
Abstract
Introduction:
To improve the outcomes and extend the adaptation of salvage surgery for intractable urinary tract problems, this study retrospectively investigated indications and outcomes of retroperitoneal surgery based on retroperitoneal laparoscopic ureterolysis (RLU), in which the ureter is dissected with or without nephrolysis.
Patients and Methods:
Twenty-three salvage surgeries based on RLU were performed on 22 patients at our hospital between November 2002 and July 2017. Intractable urinary tract problems included lower urinary tract dysfunctions, refractory urinary fistulas, middle or lower ureter troubles, ureteroileal anastomotic strictures, and stomal stricture of cutaneous ureterostomy. After RLU, various urinary tract reconstructions were performed through minimal laparotomy under a retroperitoneal approach.
Results:
In all patients, RLU secured a sufficient length of ureter for subsequent urinary tract reconstructions, irrespective of intra-abdominal adhesions. Twelve cutaneous ureterostomies, one reconstruction of cutaneous ureterostomy, two ureteroileal reanastomoses, and five ureterovesicostomies were effectively performed after unilateral RLU. Three retroperitoneoscopic transureteroureterostomies with cutaneous ureterostomy were reconstructed after bilateral RLU. Over a median follow-up of 8 months (interquartile range, 2–80 months), two patients (8.7%) required additional procedures.
Conclusions:
Retroperitoneal salvage surgery based on RLU appears useful to salvage intractable urinary tract problems, avoiding intra-abdominal adhesions and securing a sufficient ureteral length for subsequent urinary tract reconstructions. This surgical procedure is minimally invasive and contributes to improving patient quality of life.
Introduction
Dealing with intractable urinary problems resulting from a past operation, radiation therapy, or tumor enlargement is difficult. These patients often show several other problems, such as comorbidities, infection, or short life expectancy, and performance status might be poor. Minimally invasive surgery is needed to minimize the physical burden on patients when salvage surgery for intractable urinary tract problems is performed. We have performed minimally invasive salvage surgeries conducted based on retroperitoneal laparoscopic ureterolysis (RLU), and perceived the retroperitoneal laparoscopic approach to intractable urinary troubles as easier than the transperitoneal laparoscopic approach because of fewer adhesions in the retroperitoneal space despite severe intraperitoneal conditions. 1,2 To examine the utility of salvage surgery based on RLU for intractable urinary tract problems, the indications and outcomes of the surgery were retrospectively researched.
Patients and Methods
Twenty-two patients underwent salvage surgeries based on RLU in our hospital between November 2002 and July 2017. All cases underwent RLU, in which the ureter was dissected with or without nephrolysis through a retroperitoneal laparoscopic approach, followed by various kinds of urinary tract reconstruction because the conventional transperitoneal approach seemed likely to encounter difficulties from strong intra-abdominal adhesions. All patients were followed by blood analysis and/or imaging (i.e., ultrasonography, computed tomography, and drip infusion pyelography). Clinical data including operative parameters, type of the urinary tract problem, primary diseases, chief complaints, history of radiation therapy, and/or intra-abdominal surgery were retrospectively obtained from hospital records. This retrospective study was approved by the institutional review board at Tohoku University Hospital.
Results
Twenty-three salvage surgeries based on RLU were performed in 22 patients (15 men, 7 women; Table 1). Median age was 61 years (interquartile range [IQR], 46–71 years). Median follow-up period after the operation was 8 months (IQR, 2–80 months). Operative parameters, types of urinary tract problems, primary diseases, and chief complaints are listed in Table 1 and Supplementary Table S1. Radiation therapy to the pelvic area had been performed for 9 patients (39%) and intra-abdominal surgeries had been performed for 19 patients (83%). Patients showed various urinary tract problems, that is, lower urinary tract dysfunction because of intrapelvic tumors or contracted bladder, middle or lower ureter troubles including ureter injury, stricture, or obstruction, refractory urinary fistulae caused by chemoradiation or intrapelvic infection, ureteroileal anastomotic stricture after ileal urinary tract diversion (three ileal conduits and one neobladder), and stomal stricture of cutaneous ureterostomy.
