
Abstract
Background:
Laparoscopic partial nephrectomy (LPN) and robot-assisted partial nephrectomy (RAPN) are commonly used techniques for treating small renal masses. Regarding renal function (RF) preservation, no superiority of one technique over the other has yet been definitely demonstrated.
Objective:
To compare functional and surgical outcomes of LPN and RAPN.
Patients and Methods:
Between 2015 and 2019, we prospectively randomized 115 patients with cT1–T2 renal masses to LPN in total ischemia or RAPN in selective ischemia. Primary endpoint was RF preservation, assessed by renal scintigraphy (RS). RS assessments were performed preoperatively and at 6 months follow-up. Secondary endpoints included clinical, histopathologic, and surgical outcomes.
Results:
One hundred eight patients were included in the final analysis. Patient and tumor characteristics were comparable. No significant difference in RS values after 6 months was observed between both groups. Median (interquartile range) RF change after 6 months was −18.0% (−26.5 to −11.0) in LPN group and −20.0 (−33.2 to −12.0) in RAPN group (p = 0.3). Mean (standard deviation [SD]) warm ischemia time was 21.1 (6.1) minutes in LPN group and 19.6 (7.7) minutes in RAPN group (p = 0.2). No positive surgical margins (PSMs) occurred in the LPN group, whereas RAPN group had PSM in 4.9% (n = 3); p = 0.099. Renal volume loss after 6 months was 27.5% (22.7–45.7) in the LPN group vs 37.5 (13.7–54.2) in the RAPN group (p = 0.5).
Mean operative times were lower in the LPN group (192.3 minutes [SD 44.5] vs 230.2 minutes [SD 59.6], p = 0.001). More complications occurred in the LPN group (31% vs 21%, p = 0.075). Transfusion rates were 15% for LPN and 11% for RAPN.
Conclusions:
In terms of preserving RF, LPN in total ischemia and RAPN in selective ischemia are comparable. In most patients, RF decrease of the affected kidney after PN seems to not exceed 25%, regardless of the surgical approach.
Introduction
Partial nephrectomy (PN) is considered the gold standard treatment modality for small renal masses. 1 Besides complete tumor extirpation with minimal complications, the primary goal for an ideal PN is the maximum preservation of renal function (RF), as defined by the “trifecta concept.” 2 Extensive evidence suggests that an impaired postoperative RF increases the risk of cardiovascular disease, use of specialized health care, and death. 3 Laparoscopic partial nephrectomy (LPN) compared with open partial nephrectomy (OPN) is associated with improved perioperative and postoperative morbidity and comparable long-term oncologic results for T1 lesions. 4 Nevertheless, LPN has never completely replaced open surgery, most likely because of its higher technical demands, especially for the management of challenging masses in unpleasant locations. 5 In these cases, LPN usually requires a longer warm ischemia time (WIT), which can possibly impair RF. 6 Robot-assisted partial nephrectomy (RAPN) facilitates challenging steps of PN such as vascular preparation, tumor excision, and renorrhaphy, also taking advantage of the near-infrared fluorescence imaging (NIRF) system to evaluate the extent of the ischemic areas. This allows a “tailored” selective ischemia limited to the tumor, whereas sparing healthy renal parenchyma. 7 Recent literature suggests that RAPN is more favorable compared with LPN not only in terms of WIT, but also in regard to perioperative and postoperative complications, conversion rates to radical nephrectomy, duration of hospitalization, overall mortality rate, and RF preservation. 8 Our study aims to provide Level 1 evidence data regarding functional and surgical outcomes of RAPN and LPN.
Patients and Methods
Regulatory issues
This study was approved by the local ethics committee (EKNZ 2015-446) and was registered on
Study population
Recruitment of study participants was performed according to a trial flowchart (Fig. 1). Male and female patients >18 years with cT1–cT2 renal tumors eligible for selective clamping (assessed by CT-scans) were eligible. Patients with Charlson Comorbidity Index (CCI) >10, chronic kidney disease (CKD) stages 4–5, previous renal surgeries or concomitant oncologic diseases, immune diseases, cT3+ or cN1 renal cancer were not admitted. Patients were discussed in a multidisciplinary consensus board to evaluate the feasibility and indication of a PN. Randomization was performed regardless of possible surgical difficulties that might have been brought up by tumor size, location, or complexity.

