
Abstract
Introduction:
Despite proven effectiveness of medications in preventing stone recurrence, compliance with pharmacotherapy (PT) is often poor because of cost, side effects, and impact on lifestyle. We sought to compare the risk of stone recurrence between patients managed with conservative therapy (CT) vs PT controlling for aggressiveness of stone disease.
Materials and Methods:
The Multi-center collaboration to Study Treatment Outcomes in Nephrolithiasis Evaluation (MSTONE) database contains patient data and outcomes from July 2001 to April 2015 across four centers. The database was queried for patients whose stone disease was managed with CT alone (fluid and dietary recommendations) vs PT. Patients were risk stratified according to number of previous passed stones. Within each risk group, we compared CT vs PT with respect to 2-year stone event rate and stone event-free survival (SEFS) using the Kaplan–Meier method.
Results:
A total of 245 patients, with a median follow-up of 29 months (interquartile range = 16–44), were identified, including 93 on CT and 152 on PT. The overall 2-year stone event rate was 38% for all patients. Stone events at 2 years occurred less frequently in the PT group compared with the CT group (31% vs 44%, p = 0.043), with the difference most pronounced in the high-risk group (71% vs 32% for CT and PT, respectively, p = 0.058). The 30-month SEFS was significantly higher for PT (58%) than CT (46%) overall. When stratified by risk group, 30-month SEFS was statistically significantly higher for PT than CT in the intermediate risk group (65% vs 45% for PT and CT, respectively).
Conclusion:
Controlling for aggressiveness of stone disease, PT was more effective than CT in reducing and delaying stone-related events. However, CT appeared to be as effective as PT in low-risk patients. PT is best reserved for recurrent stone formers, regardless of metabolic background.
Introduction
The prevalence of self-reported stone disease in US adults has risen steadily over the past several decades. A published population level data show the current estimated prevalence of stone disease in US adults is 8.8%. 1 For those patients who have a symptomatic stone event, the 5-year recurrence rate without specific treatment has been shown to be as high as 53%. 2,3
Although the surgical management of stones has evolved to almost exclusively minimally invasive procedures with relatively low morbidity, the ultimate goal was prevention of stone recurrence in an effort to minimize the burden to patients and the health care system.
Both the American Urological Association (AUA) and the European Association of Urology (EAU) recommend that recurrent stone formers and first-time stone formers with risk factors for recurrent stone disease undergo metabolic testing, the cornerstone of which is the 24-hour urine collection. 4,5 Identifying and correcting metabolic abnormalities with pharmacotherapy (PT) has resulted in a decrease in the rate of stone recurrence and can be a potentially cost-effective strategy. 6 –8 However, the 24-hour urine collection is imperfect in predicting stone recurrence, stone composition, or responses to treatment. 9 Medications have side effects and inherent costs, and consequently, a conservative approach of dietary changes and increased fluid intake is often initially attempted. In addition, in Americans at high risk of stone recurrence, the prevalence of testing is only 7%. 10
The Multi-center collaboration to Study Treatment Outcomes in Nephrolithiasis Evaluation (MSTONE) was initiated to assess medical management practices and outcomes in tertiary care stone centers. We sought to compare the risk of stone recurrence in patients managed with initial conservative therapy (CT) vs those managed with PT while controlling for aggressiveness of stone disease.
Materials and Methods
Institutional review board approval and data transfer agreements were obtained from each of the four large, tertiary care stone clinics in the United States (Dallas, TX; Madison, WI; Iowa City, IA; and Nashville, TN). A database was retrospectively constructed that contains patient demographics, management data, and outcomes for patients seen between July 2001 and April 2015 across the four centers.
A retrospective chart review was performed to identify patients who had at least 3 months of follow-up and clear documentation of medical management, outcomes, and previous stone episodes. Details of follow-up of eligible patients from presentation to the stone clinic to last follow-up included dietary recommendations (dietary restriction of salt, protein, and/or oxalate, increase in fruits and vegetables) and stone preventative medications prescribed (potassium citrate, sodium bicarbonate, thiazide, allopurinol, calcium supplement, pyridoxine). In addition, radiographic imaging for stone diagnosis, emergency room visits, and surgical interventions during follow-up were noted.
