
Abstract
Background:
Minimally invasive cystectomy is being increasingly performed, however, data comparing laparoscopic radical cystectomy (LRC) and robotic radical cystectomy (RRC) are scarce. We compared 30- and 90-day Clavien–Dindo Classification (CDC) complications between patients undergoing LRC and RRC at our center.
Materials and Methods:
We retrospectively evaluated 300 patients who underwent minimally invasive radical cystectomy from January 2007 to July 2019 and grouped them into LRC (112 patients) and RRC (188 patients). We compared the two groups for demographic variables, perioperative characteristics, and 30- and 90-day CDC overall, minor, and major complications. Multivariable logistic regression analysis was performed to identify variables that predict perioperative complications.
Results:
The two groups were comparable for the duration of surgery (270 minutes in LRC vs 265 minutes in RRC) and rate of conversion to open surgery. The RRC cohort had a higher estimated blood loss (EBL) (675 mL vs 500 mL, p = 0.006), but the two groups had a comparable need for intraoperative transfusion. Patients undergoing RRC also had a shorter duration of hospital stay (13 days vs 14 days, p < 0.001). There was no difference between the two groups for 30- and 90-day CDC overall, minor, and major complications. The incidence of rehospitalization within 30 days (p = 0.1) and surgical reintervention (p = 0.5) was also comparable between the two groups. On multivariable logistic regression analysis, approach to cystectomy (RRC vs LRC) was not a significant predictor of 30-day CDC overall and major complications.
Conclusion:
LRC was associated with lesser EBL, whereas the hospital stay was shorter in patients undergoing RRC. The two approaches were comparable with each other for 30- and 90-day CDC overall, minor, and major complications. The choice between the two approaches should depend on availability and surgeon experience and preference, rather than any specific perioperative parameter.
Introduction
Bladder cancer (BCa) accounts for ∼7% of all malignancies and represents a huge oncologic and economic burden. 1 Around 25% to 30% of these patients present with muscle invasive bladder cancer (MIBC). 2 Radical cystectomy (RC) with bilateral pelvic lymph node dissection (PLND), after neoadjuvant chemotherapy (NAC), is the standard of care for nonmetastatic MIBC and recurrent high-risk nonmuscle invasive bladder cancer (NMIBC). 3 Open radical cystectomy (ORC) has been the most commonly used approach with robust data available on feasibility, complications, and oncologic outcomes. However, there is significant perioperative morbidity associated with ORC with 30- and 90-day overall Clavien–Dindo Classification (CDC) complication rates ranging from 30% to 60%. 4 –6
To circumvent some of the complications of this extensively extirpative surgery, minimally invasive RC was described. However, laparoscopic radical cystectomy (LRC) with PLND is a technically challenging procedure and large series have mainly been reported from high-volume centers with experienced surgeons. 7 –10 Although robotic radical cystectomy (RRC) remains a technically demanding surgery, the robotic system offers much better ergonomics and a shorter learning curve than LRC. Consequently, there have been numerous series reported for RRC worldwide. 11 –13
Multiple systematic reviews have been published comparing ORC with LRC or RRC. 14 –18 Few reports directly compare the outcomes of LRC with RRC. 19 –22 At our high-volume oncology center, we offer LRC and RRC to our patients with BCa. In this retrospective study, we sought to assess the perioperative CDC complications in our patients with LRC and RRC and determine whether either modality was better than the other. Secondary objectives included evaluating predictors of overall and major CDC complications, and analyzing the trend in performing LRC or RRC at our center over the past decade.
Materials and Methods
Population
The study was approved by the institutional review board. We searched a prospectively maintained institutional RC registry for clinically nonmetastatic BCa. From January 2007 to July 2019, 305 patients underwent RC for nonmetastatic
Data were collected for age, gender, height, weight, body mass index (BMI), American Society of Anesthesiologists (ASA) score, age-adjusted Charlson's Comorbidity Index (ACCI), and whether NAC was received (for patients undergoing RC for urothelial MIBC). We also noted the duration of surgery, estimated blood loss (EBL), need for intraoperative blood transfusion, duration of catheterization (in patients undergoing neobladder diversion), length of hospital stay, need for rehospitalization, surgical reintervention, histologic type of malignancy, pathologic T and N stages, carcinoma in situ, and margin positivity. We collected data for 30- and 90-day complications. All complications were graded as per the CDC system and grouped into minor (CDC I and II) and major (CDC ≥III). 23 Complications were also classified according to organ systems.