Characteristics of the 22 Patients and 23 Salvage Retroperitoneal Laparoscopic Surgeries
IQR = interquartile range.
Retroperitoneal laparoscopic ureterolysis
At first, RLU was performed with the patient in the lateral or supine position. 1,2 Representative port positions are shown in Figure 1. On the required side, retroperitoneal space was carefully dilated using a balloon dissection technique and the ureter without adhesions was found. The ureter was peeled off craniocaudally and transected at the level of common iliac artery, where adhesions were strong in most cases. Median time of ureterolysis was 45 minutes (IQR, 35–85 minutes).
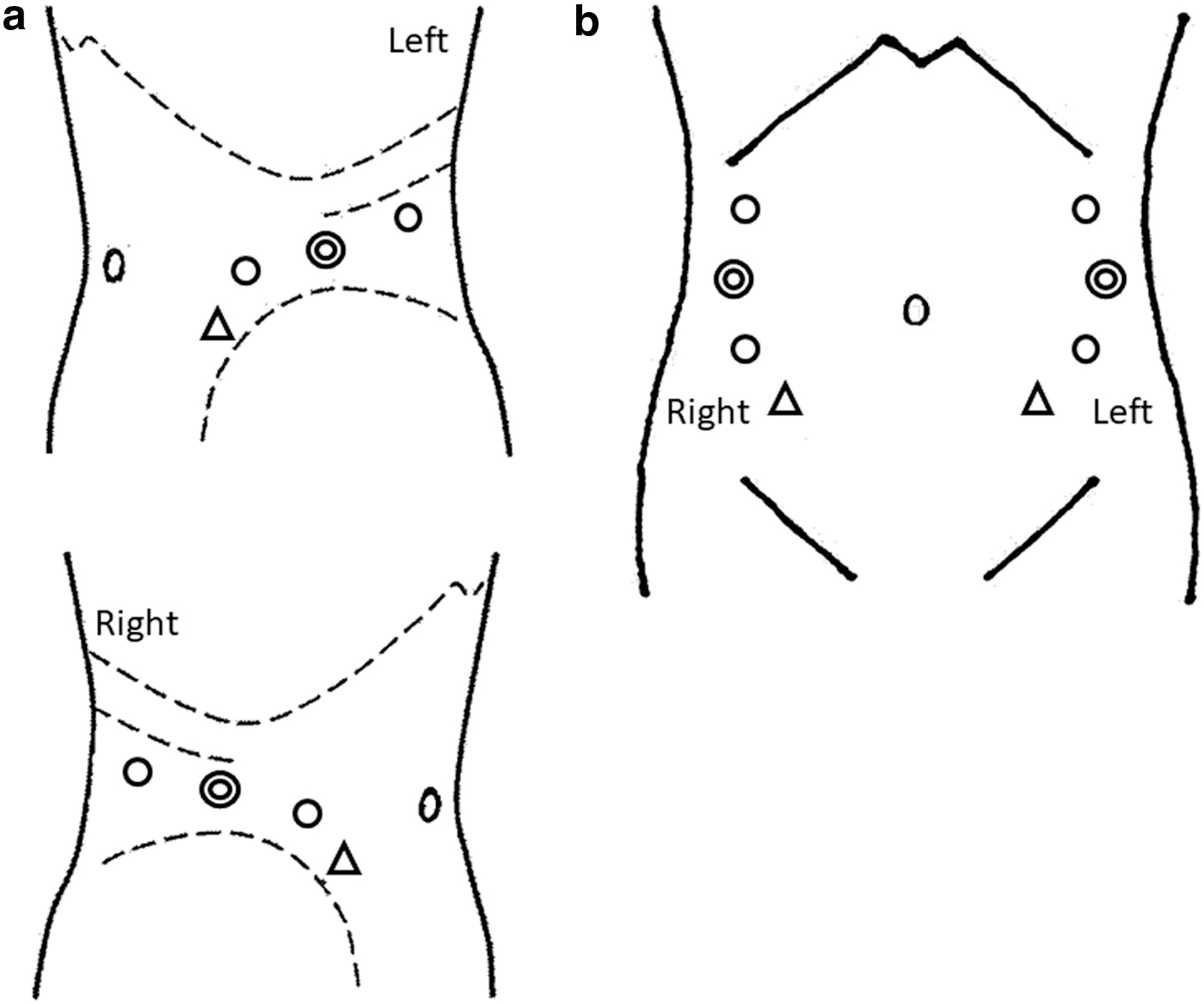
Representative port positions. In all cases, the laparoscopic procedure was performed under a retroperitoneal approach.