The database was queried for patients whose stone disease was managed with either CT alone (fluid and dietary recommendations) or PT. Stone events (new stone formation, stone growth, or an acute stone episode) were recorded. Patients were risk stratified according to number of previous stones spontaneously passed (low risk = 0, moderate risk ≤10, and high risk ≥10 previous stone episodes). For the purposes of this initial study, a 24-hour urine collection was not a requisite for inclusion.
Patients with anatomic abnormalities that predispose to stone formation (horseshoe kidney, ectopic kidney, UPJ obstruction, calyceal diverticula, and stenotic infundibulum), primary hyperparathyroidism, primary hyperoxaluria, distal renal tubular acidosis, cystinuria, and bowel segments in continuity with the genitourinary tract (ileal ureter, ileal conduit, and neobladder) were excluded from this study.
Within each risk group, we compared patients managed with CT with those managed with PT with respect to rate of stone events and stone event-free survival (SEFS) using the Kaplan–Meier method. Events after the first stone recurrence were censored. A stone recurrence was defined as symptoms or operation related to a preexisting stone or radiographic progression of stones by number (new stone >2 mm) or size (growth of an existing stone by >2 mm). Events that occurred within 3 months of the initial visit or within 6 weeks of initiation of therapy were censored, as they were unlikely to have been influenced by treatment. Patients managed with PT at any point during the follow-up period were placed in the PT group. For those that had 24-hour urine data, the incidence of low total urine volume (TV) (<2 L), hypercalciuria (>250 mg/TV), hypocitraturia (<320 mg/TV), hyperoxaluria (>40 mg/TV), hyperuricosuria (>700 mg/TV) was calculated. This 24-hour urine collection was taken before initiation of PT.
Comparisons between groups for categorical variables used chi-square test. For continuous variables, analysis of variance was used to compare the three risk groups. Time to occurrence of the first stone event, analyzed by Kaplan–Meier analysis, was compared with the log-rank test. Continuous variables are summarized as median and interquartile range unless otherwise specified. A two-sided p ≤ 0.05 was considered significant. Statistical analysis was performed with SPSS version 14 (IBM, Armonk, New York).
Results
A total of 245 patients with a median follow-up of 29 months (interquartile range [IQR] = 16–44) met the inclusion criteria and were included in the study group. Among these patients, 93 were managed conservatively (CT) and 152 were managed with PT with or without dietary measures. Age, gender, ethnicity, BMI, and duration of follow-up were similar between the two groups (Table 1). Patients were categorized as low risk (62 patients, 25%), intermediate risk (147 patients, 60%), and high risk (36 patients, 15%) according to the number of previous episodes of stone passage. Stratification of each treatment group according to risk is given in Table 1. Higher risk patients were more likely to receive PT (78% vs 22%, respectively; p = 0.012).
Demographical Information, Risk Stratification, and Baseline 24-Hour Urine Data
Values in bold denote statistical significance.
BMI = body mass index; IQR = interquartile range; TV, total urine volume.
Baseline 24 U data was available for 235 of the 245 patients. There was a statistically significant increased incidence in hypercalciuria and hypocitraturia in patients who would go on to have PT (Table 1). Median (IQR) number of surgeries in the entire cohort was 2 (1–4). Higher risk group was associated with an increasing number of life-time stone surgeries (one IQR = 0–3, two IQR = 1–3, four IQR = 2–5, for low, intermediate, and high risk, respectively, p < 0.001; Table 2).
Stone Event Outcome Based on Stone Risk Category
Values in bold denote statistical significance.
CT = conservative therapy; PT = pharmacotherapy.
The overall 2-year stone event rate for all patients was 38% at a median follow-up of 29 months (IQR = 16–45). Stone events occurred less frequently in the PT group compared with the CT group at 2 years (44% vs 31%, respectively, p = 0.043; Table 2). The high-risk group trended toward the largest reduction in 2-year stone event rate (71% vs 32% for CT and PT, respectively, p = 0.058). PT had the smallest impact in the low-risk group for 2-year stone event rate (43% vs 30% for CT and PT, respectively, p = 0.284).
Overall 30-month SEFS was significantly higher for PT (58%) than CT (46%) (p = 0.006; Fig. 1). When stratified by risk group, 30-month SEFS was significantly higher for PT than CT in the intermediate risk group (65% vs 45%, respectively, p = 0.005) and trended toward a significant improvement with PT in the high-risk group (49% vs 17%, respectively, p = 0.099). No significant difference in SEFS was detected in the low-risk group.