Male patients underwent either a radical cystoprostatectomy or a prostate-sparing cystectomy. 24 Female patients underwent an anterior pelvic exenteration. All patients underwent a bilateral PLND. Up to 2011, patients underwent a “standard” PLND limited by the common iliac bifurcation superiorly, Cooper's ligament inferiorly, genitofemoral nerve laterally, and obturator nerve medially. From 2012 onward, an extended PLND was performed with its cranial limit being the aortic bifurcation.
Our techniques of LRC and RRC have been previously described. 8,25 From 2008 to 2011, RRC was performed with the da Vinci S-HD robotic system (Intuitive Surgical, Inc., Mountain View, CA). Then in 2011, we changed for the da Vinci Si platform, which is the system that has been in use since then. The procedures were performed by one of seven surgeons. Every surgeon was fellowship trained and with sound experience in minimally invasive uro-oncologic procedures. Any conversion to open surgery was noted along with the reason for the same.
Statistical analyses
The unpaired “t” test, Mann–Whitney U test, and chi-square test were used to compare the statistical significance of differences in means, medians, and proportions, respectively. Univariable and multivariable logistic regression analyses tested the impact of perioperative variables in predicting the occurrence of overall and major CDC complications. Statistical significance was considered at p < 0.05. Statistical analyses were performed using SPSS v.20.0 software (IBM SPSS Statistics, IBM Corporation, Armonk, NY).
Results
Preoperative characteristics
The two groups were similar in terms of patient age, gender, BMI, and the proportion of patients undergoing RC for high-risk NMIBC and MIBC (Table 1). Patients undergoing RRC had a higher ASA score (p < 0.001), higher ACCI (p = 0.016), and a higher proportion of use of NAC (77% vs 51%, p < 0.001) than those undergoing LRC.
Preoperative Characteristics of 300 Patients Who Underwent Minimally Invasive Radical Cystectomy with Pelvic Lymph Node Dissection from January 2007 to July 2019
The bold values signify that the p value for that variable is significant.
ACCI = age-adjusted Charlson's comorbidity index; ASA = American Society of Anesthesiologists; BCa = bladder cancer; BMI = body mass index; IQR = interquartile range; LRC = laparoscopic radical cystectomy; MIBC = muscle invasive bladder cancer; NAC = neoadjuvant chemotherapy; NMIBC = nonmuscle invasive bladder cancer; RRC = robotic radical cystectomy; SD = standard deviation.
Intraoperative variables and pathologic findings
Conversion to open surgery was required in five patients in each group (Table 2). The reasons for conversion included interbowel adhesions (four cases), common iliac vein injury (three cases), internal iliac artery injury (one case), rectal injury (one case), and fixed bladder mass with large lymph nodes (one case). There was no statistically significant difference between the two groups for the median duration of surgery (270 minutes in LRC vs 265 minutes in RRC), proportion of patients undergoing PLND, need for intraoperative blood transfusion (30% in LRC vs 42% in RRC, p = 0.052), and the rate of margin positivity (8% in LRC and 7.4% in RRC, p = 0.8). The RRC cohort was associated with a higher median EBL of 675 mL compared with 500 mL in the LRC cohort (p = 0.006).
Intraoperative Characteristics and Histopathologic Findings of 300 Patients Who Underwent Minimally Invasive Radical Cystectomy from January 2007 to July 2019
The bold value signifies that the p value for that variable is significant.
CIS = carcinoma in situ; EBL = estimated blood loss.
Postoperative course and complications
The median duration of hospitalization in the RRC group was significantly shorter (13 days vs 14 days, p < 0.001) (Table 3). Sixty percent of the patients had at least one complication at 30 days and the incidence of CDC overall complications was not significantly different in the two groups (57% vs 62%, p = 0.3).
Perioperative Complications and Postoperative Course of 300 Patients Who Underwent Minimally Invasive Radical Cystectomy from January 2007 to July 2019
The bold value signifies that the p value for that variable is significant.
CDC = Clavien–Dindo Classification.
When categorized as CDC minor (I, II) and major (≥III) complications, 19.5% of RRC patients had a major complication compared with 18% in the LRC group (p = 0.6). Four patients (one LRC and three RRC) died within 30 days of the RC: two of them because of pulmonary embolism, while the other two as a result of urosepsis. There were 18 additional complications between days 30 and 90 and the difference between the two groups for 90-day CDC overall and major complications continued to remain insignificant. Five patients in the LRC group had a complication between 30 and 90 days: urinary tract infection (UTI) (two patients), urinary leak (one patient), pelvic abscess (one patient), and anemia requiring transfusion (one patient). For the RRC group, 13 patients had a complication between days 30 and 90: UTI (4 patients), anemia (4 patients), ureteroenteral anastomotic stricture (2 patients), neobladder fistula (1 patient), neobladder retention (1 patient), neobladder–urethral anastomotic stricture (1 patient).