Trial flowchart comparing enrollments of patients treated by conventional LPN vs RAPN in a single institution from 2015 to 2018. LPN, laparoscopic partial nephrectomy; RAPN, robot-assisted partial nephrectomy.
The study design was a single-center prospective randomized trial comparing functional and surgical outcomes between LPN in total ischemia (“LPN group”) and RAPN in selective ischemia (“RAPN group”), conducted at Luzerner Kantonsspital, Switzerland. All surgeries were performed between 2015 and 2019 by a single surgeon with expertise in both LPN and RAPN (n = 70 for LPN and n = 100 for RAPN before enrolment of the first study patient).
Surgical techniques and study assessments
In the LPN group, a laparoscopic Satinsky clamp was used to induce total kidney ischemia, clamping both vein and artery before tumor resection. In the RAPN group, bulldog clamps were used to clamp segmental tumor-feeding arterial branches. Indocyanine green was infused intravenously a few seconds after selective ischemia was induced. Da-Vinci Firefly™ NIRF was used to tailor the extent of the ischemic area by adding or removing bulldog clamps before tumor resection was performed. In both LPN and RAPN, the surgeon aimed to perform an enucleoresection of the tumor. 9 Visible open vessels were closed directly using 5 mm Titanium-clips or Hem-o-Lok® during resection. After resection, the defect was closed by placing TaboTamp® in the deeper layers of the defect and performing a single-layer noncontinuous outer renorrhaphy.
Perioperative and intraoperative study assessments are demonstrated in Figure 2. The primary study endpoint was defined as RF change 6 months after surgery using split RF assessed by mercaptoacetyltriglycine (MAG3) renal scintigraphy (RS) as surrogate. Differences in duration of operation, WIT, hemoglobin drop, transfusion rates, length of stay, positive surgical margins (PSMs), intra- and postoperative complications (Clavien–Dindo classification), and kidney volume changes (Syngo.Via® volumetry) were defined as secondary endpoints. Depending on final histopathology, patients received a follow-up, including CT, MRI, or ultrasound (US) 6 months postoperatively. Complications were assessed from the day of surgery until the latest follow-up after 6 months. Evaluation of pre- and postoperative RS values, CT, MRI, and US data was performed by dedicated uro-radiologists and specialists in nuclear medicine. Histopathologic work-up of the specimen and reporting was performed according to standardized measures by the International Society of Urological Pathology (ISUP). In cases of staging uncertainty, adjunctive immunohistochemistry was performed to confirm the presence or absence of PSM.