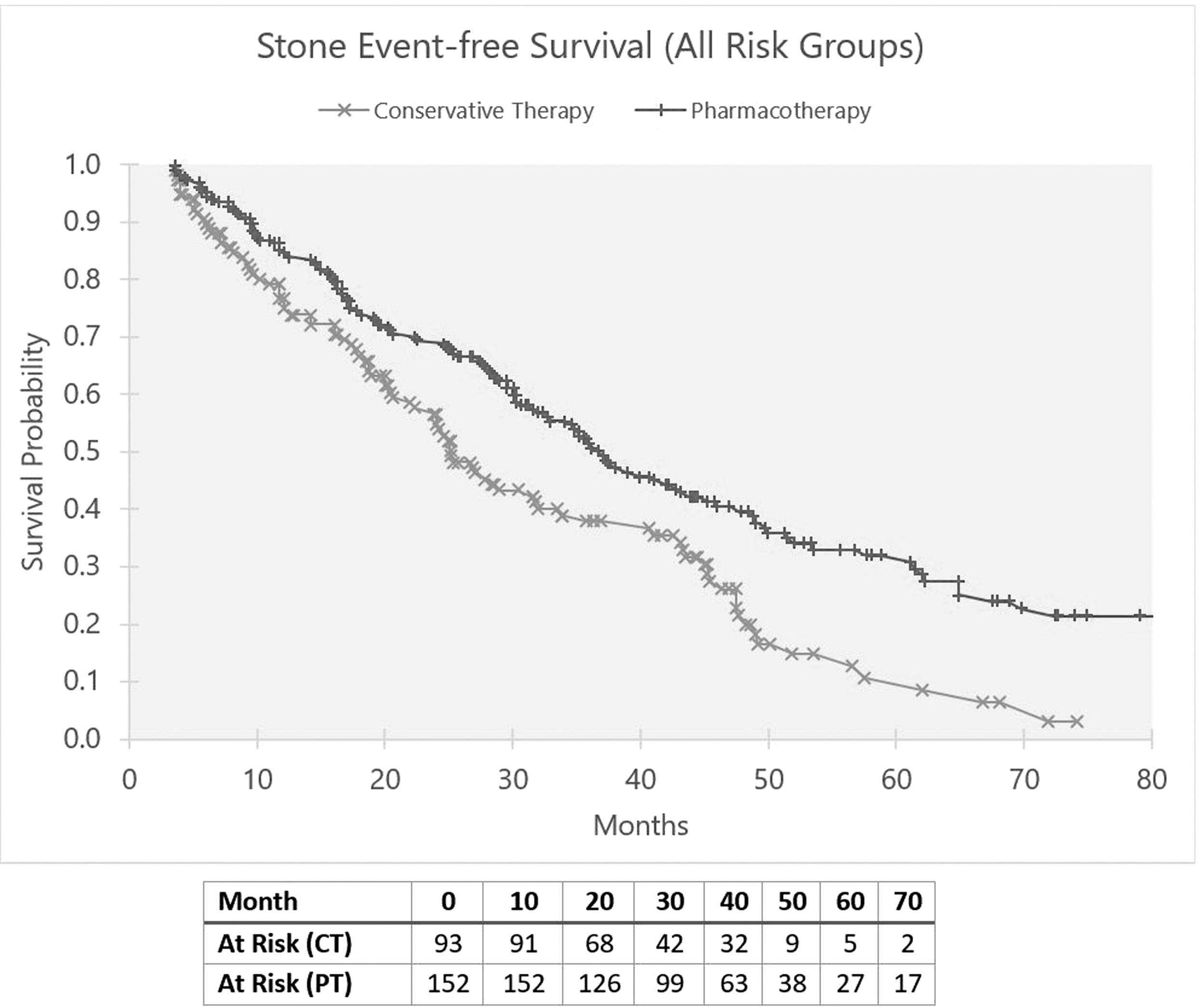
Kaplan–Meier analysis of stone event-free survival for all groups. Log-rank test demonstrated pharmacotherapy conferred an improved stone event-free survival, p = 0.043.
