
Abstract
Background:
A single-use flexible cystoscope with integrated grasper (Isiris; Coloplast, Denmark) has recently become commercially available. The objective of our study is to compare the costs of stent removal in an outpatient clinical environment between the single-use Isiris system (Coloplast) to our existing approach using a reusable cystoscope and stent grasper.
Materials and Methods:
The number of stent removal procedures at our tertiary center was recorded as a proportion of all cystoscopic procedures performed between February 2016 and February 2017. Elements in the micro-cost assessment included original purchasing price of an Olympus digital reusable cystoscope, repair fee (based on a 1-year contract), sterilization equipment and accessory costs, reprocessing costs of the cystoscope, and labor costs. The costs were estimated on a per-use basis and compared to the purchasing price of Isiris.
Results:
A total of 1775 cystoscopic procedures were performed, and the reusable cystoscope was used for stent removal in 871 (49%) cases. The per-use cost for stent removal procedures using the reusable cystoscope was estimated to be $161.85. The single per-use purchasing price for the Isiris device is $200. Based on the current volume, the break-even point was calculated to be 704 stent pulls. After 704 stent pulls, the cost benefit favors the reusable cystoscope.
Conclusion:
Based on this micro-cost analysis, per-use costs appear to favor the reusable cystoscope for stent removal. It appears that centers with high volumes of stent pulls may find the reusable cystoscope and stent grasper more cost beneficial than the single-use system.
Introduction
The placement and removal of ureteral stents are one of the most common procedures performed by urologists worldwide. Ureteral stents are composed of various materials (soft plastics, metallic stents, etc.) and are placed not only for variable indications, including, most commonly, urolithiasis, but also for hydronephrosis from various intrinsic and extrinsic causes, ureteral trauma, and identification of the ureters during complex intra-abdominal surgeries. 1 Stents can be left in place for various lengths of time depending on the indication, but they should be removed or exchanged routinely to avoid encrustation.
Although this office-based procedure takes only minutes to perform, the setup of an office visit for a ureteral stent removal can be burdensome and labor intensive. It often requires staff members with knowledge of the sterilization process, time to setup the room, occasionally an assistant to grab the stent, and periodic maintenance of the equipment.
Coloplast has developed the Isiris, a single-use cystoscope with built-in stent grasper. This pioneering device is advertised to have state-of-the-art digital technology, allow for a single operator, and prevent cross contamination by eliminating the need for processing and sterilization.
With a rising trend in disposable scope usage in urologic surgeries, it is important to consider the cost ramifications to the health care system. Phan & colleagues and Baston & colleagues are only two groups who have evaluated the cost differences between a single-use scope and the traditional technique to remove indwelling ureteral stents. 2,3 The objective of the current study is to compare the cost of the single-use Isiris to the costs of the traditional technique of using a reusable cystoscope to remove indwelling ureteral stents.
Materials and Methods
This is a retrospective study. The per-use cost of removing an indwelling ureteral stent using the traditional, reusable cystoscope and stent grasper setup was estimated and compared to the per-use cost of Isiris. At our tertiary care center, the stent pull procedure is performed in an outpatient office-based procedure room setting, with one nurse assisting the surgeon. Since the cystoscope is also used for other indications (e.g., diagnostic cystourethroscopy, etc.), the proportion of stent pulls was first estimated as a function of all cystoscopic procedures to isolate the cost of stent pulls alone.
The elements included in the micro-costing analysis consisted of the following: (1) purchasing cost of an Olympus flexible digital cystoscope (CYF-VH). The Olympus digital flexible cystoscope is typically replaced in our department every 5 years, and this was factored into the calculation to first obtain a per annum cost before obtaining a per-use cost; (2) the servicing contract for repairs (per scope, per annum); (3) the reprocessing costs, including all materials to properly decontaminate and repackage the scope and associated equipment; (4) labor costs based on the time and salary of personnel performing the reprocessing at that time; and (5) the cost for the sterilization equipment and the accompanying accessories, as well as the service contract for the sterilizing equipment (Sterrad). The cost breakdown of each of the criteria in the micro-cost analysis is described in Table 1.
Elements Included in the Micro-Costing Analysis, Calculated on a Per-Use Basis
Costs were tabulated from our administrative resources within our Urology department for the February 2016–February 2017 fiscal year, and also from the companies supplying the equipment (Coloplast). The Isiris scope includes an accompanying monitor in the purchasing price of the scope, which may vary from one institution to another.
From February 2016 to February 2017 fiscal year, a total of 1775 flexible cystoscopies were performed in the Urology department, specifically at one outpatient clinic location to uniformly address the cost analysis. Of the total number of flexible cystoscopies performed, 871 were to remove an indwelling ureteral stent. The procedure is performed awake, with no sedation, using intraurethral lidocaine gel in men and women. Based on our micro-cost analysis, each cystoscopic use for ureteral stent removal costs $161.85 USD compared to the purchasing price of the Isiris at $200 USD (Table 1).
