
Abstract
Introduction:
To compare short- and midterm outcomes of the first 55 patients undergoing robot-assisted kidney transplant (RAKT) with patients undergoing open kidney transplant (OKT) during the same period in a tertiary care hospital.
Materials and Methods:
Data of all end-stage renal disease patients undergoing renal transplant were prospectively maintained. All graft kidneys were harvested laparoscopically. Both RAKT and OKT were performed using standardized techniques, and all RAKTs were performed by a single experienced robotic surgeon. Chi-square test/Fisher exact test was done for categorical data, and Mann–Whitney U test was done for continuous data. Discrete variables were expressed in absolute numbers and percentages. For all tests, p < 0.05 was considered significant. All results were expressed as mean ± standard deviation or median with range.
Results:
Between April 2016 and September 2018, 55 patients underwent RAKT. The same was compared with 152 patients who underwent OKT. The two groups were comparable in terms of age, gender, and body mass index. Duration on hemodialysis was significantly higher in the RAKT group, and hemoglobin and donor kidney glomerular filtration rate was significantly better in the RAKT group. Requirement of perioperative analgesia was significantly less in the RAKT group. Rewarm ischemia time was significantly longer in the RAKT group. The fall in serum creatinine was slower in RAKT group till 3 months. The serum creatinine levels were statistically similar in the two cohorts at 3 months (p = 0.082), which was maintained at median 29 months of follow-up (p = 0.067). Tacrolimus levels on postoperative day 2 were found to be significantly higher in RAKT cohort (17.98 ± 14.41) vs OKT cohort (11.38 ± 6.93). Surgical-site infections were rare in the RAKT group.
Conclusions:
RAKT confers advantage of decreased wound morbidity with similar functional outcomes compared with OKT in midterm. It looks promising; however, long-term follow-up of larger numbers of patients is needed.
Introduction
Humans, since time immemorial, were fascinated by the idea of treating diseases by organs of other humans, or transplant. It was on December 23, 1954, that Joseph Murray created history by effectively transplanting human kidney from an identical twin. Since then, the field of solid organ transplant has undergone a lot of development, but mainly in immunobiology and pharmacology. The surgical technique has essentially remained the same over the past six decades.
Open kidney recipient surgery has been well established with good functional outcomes, and there are well-documented disadvantages in terms of wound outcomes. Morbidity and wound infections are common, especially in these chronically ill, obese, diabetic, and immunosuppressed patients. Wound complications become even more glaring in obese and diabetic patients. 1 Many centers across the world avoid transplant in obese patients because of these complications and suboptimal outcomes. 2
Laparoscopic live donor nephrectomy by Ratner in 1995 paved the way for minimally invasive surgery in the field of renal transplantation. Surgery with shorter skin incision was described in a few series. The first laparoscopic renal transplant was described in 2010. Complex vascular suturing and limits of cold ischemia time (CIT) were major deterrents. It remained confined to only a few centers and never gained wide popularity. 3,4
The advent of the da Vinci® surgical system (dVSS) revolutionized minimally invasive surgery. First, robot-assisted kidney transplant (RAKT) was performed in France in 2002. 5 The kidney was placed through open incision, and dVSS was used only for anastomosis, assisted by a bedside surgeon. First, full RAKT was published by Giulianotti and colleagues from Chicago in 2010. 6 Over the past decade, rapid evolution and standardization of RAKT technique have been made. Still, RAKT is confined to a limited number of centers across the world, with majority of work being done in India, Europe, and a few American centers. RAKT is still trying to get foothold against the gold standard open kidney transplant (OKT).
Herein, we have done a prospective nonrandomized comparison between OKT and RAKT to assess functional outcomes in midterm follow-up (12–40 months) and analyze differences between the two cohorts.
Materials and Methods
Study design
It is a prospective case/control study done at a single high-volume tertiary care center. All RAKTs were done by a single surgeon (A.K.), having vast experience in both open and robot-assisted surgeries. OKTs were done by experienced transplant surgeons. The study was approved by the institutional ethics committee (TS/MSSH/SKT-2/URO/IEC/16-13).