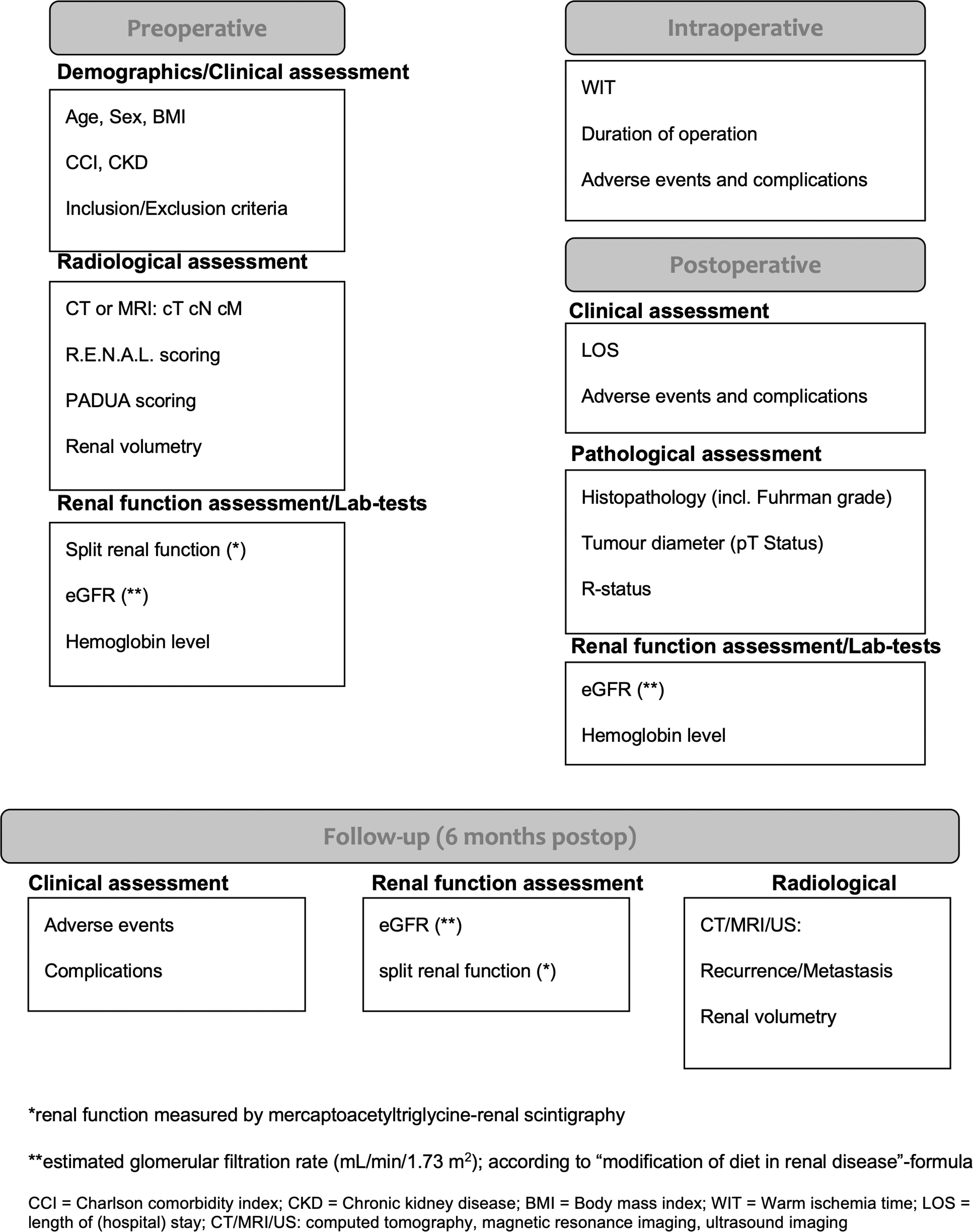
Preoperative, intraoperative, and postoperative assessments comparing oncologic and functional outcomes of LPN in total ischemia (LPN) vs RAPN in selective ischemia (RAPN) in a prospective randomized single surgeon trial between 2015 and 2018.
Power analysis and statistical considerations
Patients were 1:1 randomized in two groups (“LPN group” and “RAPN group”) by a computer-based prospective random sequence generator. Based on estimates from previous studies systematically evaluating RF decrease after PN, the expected changes of the affected kidney are ∼10% and 5% after PN with total ischemia and selective ischemia, respectively. 10 –15 A sample size was calculated for each group, with a type I error of 0.05 and a power of 80%. According to these considerations, we aimed to recruit 53 patients per group to be able to detect a potentially statistically significant difference in RF preservation between groups. However, expecting a 10% dropout or being lost to follow-up, further patients were enrolled during the recruitment period.
Categorical variables are reported as frequency and percentage, and continuous variables as mean and standard deviation (SD). The Mann–Whitney and chi-square tests (or the Fisher exact test) were used to compare continuous and categorical variables among groups.
Statistical analysis was elaborated using SPSS v.20.0 (IBM Corp., Armonk, NY, USA). All reported p-values are two-sided and statistical significance was set at p < 0.05.