An analysis was performed to determine the break-even point for the use of Isiris for the department (Fig. 1). The break-even point was calculated to be 705 ureteral stent pulls. For high-volume tertiary centers performing more than the break-even point, it would be justified to purchase reusable equipment as the per-use costs would be <$200. For centers performing <705 stent pull procedures per year, it may be less costly to use the single-use Isiris scope for stent pulls.
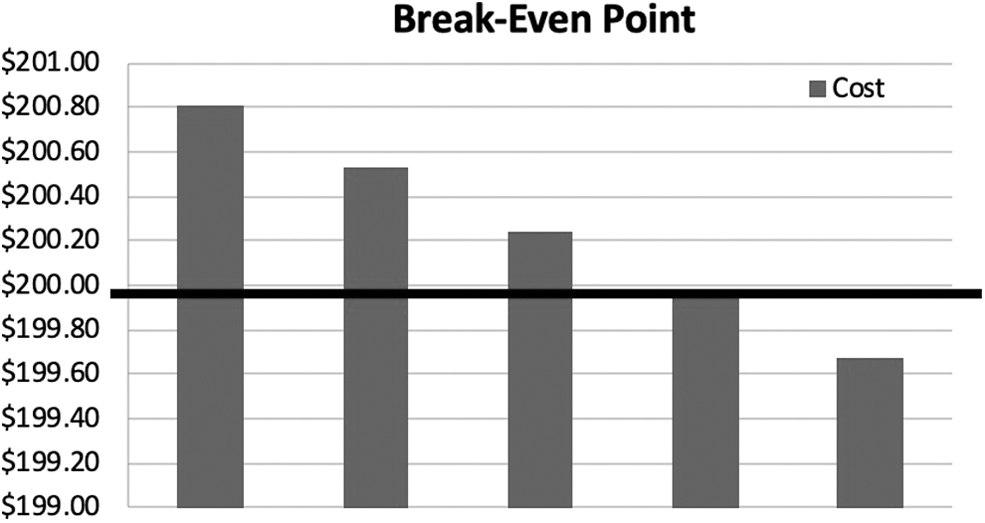
Break-even point calculated at 705 stent pulls per annum (indicated by black line).
Discussion
Despite being one of the most common procedures performed, traditional stent removal requires multiple considerations. For example, knowledgeable staff members are needed to setup the procedure in a sterile manner, ensure timely turnovers of scopes to prevent delays, and reprocessing the equipment in a meticulous step-by-step protocol to prevent transmission of infections (Fig. 2). An extensive reprocessing protocol is important to reduce the risk of infection, and has even been demonstrated to minimize the risk of mechanical failure. 4 However, even an appropriate sterilization technique can fail to eradicate all bacteria on the scope. 5 Isaacson and colleagues highlight the costs of reprocessing scopes, costing an average of $96.13, but more importantly, the time it takes for each individual step can also lead to expensive delays. 6
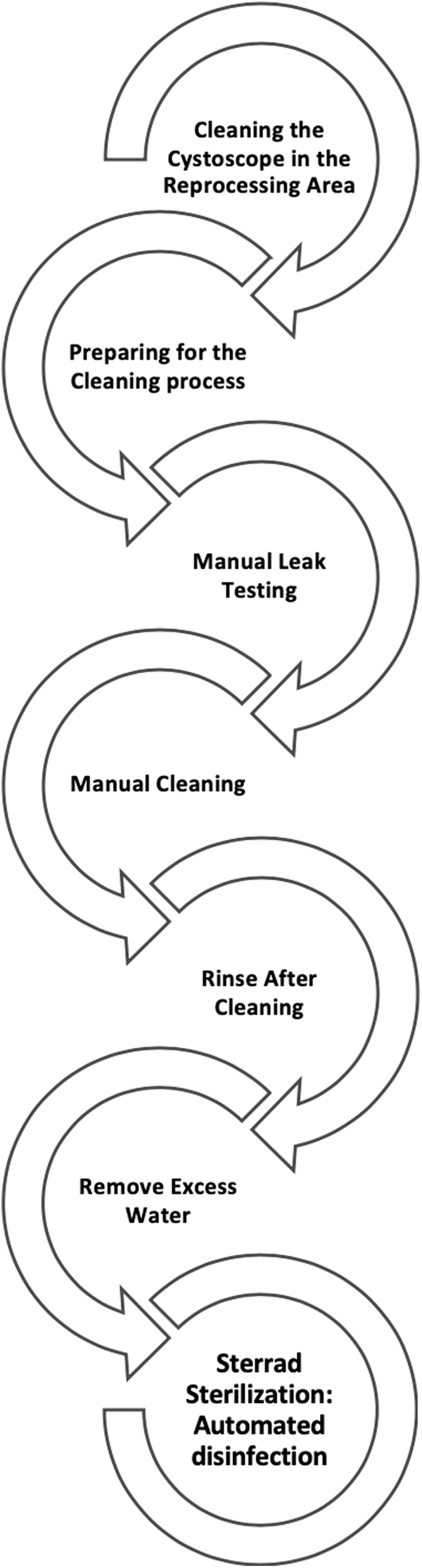
Step-by-step reprocessing protocol (institution specific).
