigid cystoscope (company Olympus; French: 17.7), in an outpatient setting, in a cystoscopy room. The patients were placed in the dorsolithotomy position with legs suspended in stirrups. A triple disinfection of the external genitalia with antiseptics and application of a lubricant containing 2% lidocaine with a minimum dwell time of 3 minutes were obligatory. After completion of the procedure, patients were transferred to the recovery room. Heart rate and noninvasive blood pressure were recorded at baseline, before filling out the STAI (T1); after the positioning of the patient (T2), after insertion of the cystoscope into the urethra of the patient (T3); at the end of the procedure (T4) and before the discharge of the patient, in the recovery room (T5). The treatment algorithm of the study is shown in Figure 1.
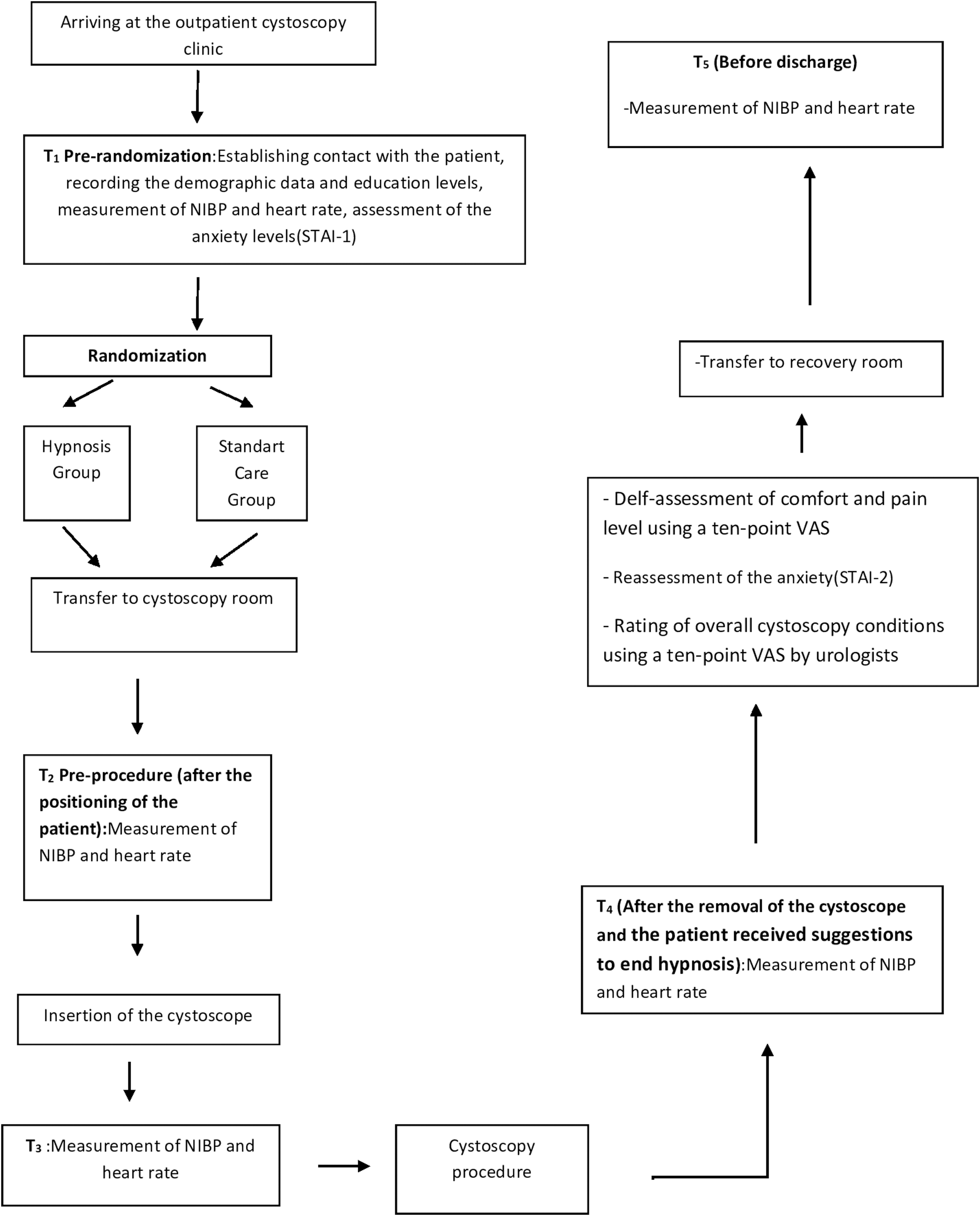
Study treatment algorithm. VAS = visual analog scale.