Results
One hundred twenty-nine patients were identified for this study between 2015 and 2019. One hundred fifteen patients meeting inclusion criteria proceeded to randomization. Fifty-four patients were randomized to LPN and 61 to RAPN. Demographic and clinical tumor characteristics included in the final analysis were comparable (Table 1). No patient was lost to follow-up in the LPN group, whereas five patients were lost in the RAPN group.
Demographic Characteristics of Patients Randomized to LPN Group (Laparoscopic Partial Nephrectomy in Total Ischemia) and RAPN Group (Robot-Assisted Laparoscopic Partial Nephrectomy in Selective Ischemia) Between 2015 and 2019
All p > 0.05.
BMI, body mass index; CCI, Charlson Comorbidity Index, n (%); CKD, chronic kidney disease; IQR, interquartile range; SD, standard deviation.
Influence of PN on kidney function
Preoperative RS values showed an equal distribution of RF in both groups, both in healthy and tumor-bearing kidneys. At 6 months follow-up, no statistically significant difference in RF changes between the groups was found, neither in healthy nor tumor-bearing kidneys. The median increase of RF in the healthy kidney and decrease of RF in the operated kidney was comparable between both groups (Table 2). We further stratified the percentage of RS-value decrease at 6 months follow-up to three subgroups of ≤25%, 26%–50%, and ≥51%–100%. The majority of patients (40 patients in LPN group and 43 patients in RAPN group) had a deterioration of ≤25%. An RF deterioration of 26%–50% was seen in 10 patients in LPN group and 15 patients in RAPN. An RF deterioration of ≥51% was seen in four patients in LPN group and three patients in RAPN group (Table 2). When analyzing relative change of estimated glomerular filtration rate (eGFR) between preoperative values and fourth postoperative day as well as at 6 months follow-up, no significant difference was detected between groups (Table 3). Three patients (5%) from LPN group and four patients (6%) from RAPN group developed a de novo CKD stage ≥3 at 6 months follow-up.
Perioperative Functional Outcomes of Patients Randomized to LPN Group (Laparoscopic Partial Nephrectomy in Total Ischemia) and RAPN Group (Robot-Assisted Laparoscopic Partial Nephrectomy in Selective Ischemia) Between 2015 and 2019 According to Results of Preoperative and 6 Months Postoperative (Mercaptoacetyltriglycine) Renal Scintigraphy Values
RF modification was assessed by percentage change in renal scintigraphy from before surgery to follow-up time.
RF = renal function.
Perioperative Functional Outcomes of Patients Randomized to LPN Group (Laparoscopic Partial Nephrectomy in Total Ischemia) and RAPN group (Robot-Assisted Laparoscopic Partial Nephrectomy in Selective Ischemia) Between 2015 and 2019 According to Results of Preoperative Estimated Glomerular Filtration Rate compared with Fourth Postoperative Day and 6 Months After Surgery
eGFR (mL/minute/1.73 m2), according to “modification of diet in renal disease (MDRD)” formula.
eGFR = estimated glomerular filtration rate.
Surgical and histopathologic outcomes
Duration of operation was significantly longer for RAPN (mean +37.9 minutes, p = 0.001). Mean WIT and tumor complexity (assessed by PADUA and R.E.N.A.L. scoring) between both groups was comparable (Table 4). For surgical safety reasons, the LPN approach was changed intraoperatively to a total nephrectomy in two cases (3.70%).
Operative Characteristics, Pathologic Data, and Complications of Patients Randomized to LPN Group (Pure Laparoscopic Partial Nephrectomy in Total Ischemia) and RAPN Group (Robot-Assisted Laparoscopic Partial Nephrectomy in Selective Ischemia) Between 2015 and 2019
LOS = length of stay; PSM = positive surgical margin; RCC = renal cell carcinoma; WIT = warm ischemia time.