Various kinds of urinary tract reconstruction
In all patients, RLU secured a sufficient length of ureter for the subsequent urinary tract reconstructions. After RLU, cutaneous ureterostomy, reconstruction of cutaneous ureterostomy, ureteroileal reanastomosis, ureterovesicostomy, or transureteroureterostomy with cutaneous ureterostomy was performed.
Cutaneous ureterostomy after RLU: To block urinary flow into the bladder for resolution of severe urinary symptoms, cutaneous ureterostomy at the laparoscopic port site was performed after RLU for seven cases with lower urinary tract dysfunctions and five cases with refractory urinary fistulae (Fig. 2). All patients showed poor performance status and most patients had short life expectancies. Bilateral cutaneous ureterostomies were constructed in 2 cases, but a unilateral procedure was selected in the remaining 10 cases. Contralateral renal embolization was added to make the bladder dry to improve quality of life in two patients with a normal contralateral kidney. In six cases (50%), patients were transferred to the hospice or died within 3 months. Cases with intractable bladder problems. Retroperitoneal laparoscopic cutaneous ureterostomy was performed. 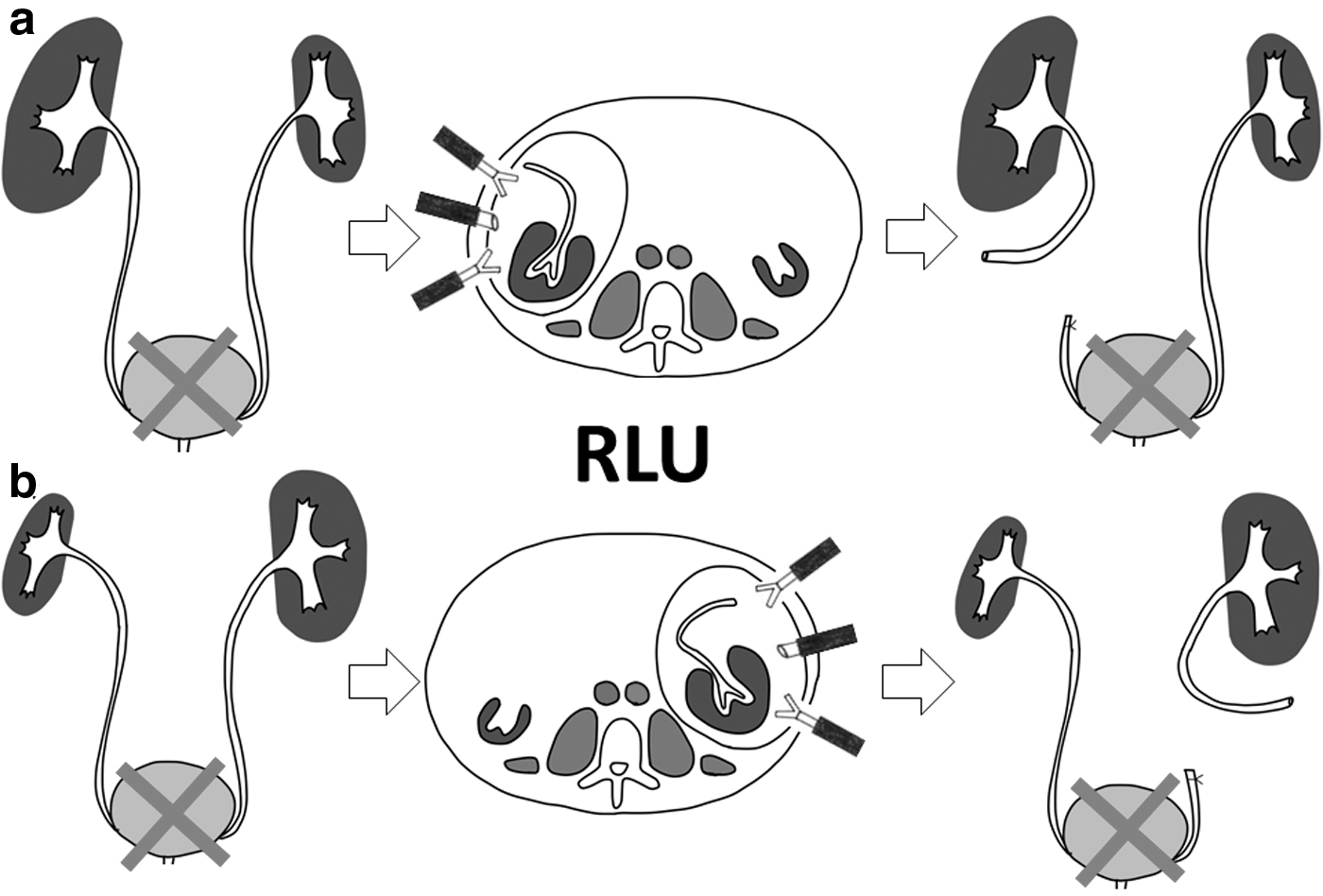
Reconstruction of cutaneous ureterostomy after RLU: For stomal stricture of the cutaneous ureterostomy, cutaneous ureterostomy was reconstructed at a different site after RLU in one case with right ureteroileal anastomotic stricture (Fig. 3). A case with right stomal stricture of cutaneous ureterostomy. Right cutaneous ureterostomy was reconstructed after RLU.