Immediately after the procedure, the patients were asked to rate their pain level using a 10-point visual linear analog scale (VAS; 0 = no pain, 10 = maximal pain). Anxiety levels were also remeasured (STAI-2). A 10-mm-long VAS was also completed by six different urologists who were blinded to the groups to assess the overall conditions for each cystoscopy (0 = impossible conditions, 10 = very good conditions). The duration of the procedure and recovery period were recorded in each case. Complete recovery was defined as a pain score of 0, no functional limitation, and resuming of normal activities. The cystoscopy findings were revealed to the patient after the patient's study data had been collected.
Hypnotic technique
After informing patients about the hypnosis procedure, hypnotic induction began once the subject was seated in a comfortable chair. The patient was focused on slow and monotone voice of the hypnotherapist. Induction was performed using the eye fixation technique. A breathing technique was then used to induce a progressively deeper hypnotic state. This involved giving suggestions to the patient of anxiety fear control and relaxation while slowly counting to 20 in time with inspiration. The patient could express any discomfort using a predefined code. A hypnotic trance was considered to have been achieved when the hypnotherapist noted muscular relaxation and regular breathing. Subsequently, patients were asked to use visual imagery, which utilizes a pleasurable and relaxing experience. Suggestions were made for the patient's external genitalia to lose sensation on the skin and the subepidermal tissues. Patients were also suggested to tolerate the feelings evoked by the insertion of the cystoscope. At the end of the procedure (removal of the cystoscope), the patient received suggestions to end hypnosis.
Statistical analysis
All statistical analyses were carried out using SPSS 20 for Windows (IBM, 2011). Number, percentages, means, standard deviations, medians, and minimum and maximum values were used for descriptive statistics of the study. Demographic comparisons of the two groups were conducted using a chi-square analysis for categorical variables and independent t-tests for continuous variables. The distribution of the data was tested with the Kolmogorov–Smirnoff test. Moreover, skewness and kurtosis were calculated and both should be <1 to use parametric tests. 8 Normally distributed data were tested using the parametric Student's t-test and data not normally distributed by the nonparametric Mann–Whitney U test. Two tailed tests were used and p < 0.05 was regarded as being statistically significant.
Results
One hundred nine consecutive patients were evaluated for possible inclusion to the study; 7 patients were excluded because they were not fluent in Turkish, 7 patients were excluded because they were suffering from a psychiatric or central nervous system disorder, and 5 patients were excluded because they refused to participate in the study. Hence, the final sample for the study was 90 patients. These patients were randomized into two groups (Fig. 2). There were no significant differences between the two groups regarding age, gender, body weight, height, educational status, existence of comorbidities, and duration of the recovery period. Duration of the procedure was significantly shorter in the Hypnosis Group (Table 1). Baseline mean arterial pressure (MAP), heart rate, and STAI-1 evaluations did not also differ significantly between the two groups (Table 2).
