
Abstract
Objectives:
To analyze predictors of open conversion during minimally invasive partial nephrectomy (MIPN) for cT1 renal masses.
Methods:
The National Cancer Database (NCDB) was investigated for kidney cancer patients who underwent partial nephrectomy (PN) between 2010 and 2015. Patients who underwent MIPN were stratified into converted and nonconverted groups. Sociodemographics, facility characteristics, and surgical outcomes were compared between the two groups, and multivariate logistic regression model was fitted to identify independent predictors of open conversion.
Results:
In total, 54,246 patients underwent PN for kidney cancer during the 6-year period. Of those, 18,994 (35%) were open partial nephrectomies (OPNs) and 35,252 (64%) were MIPN. Overall, 1010 (2.87%) of MIPNs were converted to OPN. There was an increasing utilization of MIPN from 50.35% in 2010 to 74.73% in 2015. Patients who had open conversion had more 30-day readmissions (5.95% vs 3.31%, p < 0.01). On multivariate analysis; high-volume facility (>30 MIPNs/year), year of surgery (2015 vs 2010), and robotic approach predicted a lower likelihood of conversion (odds ratio [OR] 0.52, confidence interval [CI] 0.44–0.62; OR 0.59, CI 0.47–0.73; and OR 0.31, CI 0.27–0.35; respectively, p < 0.001 for all). Conversely, Medicaid (vs private insurance; OR 1.75, CI 1.39–2.19, p < 0.001) and male sex (OR 1.26, CI 1.11–1.44, p < 0.001) were independent predictors of conversion.
Conclusions:
Open conversion in MIPN occurred in 2.87% of cases. There was an increasing utilization of MIPN associated with decreased conversion rates. Higher volume hospitals and progressing year of surgery were associated with less likelihood of conversion.
Introduction
The incidence of early stage kidney cancer has increased from 3.4% to 7% per 100,000 adults over the past decade. 1 Surgical management, namely partial nephrectomy (PN), remains a standard option for management. 2 Minimally invasive partial nephrectomy (MIPN) has evolved to be an established alternative approach to open partial nephrectomy (OPN) with well-proven perioperative benefits. 3 MIPN has been associated with less blood loss, shorter hospital stays, lower readmission rates, and decreased operative time when compared to OPN. 4,5 Introduction of robot assistance has resulted in significant shortening of learning curve and widespread adoption of the procedure. 6 Subsequently, MIPN recommendations expanded to include complex cT1b, and select cT2 tumors without compromising oncologic efficacy. 2,7,8
However, MIPN is associated with inherent risk for conversion to open surgery. Such conversion has been associated with prolonged operative time, increased risk of blood transfusion, morbidities, and higher odds of radical nephrectomy. 9,10 Open conversion rates in MIPN have been previously reported between 0.2% and 6%. 11 –14 However, these reports were limited to single institutional design and limited sample sizes. 11 –14 Moreover, they were typically from high-volume centers where the experience with MIPN is higher than the national average. 13,14
Evaluation of nationwide risks and predictors of open conversion could help identifying patients at risk and therefore aid patient counseling and surgical planning. Therefore, we utilized the National Cancer Database (NCDB) to analyze national indices and predictors for open conversion during MIPN in a contemporary cohort.
Materials and Methods
Source of data
A retrospective review of the NCDB was performed to identify study population. The NCDB is a quality improvement initiative sponsored by the American College of Surgeons Commission on Cancer and the American Cancer Society. 15 At its current capacity, the NCDB captures ∼70% of newly diagnosed cancer cases nationwide; and contains >34 million records of individual cancer cases gathered from >1500 Commission on Cancer-approved facilities. All the data available through the NCDB are deidentified, and therefore, the study is exempt from Institutional Review Board approval.
Study population
The NCDB was investigated to identify patients who were diagnosed with renal cell carcinoma (RCC) (International Classification of Diseases of Oncology, third editions—code C64) and subsequently underwent PN between 2010 and 2015. The surgical approach variable was only recorded since 2010, thus, only patients who underwent PN between 2010 and 2015 were included. Surgical approach included OPN, robotic partial nephrectomy (RPN), robotic converted to open, laparoscopic partial nephrectomy (LPN), and laparoscopic converted to open. The PN patient population was further subdivided into patients who underwent OPN, effective MIPN (Robotic and laparoscopic), and those who underwent a conversion from MIPN to an open procedure.