Right ureteroileal reanastomosis after RLU: For unilateral ureteroileal anastomotic stricture of the right side, RLU was performed followed by ureteroileal reanastomosis through open mini-laparotomy under a retroperitoneal approach for one case of neobladder (Fig. 4a) and in one case of ileal conduit (Fig. 4b). Cases with right ureteroileal anastomotic stricture. Right ureteroileal reanastomosis was performed after RLU. 
Ureterovesicostomy after RLU: Although constructing tension-free ureterovesicostomy appeared difficult for five cases with middle or lower ureter trouble with contracted bladder or short intact ureter, maximal nephrolysis and ureterolysis by RLU allowed tension-free ureterovesicostomy (Fig. 5). Cases with intractable middle or lower ureter troubles. Ureterovesicostomy was performed after retroperitoneal laparoscopic maximal nephrolysis and ureterolysis.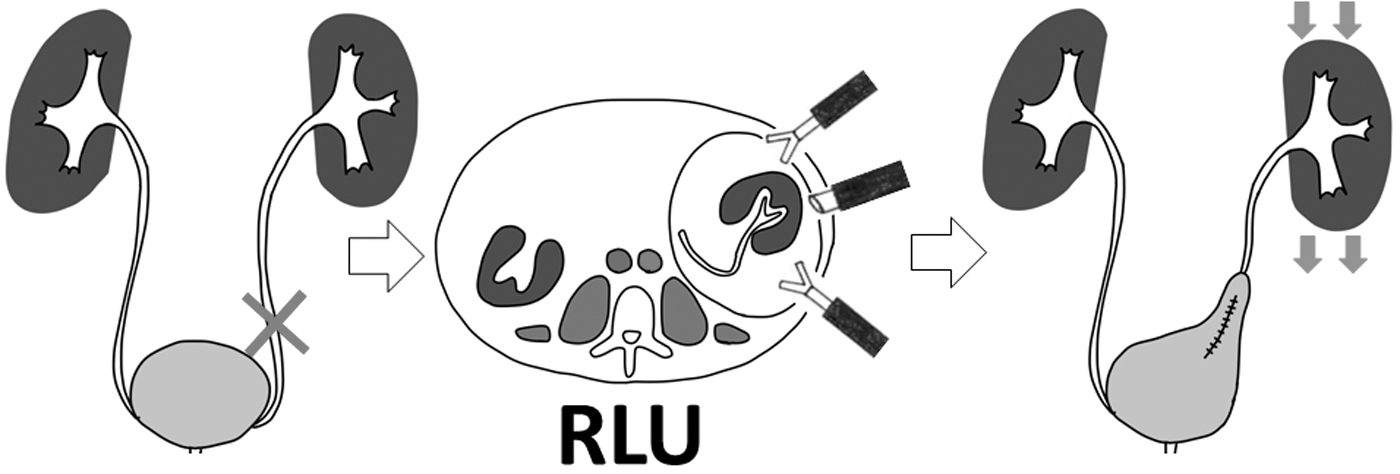
Retroperitoneoscopic transureteroureterostomy with unilateral cutaneous ureterostomy: For patients with bilateral ureteroileal anastomotic strictures or with refractory ileal conduit-perineum fistula, retroperitoneoscopic transureteroureterostomy with unilateral cutaneous ureterostomy
2
was performed. First, RLU was performed on the left side. The left ureter was peeled off and transected at the level of left common iliac artery through a left retroperitoneal laparoscopic approach. The retroperitoneal space was further extended in front of the aorta and vena cava superior to the inferior mesenteric artery (IMA), at which point the end of the left ureter was placed. Next, RLU was performed in the right retroperitoneal space. The right and left