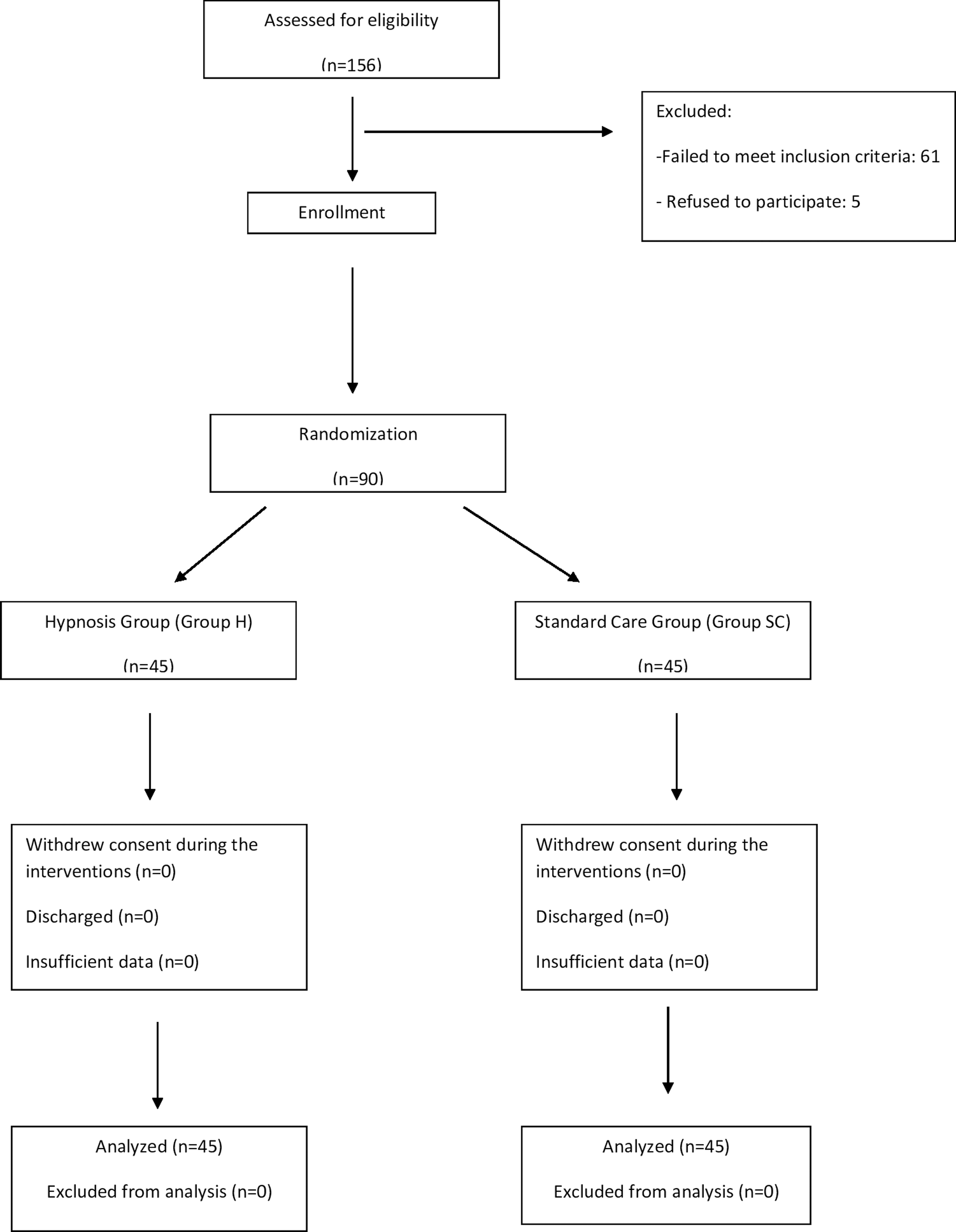
Flow diagram of the study.
Pre- and Perioperative Data of Groups
Values expressed as mean ± SD (median; min–max) or n (%).
Group H = Hypnosis+Standard Care Group; Group SC = Standard Care Group.
Comparison of Anxiety and Visual Analog Scale Scores, Hemodynamic Parameters Between Groups
Values expressed as mean ± SD (median; min–max).
Measurement time points: Baseline, T1; after the positioning of the patient, T2; after insertion of the cystoscope into the urethra of the patient, T3; at the end of the procedure, T4; before the discharge of the patient, T5.
Group H = Hypnosis+Standard Care Group; Group SC = Standard Care Group; HR = heart rate; MAP = mean arterial pressure; STAI = State-Trait Anxiety Inventory.
MAP and heart rate were significantly lower in Group H than in Group SC after the positioning of the patient (T2) and insertion of the cystoscope into the urethra of the patient (T3). These two measurements did not differ between the groups at the end of the procedure (T4) and before the discharge of the patient (T5). There was a significant difference between two groups in the second evaluation of STAI. Anxiety level of Group H was better than that of Group SC. VAS score, which aimed to measure pain level of patients, was significantly higher in Group SC than in Group H, whereas VAS score, which aimed to measure satisfaction of the urologists about the overall conditions for cystoscopy, was higher in Group H than in Group SC (Table 2).