Study sample
All end-stage renal disease (ESRD) patients (having glomerular filtration rate [GFR] ≤15 mL/minutes) presenting for live donor renal transplantation were evaluated in detail for renal transplant. Between April 2016 and September 2018, data of all consecutive patients undergoing live donor renal transplant were recorded. The patients were explained in detail about the transplant procedure, risks, and complications involved and especially about the extra financial burden of US $3000 for RAKT. Patients agreeing for robotic transplant were kept in the RAKT cohort and all others in the OKT cohort. Exclusion criteria for RAKT were more than two graft renal arteries, patients undergoing a second transplant, and patients deemed unfit for general anesthesia due to poor chest condition or cardiovascular morbidity as per preanesthesia assessment.
In all, 152 OKTs and 55 RAKTs were performed during the study period. In OKT, cadaveric donor transplants and transplant with more than two donor arteries were excluded from the final analysis.
Study variables and outcomes
Data for demographic variables, perioperative variables, functional outcomes, and follow-up were prospectively captured. Demographic variables assessed were age, gender, body mass index (BMI), duration on dialysis, preoperative hemoglobin, donor GFR, and induction method. Human leukocyte antigen (HLA) matching was done for all biologically related donors. Induction was done with antithymocyte globulin 3 mg/kg body weight in emotionally related donors and biologically related donors having <50% match. Induction with injection basiliximab 20 mg on day 0 and 4 was done when biologically related donors had 50% HLA matching or more. In few cases with 100% HLA match, induction was omitted.
Perioperative variables assessed were blood transfusion, analgesic use, warm ischemia time (WIT), CIT, rewarm ischemia time (reWIT), surgical complications, and mortality rate at day 90. Functional outcomes assessed were serum creatinine at days 7, 30, and 90, and then periodically till last follow-up. First, tacrolimus level assessment was done at postoperative day (POD)-2 of surgery. Any graft dysfunction had biopsy to see for biopsy-proven acute rejections (BPARs) or acute tubular necrosis (ATN). Biopsy was uniformly done under real-time ultrasound guidance; difficulty due to bowel interposition was not encountered in RAKT as graft kidneys were uniformly retroperitonealized.
WIT was calculated as the time duration from application of main renal artery clip to start of ice-cold perfusion. CIT was calculated from start of ice-cold perfusion till kidney was taken out of ice slush for engraftment. reWIT was calculated from removal of kidney from ice slush till restoration of renal graft perfusion.