Covariates
Patient clinical and sociodemographic variables were analyzed, including age, gender, year of diagnosis, ethnicity, health status based on Charlson–Deyo score (comorbidity index), geographical region within the United States, insurance status (private, Medicare, Medicaid/other governmental insurance, Uninsured), income, and educational level.
We also abstracted data on treatment facility-related variables, including facility type (community cancer program, comprehensive community cancer program, academic/research program, and integrated network), geographic location (Northeast, Atlantic, Southeast, Great Lakes, South, Midwest, West, Mountain, and Pacific), and distance to treatment facility. Hospital average yearly volume was calculated by dividing the number of entries from each treatment facility by the total study period in years. Treatment facilities were then stratified according to the median number of procedures per year into low-, medium-, and high-volume hospitals.
Statistical analysis
We utilized Pearson chi square and Mann–Whitney U test to compare patient and facility variables between converted and nonconverted cases. Incidence trends of utilization of MIPN as well as trends in conversion to open surgery were analyzed. Statistical significance was evaluated using the Cochrane–Armitage test for trend. Multivariate logistic regression models were utilized to identify independent predictors of conversion to OPN. All statistical analyses were performed using Stata 13.1, with two-sided significance level set at p < 0.05.
Results
Between 2010 and 2015, we identified 54,246 patients who were diagnosed with RCC and subsequently underwent PN (Fig. 1). During the study period, MIPN accounted for 35,252 procedures (64.9%), while OPNs accounted for 18,994 procedures (35.1%). Among patients undergoing MIPN, 1010 (2.87%) patients were converted to OPN. Conversion rates were 2% for patients undergoing RPN and 6.9% for LPN (p < 0.001).
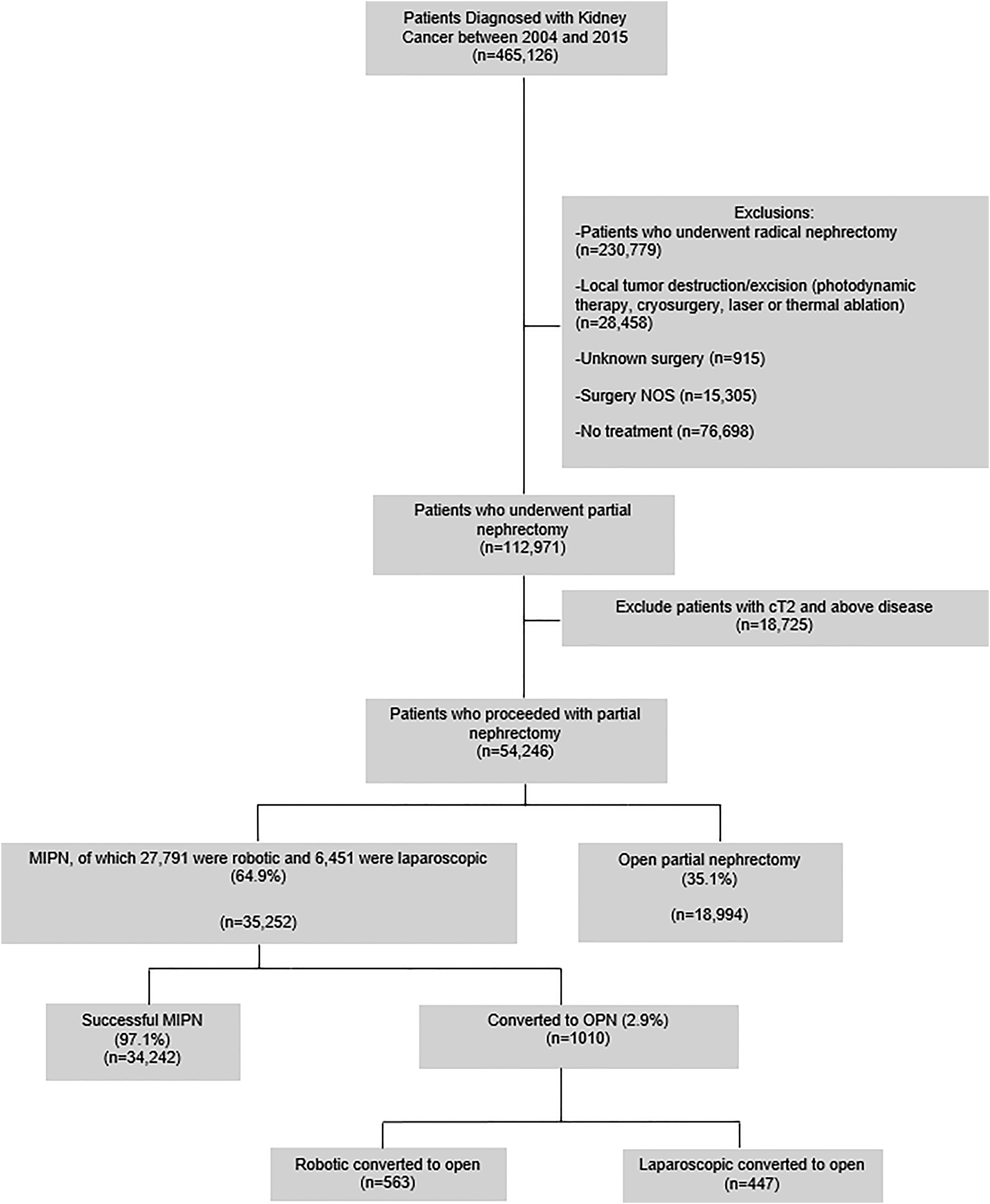
Distribution of partial nephrectomy patients identified through the NCDB screen. MIPN = minimally invasive partial nephrectomy; NCDB = National Cancer Database; NOS = not otherwise specified; OPN = open partial nephrectomy.