Discussion
The results of this randomized controlled trial revealed that a brief hypnosis intervention can be an effective means to reduce pain and anxiety in patients undergoing rigid cystoscopy. Pain and anxiety were reduced and a better hemodynamic stability was maintained in patients receiving hypnosis relative to a standard care control group. Urologists were also more satisfied with the cystoscopy conditions provided by adjunct hypnotherapy.
Hypnosis can be defined as an induction that usually consists of an initial suggestion for using the subject's imagination or an invitation to focus the subject's attention followed by a set of suggestions. These motivational suggestions generally aim to change the subjective experience, perception, sensation, emotion, thought, or behavior. Pain and anxiety management is one of the instances that hypnosis has been used effectively. 9 Elliotson (1791–1868) was the first reporter who used hypnosis for pain management, as an effective anesthetic during surgery. 10 During the following years, it was used in treating the pain associated with the medical procedures such as bone marrow aspiration, lumbar puncture, burn debridement or other burn care, surgical procedures, abortion, venipuncture, radiologic procedures, and angioplasty. 11 –18 To our knowledge, this is the first report about the use of hypnosis for pain and anxiety management associated with rigid cystoscopy.
Cystoscopy is one of the most commonly used outpatient procedures in urology clinics. It was first introduced in the field of urology in 1805 by Bozzini and since then with the various technological advances, flexible cystoscopes have been among the most utilized techniques in the urologist's armamentarium. 19 However, rigid cystoscopes are still frequently used in developing world for outpatient cystoscopy, because of their lower cost, better optical area, and easier handling. 20 –22 Various approaches such as topical urethral analgesia, dorsal penile nerve block, sedation, and listening music therapy have been used to make this procedure more tolerable for patients. 5 –7,23
Our results suggest that in rigid cystoscopy patients, hypnosis was effective in reducing anxiety and pain as measured by STAI and VAS, respectively, along with physiologic measures such as MAP and heart rate. This observation accords well with the likelihood that the anxiety and pain are often associated, providing a vicious cycle between the two. Hypnosis has a dual role in pain and anxiety reduction, probably leading to break this cycle. The urologists in our study were also more satisfied with adjunct hypnotherapy compared with sole local anesthesia, probably because of better patient tolerance associated with lower anxiety and pain levels.
Although our study was not designed to evaluate costs, our finding that hypnosis significantly reduces the duration of the procedure may be an indication of lower costs. Lang et al. reported similar results in their two different studies about cost analysis of adjunct hypnosis with sedation during outpatient interventional radiologic procedures and outpatient large core breast biopsy. They showed that shorter room times reduces costs effectively because of equipment amortization and personnel cost based on local salaries. 24,25 However, a potential drawback of hypnotherapy is the cost and availability of a skilled hypnotherapist. Further studies are needed to evaluate cost-effectiveness of adjunct hypnotherapy in rigid cystoscopy patients.
The effect of hypnosis was examined in adults undergoing surgical and painful medical procedures as well as in patients suffering from chronic pain by several meta-analysis and reviews. Tefikow et al. underlined the limited number of randomized controlled trials on the beneficial effects of hypnosis in patients undergoing medical and surgical procedures in their meta-analysis published in 2013. 2 With the growing data from randomized controlled clinical trials, Kendrick and colleagues concluded that hypnosis decreases acute procedural pain and seems to be especially effective in minor surgical procedures. 4 Furthermore, researches demonstrate that hypnosis has direct effects on the supraspinal areas that are linked to the experience of pain. 26 Hypnosis has also been shown to be beneficial as an adjunct intervention to reduce anxiety in patients undergoing dental procedures and cancer patients. 11,14,27
Our study had some limitations such as the subjectivity of the pain. Pain was most often measured with a single VAS score in similar hypnosis studies. This scale is easy to administer and has low time-cost from the respondents. Besides this, physiologic measures such as MAP and heart rate also support the significant difference of VAS scores between groups. MAP and heart rate of the patients in Group H were more stable than those in the Group SC. Another possible limitation of our study is the absence of a third group that had no interview with hypnotherapist. As because patients are already informed by the urologist in our routine practice, we do not perceive this as a real limitation.
Conclusion
In conclusion, the results of this study suggest that the use of hypnosis before rigid cystoscopy as an adjunct therapy to local anesthesia can be considered a brief, easily implemented, and an effective intervention in reducing pain and anxiety, leading to more satisfied patients and urologists.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.