With regard to rehospitalization within 30 days and surgical reintervention, there was no significant difference between the two groups. In the LRC group, 17 (15.1%) patients required a readmission within 30 days, reasons being UTI requiring intravenous antibiotics (18 patients), urinary leak (2 patients), anemia requiring blood transfusion (2 patients), ureteroenteral anastomotic stricture (1 patient), and intestinal obstruction (1 patient). Reasons for 30-day readmission in the RRC group (43 patients, 22.8%) included UTI (25 patients), urinary leak (5 patients), requirement of blood transfusion (7 patients), ureteroenteral anastomotic stricture (2 patients), neobladder retention (1 patient), subacute intestinal obstruction (1 patient), pulmonary embolism (1 patient), and dyspnoea because of pulmonary metastasis (1 patient). No difference was noted between the two groups with regard to organ-specific complications (Table 4). The surgical reinterventions are summarized in Table 5.
Thirty-Day Complications as per the Clavien–Dindo Classification and as per Organ Systems in 300 Patients Who Underwent Minimally Invasive Radical Cystectomy from January 2007 to July 2019.
Surgical Reinterventions Within 30 Days for 300 Patients Who Underwent Minimally Invasive Radical Cystectomy from January 2007 to July 2019
Predictors of complications
On univariable analysis, ASA score (odds ratio [OR]: 2.90, confidence interval [CI]: 1.17–7.19, p = 0.02), neobladder vs ileal conduit diversion (OR: 1.68, CI: 1.01–2.82, p = 0.04), and EBL (OR: 1.001, CI: 1.001–1.002, p < 0.001) were found to significantly predict the occurrence of 30-day overall CDC complications (Table 6). On multivariable analysis, ASA score (OR: 2.82, CI: 1.08–7.38, p = 0.03) and EBL (OR: 1.002, CI: 1.001–1.002, p < 0.001) retained their significance to predict overall CDC complications. None of the factors were found to be significantly associated with CDC major complications. Surgical approach (RRC vs LRC) was not found to be significantly associated with overall CDC (OR: 1.56, CI: 0.95–2.58, p = 0.07) or major CDC complications (OR: 0.97, CI: 0.53–1.77, p = 0.9) on univariable analysis.
Predictors of 30-Day Clavien–Dindo Classification Overall and Major Complications Using Univariable and Multivariable Logistic Regression
The bold values signify that the p value for that variable is significant.
CI = confidence interval; OR = odds ratio.
Trends in surgical approach and complications
We began performing RRC in 2008 and its use has increased over the years to 50% of all cystectomies in 2011 and then to 100% of cystectomies since 2015 (Fig. 1). The trends of overall, minor, and major CDC complications are shown in Figure 2. The fluctuations in all three trend lines are not statistically significant. Combining the observations of these two figures, we can conclude that although our approach to RC has shifted over the years from LRC to RRC, the incidence of overall, minor, and major CDC complications has remained fairly similar.