retroperitoneal spaces were connected and the left ureter was transposed to the right side through the retroperitoneal tunnel. The end of the left ureter was anastomosed to the side of the right ureter. Finally, unilateral cutaneous ureterostomy at the laparoscopic port site was constructed in three patients (Fig. 6c). Cases with bilateral ureteroileal anastomotic stricture. (1) The left ureter was peeled off and transected at the level of the left common iliac artery through a left retroperitoneal laparoscopic approach, then transposed to the right side through the retroperitoneal tunnel. (2) Right ureterolysis was performed through a right retroperitoneal laparoscopic approach and the left ureter was identified through the retroperitoneal tunnel. 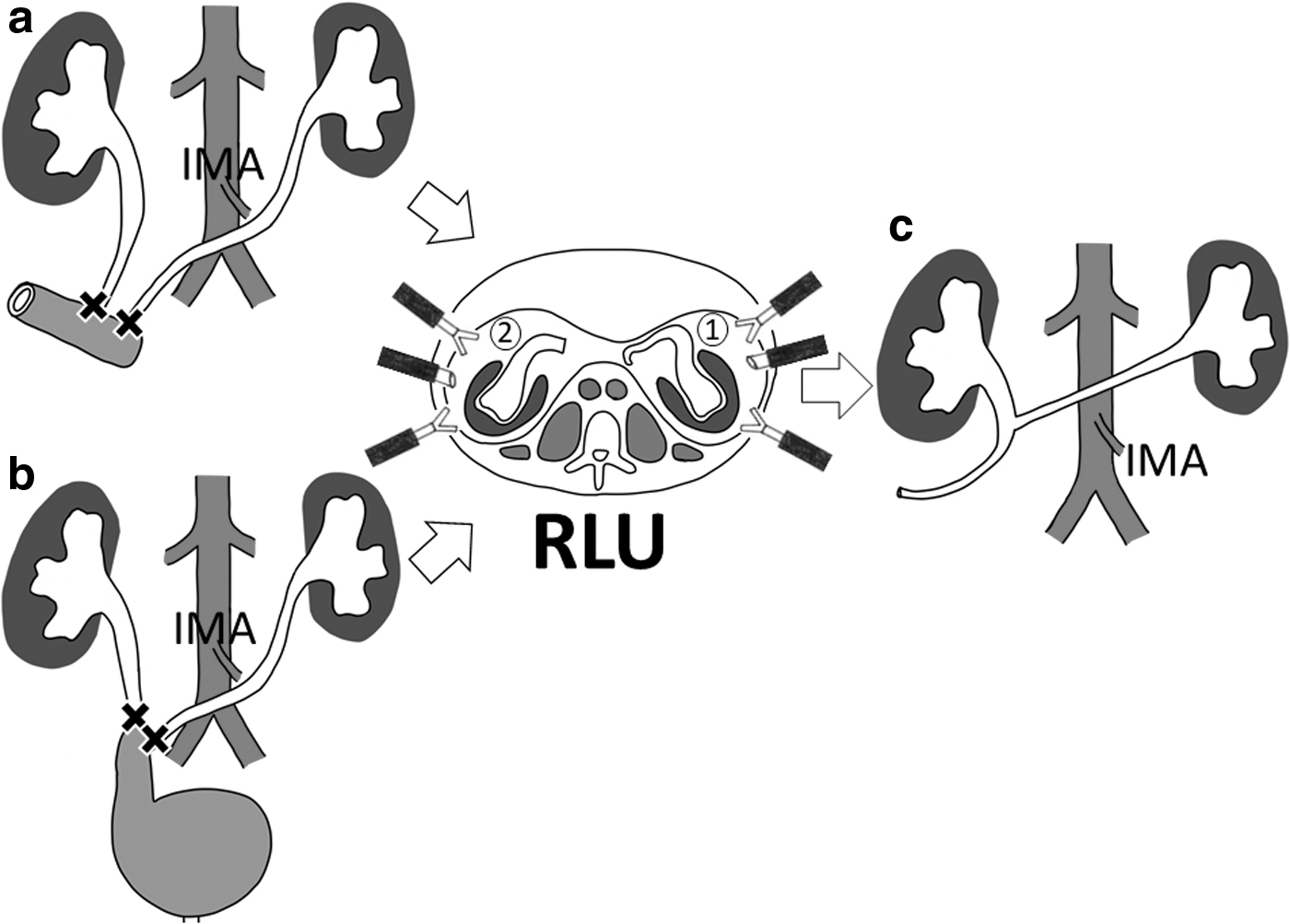
After these salvage surgeries, urine passage was restored in nine cases, urine leakage from fistulas improved in five cases, severe pain symptoms were improved in four cases, the bladder was made dry through urinary diversion to improve severe symptoms in four cases, and recurrent urinary tract infections were improved in one case. No additional treatment was required for 21 procedures (91.3%) with a median follow-up of 8 months (IQR, 2–80 months) and the durable patency rate over the 12 months follow-up period was 83.6%. Two cases (8.7%) required an additional operation after urinary tract reconstructions. In the case of one patient who underwent retroperitoneoscopic transureteroureterostomy with cutaneous ureterostomy for refractory ileal conduit-perineum fistula, renal function deteriorated because of anastomotic stricture and bilateral