The ratio of MIPN to total PNs increased from 50.35% in 2010 to 74.73% in 2015 MIPN (Fig. 2). Concomitantly, conversion rates decreased during the data period from 4.75% in 2010 to 2.44% in 2015 (p < 0.001) (Fig. 3).
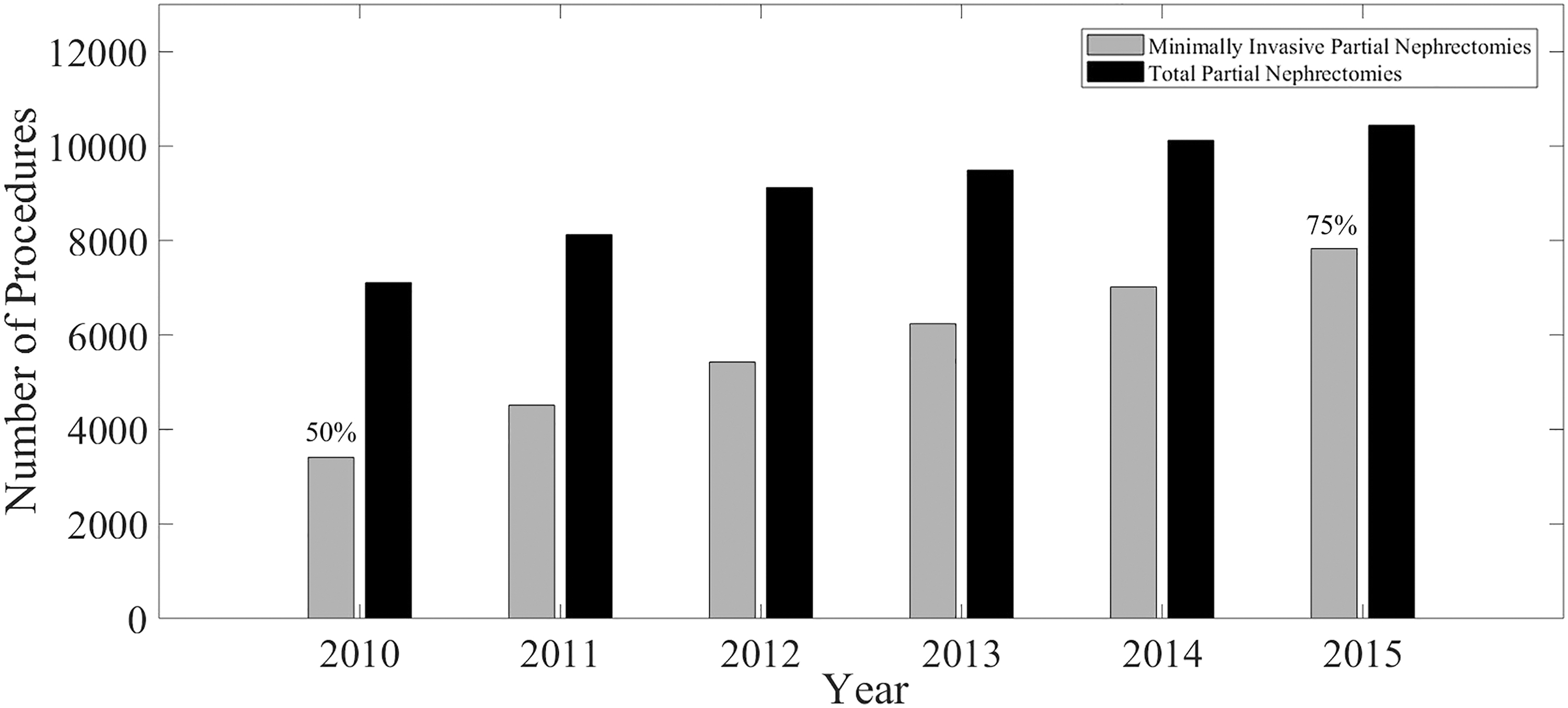
Annual MIPN procedures as proportion of all partial nephrectomies in the NCDB.