Discussion
Efforts to reduce stone recurrence are aimed at altering the urinary environment to lower urinary saturation of stone-forming salts. Metabolic testing with serum chemistries and 24-hour urine analysis identify abnormalities that can be targeted for dietary modification or PT. Dietary measures for stone prevention include aggressive hydration, reduction of salt and animal protein, consuming normal, but not excessive calcium, and limiting intake of oxalate-rich foods. Drug therapy includes thiazide diuretics for hypercalciuria, potassium citrate for low urine pH and/or hypocitraturia, and allopurinol for hyperuricosuria not responsive to dietary measures. 4 Although the value of 24-hour urine testing has recently been brought into question, the benefit of dietary measures and PT has been consistently demonstrated. 9,11,12
Our study examines data from four high-volume tertiary care centers with Endourological Society fellowship-trained urologists experienced in medical stone management. Although most patients included in our study underwent metabolic testing with one or more 24-hour urine analyses, urine collection was not a prerequisite for inclusion in this study. Our aim was to establish intermediate outcomes of medical stone management while controlling for stone aggressiveness indicated by previous stone episodes, a metric that correlated closely with the number of previous stone surgeries. With a median follow-up of 29 months, the initiation of drug therapy was associated with a statistically significant decrease in 2-year stone event rate. The reduced stone event rate overall can be accounted for primarily by a benefit of therapy in intermediate and high-risk patients. Kaplan–Meier analysis also demonstrated that for high-risk patients, PT delayed the occurrence of a stone event by a little over 1 year. No added benefit of PT over dietary measures was demonstrated for low-risk patients, perhaps because dietary measures are sufficient for these patients.
Dietary modification has been shown to reduce stone recurrence rates. 13,14 Indeed, the “stone clinic effect” describes the benefit of dietary measures seen in the placebo control arms of PT trials on which the AUA and EAU guidelines are based, which show a 0%–61% decrease in stone recurrence rates and a 20%–86% remission rate. 4 Most patients on PT are also advised to adhere to dietary measures, and thus the benefit of drug therapy can only be determined by comparison with a control group on dietary measures alone.
Although the AUA recommends selective medical therapy based on metabolic testing, compliance with drug therapy is only ∼50%. Reasons for noncompliance include cost, potassium citrate pill quantity, and adverse drug effects of thiazide diuretics. 15 Our study did not address or assess rates of patient noncompliance, although we assume noncompliance affected our patient population as well.
Our findings are consistent with a recent systematic analysis of 21 randomized controlled trials comprising 2168 participants that found that drug therapy was more effective than dietary therapy in preventing stone recurrence among recurrent idiopathic calcium stone formers. 16 Like our study, the meta-analysis found that the benefit of PT was apparent only among patients with two or more previous stone episodes.
Our study has several strengths, including the involvement of multiple sites, geographically varied patient populations and a relatively large, well-characterized cohort with intermediate-to-long-term follow-up. Although we included baseline 24-hour urine collection data, we did not analyze how those values evolved over the course of treatment or how they were used to guide initial therapy. Likewise, we did not use 24-hour urine analysis in our risk stratification given its complexity. This prevented stratification by severity of metabolic abnormalities and assessment of the success of therapy in correcting urinary abnormalities. We hope to perform a prospective evaluation in which the severity of disease, as determined by pretreatment stone events and analysis of baseline 24-hour urine collections, can be correlated with response to dietary and drug therapy from both a urine chemistry perspective and actual stone event/progression. In that analysis, we might be able to identify subgroups of patients who would benefit the most from PT vs dietary measures alone. Finally, patient compliance with medication and dietary recommendations were not verified, and consequently we cannot be certain that the outcomes are attributable to the treatment initiated.
These limitations notwithstanding, our results are intriguing. If it can be established that low-risk patients are effectively managed with conservative measures, then medications might be reserved for high-risk, aggressive stone formers. On the contrary, intermediate and high-risk patients appear to benefit from PT and this should be the preferred approach if our findings are validated. Further risk stratification could improve identification of higher risk cohorts.
Conclusions
Overall recurrence rates in our multicenter cohort were high for both CT and PT. However, PT was more effective in reducing and delaying stone-related events, particularly among high-risk stone formers. Low-risk stones formers may be managed by dietary measures alone when all factors are weighed. For those with aggressive stone disease, PT is effective in delaying the onset of recurrent stone events by over a year. There is also a role for selective medical management in high-risk patients. As our data were limited by absence of complete 24-hour urine data and subsequent stratification by metabolic abnormalities, further studies are needed to identify which patients might benefit the most from aggressive medical management.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.