Despite having knowledgeable staff who are all Occupational Safety and Health Administration (OSHA) trained for the sterilization of cystoscopes, mechanical failures and scope breakage are anticipated with the need for repairs. There is an added chance of scope breakage or malfunctioning in the reprocessing, which leads to added costs. McGill and colleagues demonstrated that reprocessing protocols can decrease cost when comparing two protocols, illustrating that it costs about $9.64 per procedure failure vs $5.41 using their new protocol. 4 Their study also poignantly shows cost per procedure failure representing the added costs. In 1997, Fuselier and Mason reported the number of flexible cystoscope repairs at a large academic center, demonstrating that the average repair cost was >$1500 in a 2-year duration and seven cystoscopes needing replacement or repairs emphasizing that these costs are not a small amount. 7 As such, the overall reprocessing protocol and normal wear-and-tear can lead to added costs in itself for repairs or replacements.
In an effort to mitigate these nuisances, there has been a trend in the increased use of single-use, disposable instruments, including cystoscopes and ureteroscopes (LithoVue, Pusen, WiScope, etc.). Disposable equipment can provide benefits such as bypassing all sterilization protocols, decreasing the risk of bacterial contamination, no mechanical failure, new scope at every use and no need for repair costs, no need for extra personnel for grasper use, and easy features for use. One additional advantage is that disposable cystoscopes would be readily available if ordered and stored in a timely and orderly manner based on clinic volume, due to bypassing the entire reprocessing pathway. On the contrary, they can be costly, and one needs to take this into consideration with the rising costs of health care.
Isiris is a new, single-use disposable flexible cystoscope with an integrated stent grasper that is activated by a ratchet (Fig. 3). Its clinical feasibility has been previously reported. Talso and colleagues evaluated the quality of the device in comparison to five different reusable flexible cystoscopes and demonstrated through four standardized scenarios that the image quality and water flow is comparable. 8 Doizi and colleagues demonstrated in a prospective cohort multi-institutional study in Europe of a clinical evaluation of the Isiris by evaluating image quality, active deflection, maneuverability, and grasper functionality in an in-vivo patient setting. 9 They showed that the Isiris was unable to retrieve the stent in five patients, where four patients had encrusted stents and one patient had a migrated stent up the ureter where stent removal was attempted with the reusable conventional cystoscope and grasper but was unable to obtain the stent and required subsequent ureteroscopy. 9 Based on their criteria, Isiris works effectively in removal of indwelling ureteral stents with minimal complications. Conversely, these studies did not evaluate the costs associated with the use of the Isiris in comparison to the conventional cystoscope and grasper.

Isiris cystoscope and grasper (© Coloplast, with permission).
One important question is how this new disposable equipment impacts health care costs. One consideration would be to avoid placing stents in the first place, or leaving strings attached to avoid the procedure to remove the stent. Both scenarios have been studied but have not gained wide traction for a variety of reasons. Factors including case complexity, ED visits, and inadvertent dislodgment of stents need to be considered, however, these options can still lower the overall costs related to stents. Another important cost consideration is repair cost associated with reusable equipment. Canales and colleagues performed an independent analysis on the cost of repairs of Olympus flexible reusable cystoscopes and determined that the most common site of damage on the scope that required repair is at the distal deflection tip (28% of the 1150 repairs on Olympus cystoscopes), which at that time ranged from $85 to $1370 depending on the repair needed. 10 There is some potential cost savings in disposable equipment by foregoing the reusable equipment's associated repair fees (contract fees, repair fees, including labor and parts, etc.).