nephrostomies were eventually required. The remaining one case who had experienced improvement of continence after unilateral salvage cutaneous ureterostomy claimed reappearance of incontinence after 12 months. He underwent contralateral cutaneous ureterostomy after RLU.
Discussion
Salvage surgery for intractable urinary problems is technically challenging because of severe tissue adhesions from past operations, radiation therapy, or tumor enlargement. Nevertheless, interventions need to be less invasive and show a higher success rate, because the patients often have several other problems such as comorbidities, infection, poor prognosis, or poor performance status. Traditionally, open salvage surgery has been chosen for such patients, but laparoscopic approaches have been developed because of the less invasive procedure. 3 –5 In cases with intra-abdominal adhesions, the retroperitoneal approach seems more feasible than the transperitoneal approach because fewer adhesions arise in the retroperitoneal space despite severe intra-abdominal conditions. We have introduced RLU as a basic procedure for urinary tract reconstructions. The retroperitoneal laparoscopic approach was a less invasive procedure that enabled us to constantly secure ureters of sufficient length to reconstruct the urinary tract. In all 23 procedures, RLU was effectively performed and followed by various kinds of urinary tract reconstructions tailored to the status of each patient. Our results indicate that RLU is useful as a basic procedure taking advantage of the retroperitoneal laparoscopic approach during salvage surgery for intractable urinary problems.