Conversion rates to OPN from MIPN procedure by year in NCDB Screening.
The rates of conversion for low-, intermediate-, and high-volume centers were 3.5%, 3.0%, and 1.8%, respectively (p < 0.001). Patients who required conversion were not significantly different in terms of margin positivity compared to nonconverted cases. Open conversion was associated with a higher likelihood of readmission within 30 days (5.95% vs 3.31%, p < 0.01) and higher likelihood of 30- and 90-day mortality (0.87% vs 0.25% and 1.25% vs 0.42%, respectively, p = 0.001). Among patients who were converted to OPN, 4.88% of patients were pathologically upstaged to ≥pT3a (p < 0.001). Clear Cell RCC was the dominant histologic subtype in the two groups representing ∼64% with no significant difference in histologic subtypes noted between the groups (p = 0.602) (Table 1).
Sociodemographic Characteristics of Patient Who Underwent Minimally Invasive Partial Nephrectomy vs Those Who Were Converted to Open Partial Nephrectomy
CCI = Charlson-Deyo comorbidity index; NOS = not otherwise specified; NS = not specified; RCC = renal cell carcinoma.
Multivariate logistic regression modeling identified male sex (compared to female, odds ratio [OR] 1.26, confidence interval [CI] 1.11–1.44, p < 0.001), Governmental insurance (Medicaid compared to private insurance, OR 1.75, CI 1.39–2.19, p < 0.01) as independent predictors of conversion. Predictive factors associated with a lower likelihood of conversion were advancing year of diagnosis (2015 vs 2010, OR 0.59, CI 0.47–0.73, p < 0.001), robot approach (compared to laparoscopic, OR 0.31 CI 0.27–0.35, p < 0.001), and treatment at high-volume facilities (compared to low volume, OR 0.52; CI 0.44–0.62, p < 0.001) (Table 2).
Multivariate Regression Analysis of Predictors of Conversion to Open Partial Nephrectomy
PN = partial nephrectomy.
Comment
The adoption of MIPN has increased in recent years relative to OPN with substantial evidence of comparable efficacy and long-term outcomes. 6 Our findings suggest that MIPN has gained strong positioning in the management of localized RCC over the course of the study period and has become the dominant surgical approach. We observed a significant increase in percentage of MIPN to all PNs from about 50% in 2010 to 76% in 2015. This was also associated with overall increase in utilization of PN. In fact, the number of MIPN procedures performed alone in 2015 (7017 cases) is comparable to the total number of all PN performed in 2010 (7108 cases). This may be attributed to increase in rate of diagnosis of small renal masses as well as increased adoption and expansion of the indications of PN. Although conversion to OPN is a rare event, it eliminates the proposed advantages of minimally invasive surgery. We observed a significant concomitant decrease in conversion rates, dropping from 4.75% in 2010 to 2.44% in 2015. As a specialty, this significant improvement in outcomes over few years associated with increased case volumes is intriguing.