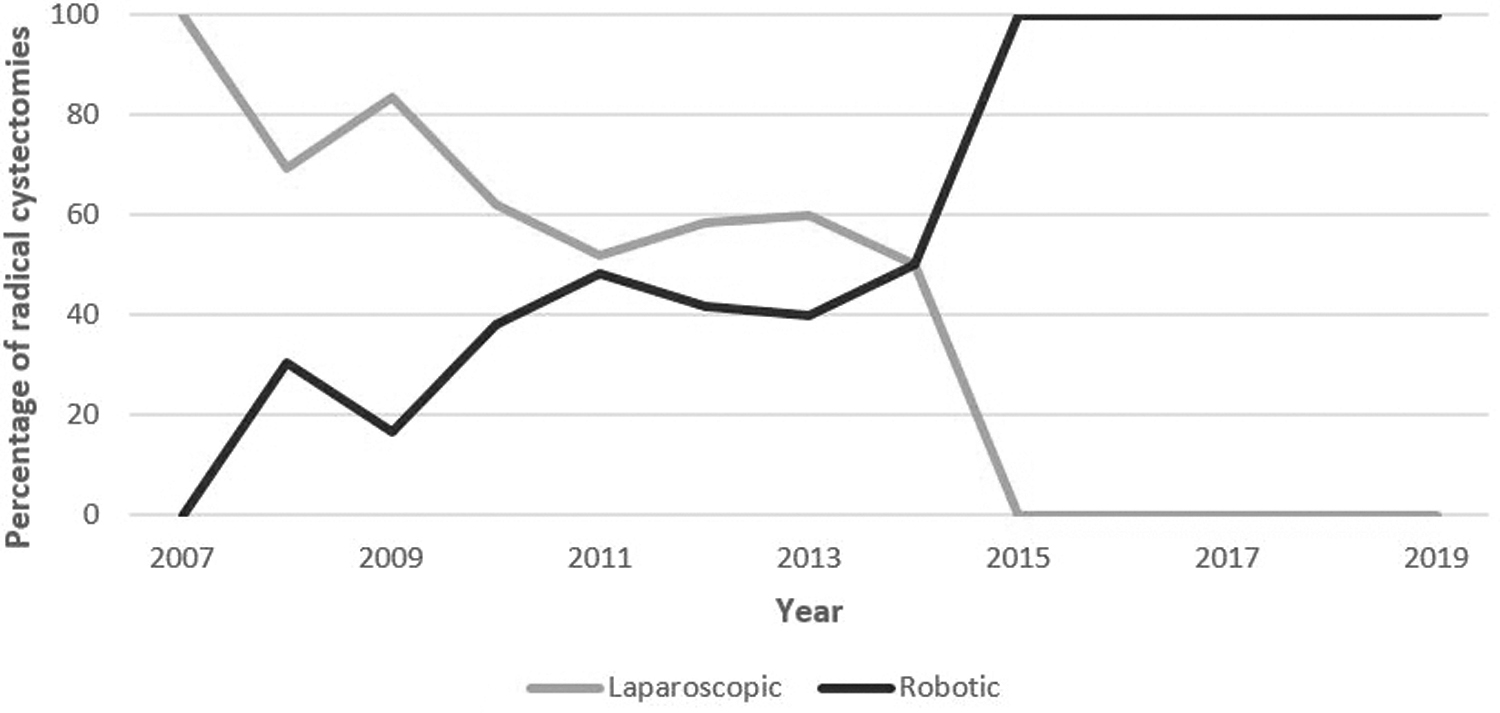
Trends of surgical approach to radical cystectomy at our institute over time.

Trends of CDC overall, minor (Grade I, II), and major (Grade ≥III) complications. CDC = Clavien–Dindo Classification.
Discussion
RC with bilateral PLND has traditionally been performed through the open approach. However, it is associated with significant perioperative morbidity. 4 –6 The technical challenge of performing an LRC meant that large series have mainly been reported from high-volume centers with experienced surgeons. 7 –10 This technical difficulty and the concurrent availability of the da Vinci® Surgical System since 2001 resulted in failure of widespread adoption of LRC. As a result of better ergonomics and a shorter learning curve compared with LRC, there have been numerous series reported for RRC worldwide. 11 –13,26
Multiple systematic reviews have been published comparing ORC with LRC or RRC. 14 –18 The general consensus is that RRC/LRC result in a similar complication profile as ORC but are associated with lesser blood loss and a shorter hospital stay. Although the established benefit of minimally invasive RC over ORC is modest, recent trials such as CORAL and BOLERO have shown poor patient accrual, with patients preferring LRC or RRC over ORC and thus preventing randomization. 21,27 The RAZOR trial was the only recent trial with large patient accrual (174 ORC vs 176 RRC), but it was performed in >15 high-volume centers in the United States. 28 We believe that minimally invasive RC would have more widespread adoption in the future and the complication rate will only get better with increased surgeon experience.
Although most of the recent single-center reports are about experience with RRC, lack of widespread availability and increased cost with the robotic system means that LRC remains an important means of offering minimally invasive RC. There is paucity of data for direct comparison of perioperative outcomes between LRC and RRC. At our high-volume center, we have been performing LRC since 2001 and RRC since 2008. To the best of our knowledge, this study represents the largest series in the Western world comparing complications between LRC and RRC.
We studied a total of 300 patients who underwent minimally invasive RC. Most of the previous retrospective reports comparing LRC or RRC with ORC were criticized for selection bias that might have inflated the difference in complications between ORC and LRC/RRC. During our study period, all patients with BCa underwent either LRC or RRC (two patients who underwent upfront ORC were excluded). This eliminated any bias regarding selection of younger and healthier patients with low disease burden for minimally invasive RC. Also, over the past few years, we have been performing all cystectomies by the robotic approach that has further eliminated selection bias (at least in the past 4 years) while comparing outcomes between LRC and RRC.