LithoVue, the single-use disposable ureteroscope by Boston Scientific has been released in the market before the development of the Isiris. Martin and colleagues compared costs of a reusable flexible ureteroscope (Storz Flex XC ureteroscope) to the LithoVue and determined that after 99 ureteroscopic uses, cost-benefit analysis favored reusable scopes. In addition, there was a determined 12.5 average ureteroscopic cases to reusable device failure. The authors concluded that at low-volume centers, a disposable ureteroscope may be cost beneficial. 11 Taguchi & colleagues and Hennessey & colleagues also illustrate similar findings in micro-cost analyses, demonstrating that although LithoVue acquisition costs may be higher, there are savings realized in labor, consumables, and repairs. 12,13 A PRISMA systematic review by Talso and colleagues compared disposable and reusable flexible ureteroscopes from 2000 to 2018 further drives the observation of decreasing costs with increased volume of procedures, displaying that reusable flexible ureteroscopes are still more cost-effective than disposable scopes. 14
Traditionally, ureteral stents are removed through the visualization of a sterile cystoscope with a reusable stent grasper or via an extraction string. Baston and colleagues show that extraction of the stent via string can be a good option for patients, with no increased admission rates after stent removal by string and lower indwelling time of stent. 3 Others have demonstrated that the use of extraction string poses a risk of accidental stent dislodgement (7%–15%) that can lead to accidental costs. 15 –17 Due to this risk, some urologists prefer to have stents removed with a cystoscope, as the use of extraction string is not feasible in all patients.
Phan and colleagues demonstrated in their cost analysis in the United Kingdom that using the Isiris was a more expensive option compared to the reusable cystoscope (£260.65 for Isiris vs £123.41 for the reusable system). However, Isiris provided ease and flexibility to providers, with an astounding 60% of stent removals being delayed in patients for the reusable system and 0% of the time with Isiris. 2 Similarly, with endoscopy suite constraints in the United Kingdom, Baston and colleagues demonstrated in a retrospective review that patients with Isiris cystoscope stent removal had a 33.5% reduction in ED attendance and 22% reduction in hospital readmission rates compared to the standard reusable cystoscope group due to having their stents removed in a shorter period of time (able to be done in clinic instead of the endoscopy suites). 3 This translated to ∼£750 cost saving per 100 stent removals. Overall, our results are consistent with other published series demonstrating that there are some economic benefits of a disposable scope system in the office setting.
As medical technologies advance toward increasing the safety profile of devices, it is essential that we also consider the impact of our carbon footprint on the environment. The majority of medical equipment is not recyclable and also needs proper handling to be disposed. The disposal of disposable equipment is a factor that has not been explored extensively. 18 Davis and colleagues had demonstrated that the carbon footprint of a disposable and reusable flexible ureteroscope have comparable environmental impacts, but is still concerning as a source of emission. 19 There may be additional unidentified direct or indirect costs of disposing such equipment. It would be important for manufacturers to consider recycling whole or portions of these devices to reduce our impact on the environment.
The current cost analysis is based on a 1-year evaluation of our current volume at a single institution. In calculating the cost savings, it is $38.15 saved per stent pull ($200–$161.85 = $38.15) when performing 871 stent pulls (per year) and equates to savings of $33,228.65/year at our institution, which is a substantial amount. If the number of stent pulls is less than 704, the cost benefit may favor the disposable scope over the reusable scope. However, this cost-benefit analysis is a reflection of our current volume—either within our institution or across institutions. The cost per procedure is variable to the volume of procedures, thus the purchasing price of the cystoscopes, hours paid to the staff for cleaning and storing our equipment, and bulk ordering can alter based on changes of volume at other institutions.
There are limitations to this study. First, the cost of reprocessing and sterilization calculated per scope use cannot be generalized. It is based on contracts made between organizations and product ordering for our institution. In addition, there are some added costs that have not been factored into our analysis such as the cost of the tower and specific repair costs. We are working off the assumption that most urology offices have a tower/video system already, since other procedures such as diagnostic cystoscopy, Botox injections, and other procedures would likely be routinely performed. We also took into consideration that even if a center switched over to this single use ISIRIS system for all stent removals, they would still likely need to maintain their standard cystoscopy towers and scopes for these other procedures. Therefore, we did not include this as a separate line item in our cost analysis. Furthermore, the use of consumables can vary by contract from institution to institution, especially with bulk purchasing. As such, the same micro-cost analysis may not be reproducible from a year to year basis or between institutions. We utilized digital cystoscopes for stent removal in this study. In our clinics, we are standardized to digital cystoscopes as they are also used for diagnostic cystoscopies. Fiber optic cystoscopes, which are generally less costly to purchase, could also be utilized for stent removal and could alter the cost analysis. Our study specifically addresses the cost-benefit analysis of the use of a disposable cystoscope for stent removal at a large volume center and may not apply to centers with lower case volumes. Furthermore, practice patterns across the globe varies, with other centers performing stent pulls in the operating room, dedicated endoscopy suites, or clinical settings, all of which will be associated with variable costs.
Conclusion
Disposable equipment is becoming widely available, particularly in the realm of endourology, and can potentially improve the provision of care in certain settings, while also reducing associated costs. Based on this micro-cost analysis, the Isiris disposable stent grasper was more costly than the reusable system. However, it appears that at centers with lower volumes of stent pulls, Isiris may be more cost-beneficial.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.