Histopathologic results predominantly showed RCC T1a–b (74% in LPN and 66% in RAPN group) with a Fuhrman grade ≤2 (87% in LPN and 85% in RAPN). Benign histology, such as angiomyolipoma or oncocytoma, was found in 20% in the LPN group and 25% in the RAPN group. No PSM was found in the LPN group, whereas RAPN had three PSM (5%).
Mean negative kidney volume change of the affected kidney 6 months after surgery was comparable between both groups.
Complication rate was 31% in LPN group and 21% in RAPN group (p = 0.075). Predominant complications in LPN group were grade II (68%), whereas grade IIIa complications were predominant in RAPN group (43%). The main cause of postoperative complications was persistent bleeding from the surgical site (38.89% of all complications for LPN and 50% of all complications for RAPN). Transfusion rates were 15% for LPN and 11% for RAPN. Coiling of pseudoaneurysms was performed in five patients in RAPN group, whereas no coiling was performed in the LPN group. Success rate of coiling was 100%. Overall bleeding complications (regardless of Clavien–Dindo grading) occurred in 25.9% in the LPN group and 18.0% in the RAPN group. One grade IVa complication occurred each in LPN group (septic shock caused by severe infection of renal hematoma with open surgical revision) and RAPN group (cardiogenic shock caused by acute myocardial infarction). No grade V complication occurred in both groups.
Discussion
Recent meta-analyses of retrospective studies favor RAPN over LPN, especially in terms of shorter WIT. 8,16 LPN is being attributed as technically more challenging and with a steeper learning curve compared with RAPN, suggesting worse functional outcomes. 17,18 Furthermore, with the implementation of the NIRF system and the rise of live three-dimensional view, superimposing images of the renal hilus and tumor-feeding vessels directly in the console, selective artery clamping during PN appears to be an interesting option especially for RAPN, whereas technical and surgical demands in LPN seem to be rather impeding for selective clamping. 19 Despite lacking prospective data on this topic, some authors propose that there seems to be no actual competition between RAPN and LPN; indeed, the real competition is being proposed rather in comparing OPN with RAPN. 20 Contrary to this, recent results from a multicenter observational study suggest that any minimally invasive approach is more favorable in avoiding acute kidney injury after surgery compared with OPN. 21
To our knowledge, we performed the first prospective randomized controlled trial comparing functional outcomes of RAPN in selective ischemia vs LPN in total ischemia with split RS values as surrogate for RF deterioration of the affected kidney.
Literature suggests that the most effective and accurate way to determine renal damage after PN in the setting of bilateral kidneys is the assessment of eGFR in combination with pre- and postoperative RS, which allow to objectively quantify RF changes in the affected kidney. 10,14,22 It has been demonstrated earlier, that the maximum damage of renal tissue after PN is overcome 3 months postoperatively and no further worsening occurs after 2 years follow-up. 13 Therefore, using the combination of eGFR and RS values preoperatively and 6 months postoperatively, our study yielded relevant and, so far, unique data on the impact of LPN and RAPN in terms of RF change. In this regard, our trial could not detect a statistically significant difference between LPN and RAPN, which is the main conclusion from our study.
When analyzing other modifiable determinants of functional outcome after PN, evidence suggests that RF depends on various factors, including type and duration of ischemia, excisional volume loss, and reconstruction-related injury. 23,24 Especially, the role of healthy parenchymal tissue preservation during tumor excision has been proposed as a major predictor of ultimate RF. 23,25 Therefore, tumor size and degree of complexity directly affects functional results by influencing the amount of renal parenchyma resected. As our data inherit comparable tumor sizes and complexities, and standardized approaches (enucleoresection of the tumor and identical renorrhaphy techniques in each case, mean WIT <25 minutes) performed by a single surgeon, we think that our results are robust. Furthermore, using specialized software, we calculated kidney volume changes 6 months postoperatively and could not find a significant difference between both groups, which is consistent with the previously described homogeneity of RF changes in both groups. Still, compared with existing literature, the kidney volume loss in our cohort, regardless of the LPN or RPN approach, was relatively high. 26 In this regard, as we aimed to perform an enucleoresection for all tumors in both approaches, we conclude that especially the renorrhaphy technique (using a noncontinuous cortical renorrhaphy) might have contributed to the renal volume loss.