Previous cohorts have reported rates of conversion to radical nephrectomy 0% to 5.5% or any open nephrectomy 0.2% to 6%. 11 –14 One group reported a rate of conversion from RPN to radical minimally invasive nephrectomy as 4.99% and reported only a single case of conversion to OPN (0.2%). 10 This raises an interesting question of current practice patterns for nephron sparing surgery when MIPN is not effective. Previous reports showed that emergent hemorrhagic complications were rarely the reason for conversion to either RN or OPN, and conversion is most frequently a result of unexpected tumor complexity or concern for positive margins or failure to progress. 16,17 While conversion to OPN could be a major retreat from the advantages of MIPN, it might not be a surgical failure. However, it can in some circumstances be an attempt to complete the initially intended PN, which provides equivalent oncologic control to radical nephrectomy, while at the same time preventing or delaying chronic kidney disease and subsequent cardiovascular morbidity and mortality. 18 –21
Our data showed that high-volume centers were associated with lower likelihood of conversion irrelative of the facility type. This volume-outcome relationship has been reported in previous studies, pertaining to a number of high-risk urologic interventions. Academic centers may have a higher number of complex cases, and thus may not achieve superior outcomes well described for a number of urologic conditions at high-volume centers. 22,23 Although centralization of cancer care allows for efficient delivery of cancer treatment with proposed improved outcomes, centralizing health care is associated with downsides. Reported consequences of regionalization included longer commute distances for patients, lack of local support systems, difficult access to high-volume hospitals, and detrimental effect on quality of care in lower volume hospitals. 24,25
Male sex in this study was associated with an increased OR of conversion to OPN on multivariate analysis. This has been previously demonstrated in other studies. 26,27 Previous studies have reported that male gender among obese patients, and not obesity itself, was an independent predictor of greater estimated blood loss, operative time, warm ischemia time, and postoperative complications. 28,29 Body mass index was not significant on multivariate analysis, which may indicate that male gender affects not only the quantity but also the quality of adipose tissue around the renal unit, making dissection more difficult. Male sex, independent of obesity, has also been associated with increased perirenal adhesions and high-grade renal malignancy during PN. 30,31 The quality of perinephric fat may be a significant host-related risk factor for surgical difficulty. Adherent perinephric fat (APF) or “sticky fat” was described. 32 One study previously identified an increase in cytokine perinephric fat in individuals with more APF, which may explain the pathophysiology of this risk factor. 33
Our analysis demonstrated that governmental insurance was also an independent predictor of conversion. Medicaid insurance, and more specifically, the lack of private insurance, was previously associated with perioperative events in PN. 34 Medicaid patients are a subset of patients who typically share a disadvantaged socioeconomic profile and it often reflects on their outcomes and measured quality-of-care metrics. 35 A previous report similarly showed that Medicaid patients are less likely to receive RPN. 36 Furthermore, when compared to private insurance, Medicare and Medicaid patients were found to have worse outcomes after PN; namely higher rates of transfusion, prolonged hospital stay, and higher rates of postoperative complications. 35
Multivariate analysis also associated robotic MIPN with lower risk of open conversion compared to laparoscopic approach. A recent analysis of the RECORD2 multicenter registry found robot approach to have lower rates of open conversion than laparoscopic PN; in addition to achieving superior rates of trifecta than laparoscopic or open PN in tumors with PADUA scores <10. 37
In the study population, 20% of patients were older than 70 years. This finding may raise concerns for underuse of Active Surveillance (AS) in this subset of patients. AS is a viable option for management of small renal masses and complex renal cysts in elderly patients and those with comorbid conditions. 2 It was shown to be noninferior to PN in patients older than 70 years as these patients have an estimated competing risk mortality of 28% vs a cancer-specific mortality of <5%. 38,39 Nevertheless, this finding can be explained by the study duration (2010–2015) when interest in AS was not at the same current level. Future studies should evaluate adoption of AS after strong endorsement in the 2017 update of the AUA guidelines. 2
To our knowledge, this is the first contemporary nationwide analysis of incidences and predictors of conversion to open surgery in MIPN. However, our results are to be interpreted within the inherent limitations of NCDB and retrospective study design. Important factors such as body mass index, tumor location, size, and complexity and nephrometry scores were not captured in the NCDB. These factors have been proved to be important predictors of outcomes and risks of conversion and hence are important for patient selection. Furthermore, data regarding estimated blood loss, ICU admission, and other markers of serious hemorrhagic complications were not recorded and would have offered valuable insight. In addition, reasons for open conversion (such as massive bleeding, concerns regarding positive surgical margins, or failure of surgery progression) and surgeons' level of training were also not available. Moreover, the rate of conversion to radical nephrectomy rather than an OPN could not be estimated.
Conclusions
Over the data period, open conversion in MIPN occurred in 2.87% of the cases. There was an observed increased trend in utilization of MIPN to represent 74.73% of all PNs in 2015. This was also associated with decreased conversion rates. Higher volume hospitals, robotic approach, and progressing year of surgery were associated with less likelihood of conversion. Male gender and governmental insurance were associated with higher risks of conversion. Further research is needed to identify case-specific reasons for conversion as well as risk stratification and insights into the patient and system-related consequences of unplanned conversion.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.