Various kinds of urinary tract reconstructions such as cutaneous ureterostomies, ureteroileal reanastomoses, ureterovesicostomies, and transureteroureterostomy with cutaneous ureterostomy had been described in this report. In cases of urinary rediversion, previous studies have reported that complications after urinary tract reconstructions using intestinal tract are common and reoperations are inescapably required at a certain percentage for a variety of reasons. 6 Fifty-four percent and 35.7% of patients required reoperations for urinary tract reconstructions using intestinal tract by Pahernik and colleagues and Liedberg and colleagues, respectively. 6,7 In addition, Chang et al. reported that a history of radiation therapy should not serve as an absolute contraindication for salvage surgery, but attention must be paid to the use of ileum because of postoperative morbidity. 8 In our report, additional treatment was required in only two cases (8.7%). Although the short follow-up was a clear contributor to the small number of reoperations, we consider that another reason might be the small number of urinary tract reconstructions using intestinal tract, because most patients showed poor performance status or poor prognosis, resulting in the low frequency of additional treatment.
Ureteroileal anastomotic stricture is one of the major problems after radical cystectomy. 9 For patients with unilateral ureteroileal anastomotic stricture of the right side, ureteroileal reanastomosis is usually required for urinary tract reconstruction. Right RLU facilitates minimally invasive ureteroileal reanastomosis laparoscopically or through open mini-laparotomy. In cases of left-side or bilateral ureteroileal anastomotic stricture, however, ureteroileal reanastomosis is difficult to perform after RLU because access to the ileal conduit is not usually an easy procedure on the left side. Although several articles have recently reported effective ureteroileal anastomotic repairs using robotic surgical instruments, 10,11 left-side repair remains an issue in the future because only few reports have described minimally invasive repair for left-side ureteroileal anastomotic troubles. Transureteroureterostomy, in which the left ureter is pulled from the left to the right retroperitoneal space through the retroperitoneal tunnel superior to the IMA, is one of a few minimally invasive salvage surgeries for left-side or bilateral ureteroileal anastomotic troubles. 2 In our report, for those patients with bilateral ureteroileal anastomotic strictures or with refractory ileal conduit-perineum fistula, transureteroureterostomy followed by right-side cutaneous ureterostomy was performed.
Special attention should be paid to the indications for transureteroureterostomy. In the patient who underwent transureteroureterostomy with cutaneous ureterostomy for refractory ileal conduit-perineum fistula, anastomotic stricture occurred at the ureteroureterostomy and bilateral nephrostomies were required because of deterioration of renal function. Not so long ago, when transureteroureterostomy was performed in open surgery, an empirical statement was made that transureteroureterostomy did not work well if the recipient ureter was not dilated by obstruction of urine passage. Sufficient blood flow has been considered to correlate with effective transureteroureterostomy. 12 –14 Rainwater et al. reported that the ureter dilated by obstruction was favored in transureteroureterostomy because of the thickened ureteral wall and increased blood supply compared with the nondilated ureter. 14 Blanchard and coworkers verified that blood flow around the ureter was increased after blockage of the vessels at the ureterovesical junction in animal experiments. 15 In the case with renal function deterioration, the recipient and donor ureter are not dilated, and the blood supply might be insufficient. In each of the other three patients, in whom bilateral ureters were dilated by urinary obstruction, transureteroureterostomies proved effective.
This study showed various limitations. The most major limitation was the relatively short highly variable duration of follow-up (median follow-up, 8 months; IQR, 2–80 months). This study included patients with poor performance status and short life expectancy who were transferred to the hospice or died within a short period. Even in such cases, however, we were able to safely perform salvage surgery and no additional treatment was required in most cases. In addition, we did not use objective intraoperative methods for evaluating ureteral vascularity before anastomosis, such as near-infrared fluorescence imaging using indocyanine green, which has gained wide application in many fields of surgery for assessing blood supply. Despite the limitations seen in this investigation, retroperitoneal urinary tract reconstructions were effectively achieved in all cases and few additional treatments were required. Retroperitoneal salvage surgery based on RLU thus appears to offer an effective option in salvage surgery for intractable urinary tract problems.
Conclusions
To salvage intractable urinary tract problems, RLU is useful to avoid intra-abdominal adhesions and secure a sufficient ureteral length for anastomosis. Urinary tract reconstructions conducted based on RLU rescued patients from their intractable urinary tract problems. These salvage surgeries can also allow patients to achieve freedom from the nephrostomy catheter or nephroureteroconduit stent, even in patients with poor performance status and short life expectancy. Urinary tract reconstruction conducted based on RLU is minimally invasive and contributes to improved quality of life for patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.