In our study, there was no significant difference between the two cohorts with regard to age, gender, and BMI. However, the patients in the RRC cohort had a higher ASA score and ACCI than the LRC group. This could probably just be a result of patients with more comorbidities presenting to us in the latter half of the study period when the number of RRC procedures exceeded LRCs. Similarly, the RRC group had a higher percentage of patients who had received NAC for urothelial MIBC. This can be explained by the fact that the use of NAC at our institute has grown substantially over time (∼85% of eligible patients presently).
Duration of surgery was comparable in the two cohorts (median of 265 minutes in LRC and 270 minutes in RRC). It is noteworthy that the operating time in RRC included the time required for docking of the robot. The median EBL in our RRC cohort was 675 mL, whereas that in the LRC group was 500 mL, with the difference being statistically significant. However, this difference does not seem to be clinically significant as it did not translate to a significantly higher rate of intraoperative blood transfusion in the RRC group. Similar findings were reported by Su et al. in their recent retrospective comparison of LRC with RRC. 22 The CORAL trial is the only prospective study comparing LRC with RRC and it had reported a significantly longer operating time and similar EBL for RRC compared with LRC, but these results have to be interpreted in light of the small sample size in that study (20 in each arm). 21 The median length of hospital stay in the RRC group was 1 day shorter than that in the LRC group (13 days vs 14 days), and although this difference was found to be statistically significant, its clinical implication is debatable.
Our results show no difference between the two groups with regard to CDC overall, minor, and major complications at both 30- and 90-day interval postsurgery. In addition, on multivariable logistic regression analysis, the approach to cystectomy (RRC vs LRC) was not found to be a significant predictor of 30-day CDC overall and major complications. The CORAL trial also did not find a significant difference but the number of complications was too small to draw a conclusion. 21 Khan and colleagues reported a higher complication rate in LRC, especially left ureteroenteral anastomotic stricture (13.7%), which they attributed to inadequate left ureteral mobilization. 20 We experienced a ureteral anastomotic stricture in ∼2% of the cases in each group. This low ureteral anastomotic stricture rate could be a reflection of the fact that we use the Wallace technique for the anastomosis.
Even while comparing for organ-specific complications, no significant differences were seen between the LRC and RRC groups. The most common complications were infectious postoperative blood transfusion and gastrointestinal complications. These findings are comparable with those reported previously in the literature. 4,13,20 Logistic regression analysis identified ASA score (III vs I, II) and EBL as independent predictors of 30-day overall CDC complications. Multiple prior reports have identified high ASA score to be a predictor of perioperative morbidity, although some of these were analyzing complications in ORC. 13,29,30 None of the factors in the logistic regression model were found to be significant predictors of 30-day major CDC complications.
At our institute, the use of robotic approach for cystectomy has steadily increased over the years and now all patients planned for a minimally invasive cystectomy undergo an RRC. In contrast, the use of LRC has gradually declined. Despite this shift in the surgical approach, there has been no significant change in the incidence of complications. This reiterates the finding of surgical approach not being an independent predictor for complications. The shift from LRC to RRC at our center could be because of increasing experience of the surgeons in using the robotic platform, a shorter learning curve with the robotic approach, and the ergonomic ease offered by the robotic system. Also, we did not find the type of robotic platform (da Vinci S-HD or da Vinci Si) to have an impact on our PLND or the neobladder–urethral anastomosis.
We acknowledge certain limitations of our study. First, data were collected retrospectively and thus the results are subject to selection bias. This has been automatically avoided in the past 4 years when we have been performing only RRC for BCa. Second, the results do not apply to patients undergoing an intracorporeal reconstruction for urinary diversion. Third, ours is a high-volume uro-oncology center with vastly experienced surgeons, and thus our outcomes are indicative of this setting and may not be applicable to centers not routinely performing minimally invasive RC. Also, being a retrospective study, there may be an element of bias in the reporting of complications. Despite the mentioned limitations, our series is one of the largest till date to compare perioperative complications between LRC and RRC. Except for higher EBL in LRC and a shorter hospital stay with RRC (the magnitudes of these differences seem clinically insignificant), our results do not demonstrate any difference in conversion to open surgery, incidence of positive surgical margins, and perioperative complications between the two cohorts. Thus, choosing between the two approaches would depend on availability of the robotic system, surgeon experience, and preference; and patients need to be counseled about comparable outcomes.
Conclusions
LRC and RRC are both feasible approaches for minimally invasive RC and PLND. LRC was associated with lesser EBL while the hospital stay was shorter in patients undergoing RRC. The two approaches were comparable to each other for 30- and 90-day CDC overall, minor, and major complications. For a surgeon, the choice between the two approaches would depend on availability and personal experience and preference, rather than any specific perioperative parameter.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was provided for this article.