However, maximum RF preservation while treating renal masses should not be the only key factor for the surgeon. While striving for the well-established “Trifecta”-concept (no PSM, WIT <25 minutes, no complications ≥Clavien–Dindo II), we should keep in mind that the risk to overestimate the surgeon's skills and capacities in the desire to offer PN even for highly complex tumors to maximize postoperative RF could as well lead to unfavorable oncologic outcomes, because of higher PSM or complication rates. 27 PSM predicts worse survival, higher local recurrence rates, and metastasis. 28 Furthermore, the risk of PSM has risen since the introduction of minimally invasive PN (6.8%–7.3% from 2010 to 2013 in the United States) and is more likely in kidneys with higher pathologic T stages and higher nephrometry scores. 28,29 Therefore, to offer the best condition for a clean tumor resection, the anticipated excision area should be ischemic and consequently free of bleeding, which could potentially ameliorate the view on the resection margin. However, in our study, we found that quite often several undetected small branches during selective ischemia still perfused the resection border to a certain degree, which complicated resection dexterity and might be a reason for slightly higher PSM rate in the RAPN group. Another explanation for the PSM in the robot-assisted approach might be the potentially increased risk to induce iatrogenic lesions in the tumor during resection because of the smaller and, therefore, eventually more traumatic robotic instruments.
Apart from this, we think that selective ischemia, demanding a more precise preparation of the renal hilus, was the main reason for the significantly longer surgery times in the RAPN group. Still, both LPN in total ischemia and RAPN in selective ischemia were found to be feasible techniques with a similar spectrum of complications; although LPN by trend had a higher rate of complications in general (31% vs 21%), RAPN was found to inherit more severe grades (IIIa and higher) and was the only approach provoking postoperative pseudoaneurysms needing angiographic coiling. Latter is opposed to recent findings in the literature, which stated a higher probability for coiling after LPN. 30
Although our study was planned and performed meticulously, we acknowledge limitations in our study design and results. The aim of this study was to represent our personal clinical practice regarding clamping techniques for RAPN and LPN. We are aware that also a total ischemia approach during RAPN is commonly utilized in many centers. Needless to say, selective clamping is also feasible during LPN, but we assume that many surgeons would prefer a total ischemia in most of the cases because of the higher technical complexity of hilus preparation and lack of NIRF in most centers using the conventional laparoscopic technique. Therefore, we decided to compare not only two surgical techniques (LPN and RAPN) but also two different ischemia approaches (selective and total ischemia), which can be regarded a limitation of this study. Having said that, we are of the opinion that based on our results the ischemia technique might not be the main driving factor for preserving RF, as long as the trifecta concept (and especially a WIT ≤25 minutes) is being respected.
Furthermore, secondary outcomes, especially when looking on PSM and complication rates, are trend results only because of the study being powered on differences in RS values, and do not suffice to claim RAPN superior to LPN or vice versa.
Conclusion
In terms of preserving RF, LPN in total ischemia and RAPN in selective ischemia are comparable. In most patients, RF decrease of the affected kidney after PN seems to not exceed 25%, regardless of the surgical approach.
Take Home Message
This trial did not yield a significant difference between laparoscopic partial nephrectomy in total ischemia and robot-assisted partial nephrectomy in selective ischemia in terms of preserving renal function 6 months after surgery. In most patients, RF decrease of the affected kidney after PN seems to not exceed 25%, regardless of the surgical approach.
Footnotes
Acknowledgments
The authors thank the Clinical Trials Unit Nottwil (Switzerland) for the scientific input and providing the framework for the database and the Max und Hedwig Niedermaier Foundation (Switzerland) for providing a junior grant for this protocol.
Funding Information
Christoph Würnschimmel received a junior grant for the study protocol from Max- und Hedwig Niedermaier Foundation, Zurich, Switzerland.