Surgical procedure
The graft kidney was uniformly retrieved using laparoscopic donor nephrectomy. Following retrieval, the graft kidney was immediately transferred to ice slush and perfusion started with ice-cold organ preservation solution histidine-tryptophan-ketoglutarate till efflux was clear. Next, kidney was defatted with meticulous clipping of all blood vessels under 3 × magnification. Double arteries were reconstructed in a pajama manner to obtain a single stump for arterial anastomosis. In case of discrepancy in size, a smaller artery was reimplanted into the main artery (Fig. 1).
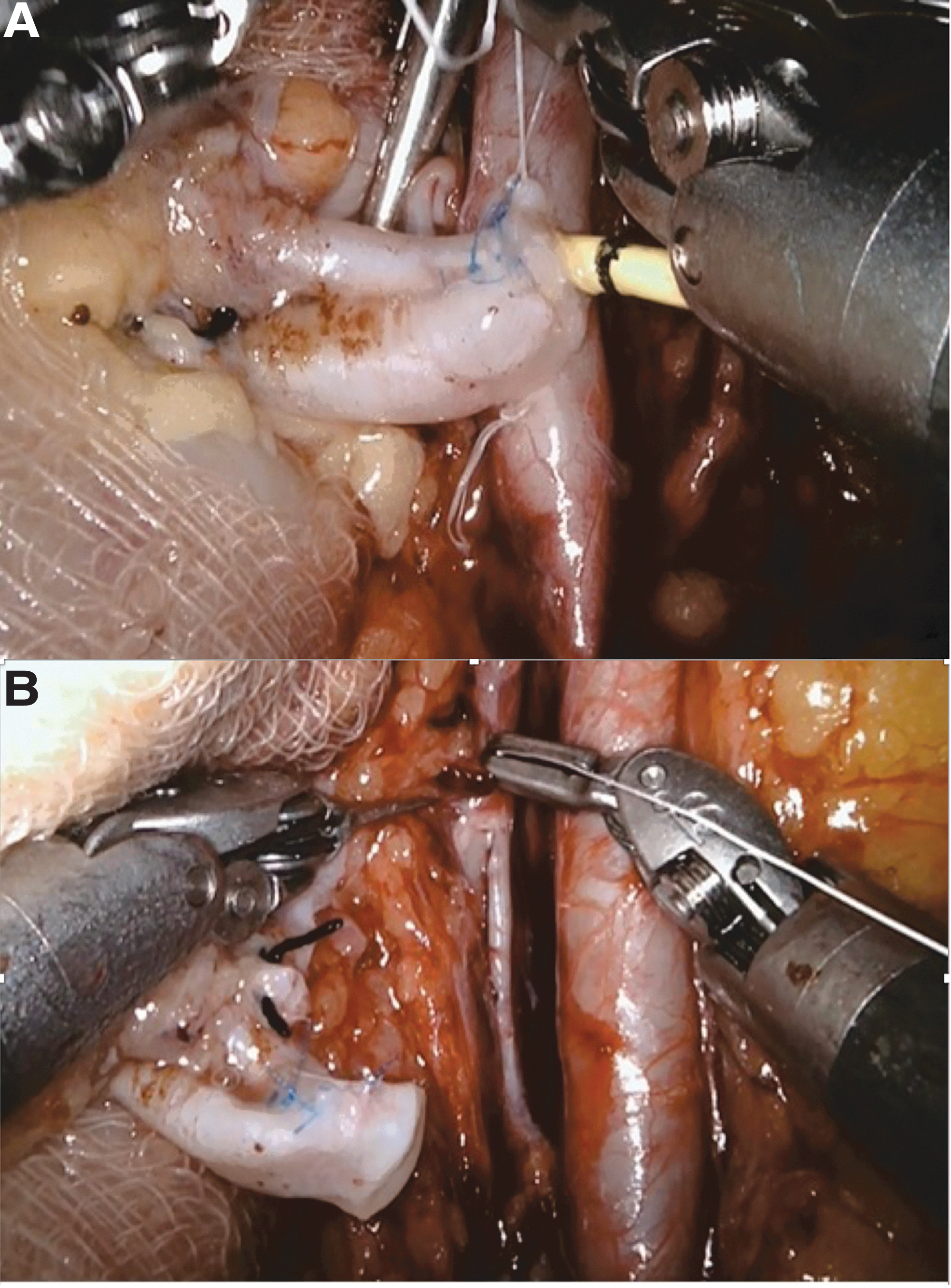
Accessory graft renal artery reconstruction.
Ice jacket was made using a gauze piece to maintain graft kidney hypothermia. Even arteries originating far apart could be managed with reconstruction after meticulous hilar dissection. The ice jacket also aided in handling of graft within a recipient, without causing injury by robotic instruments. Jacket was closed using silk suture, and the upper pole of kidney was marked by a long tail of suture used as an identification tag. Ice slush was also placed inside the pelvic cavity.
The RAKT technique was standardized by Menon and colleagues in their IDEAL phase 1–2a studies. 7,8 Briefly, after a patient was handed over by the anesthesia team, an 18F silicone Foley catheter was placed and the urinary bladder filled with diluted povidone iodine solution under gravity up to 300 mL. Catheter was clamped and port placement done. Patient was turned to 300 Trendelenburg position. da Vinci Xi surgical system (dVSS) (Intuitive Surgical, Sunnyvale, CA) was docked and bowels were retracted. Peritoneum was opened in right iliac fossa in a flap-like manner to access vessels and mobilized superiolaterally to create a space for kidney to sit in and retroperitonealized. Right external iliac vessels were prepared. Bladder was dropped and prepared for ureterovesical anastomosis.
Kidney within ice jacket was introduced into peritoneal cavity either by GelPOINT® (Applied Medical, Inc., CA) (n = 24) or by a six-centimeter Pfannenstiel incision (n = 31). GelPOINT® was preferred in obese patients with BMI of more than 30 kg/m2, and Pfannenstiel incision in patients with BMI ≤30 kg/m2. Along with kidney, blocks of ice slush were placed inside the peritoneum to maintain low temperature (as described by Menon and colleagues). Kidney was kept in position with the aid of a fourth arm of dVSS. External iliac vein was clamped with Scanlan® Reliance bulldog clamps (Scanlan International, Inc., MN), and venotomy was done using robotic Potts scissors and flushed with heparin saline using a ureteral catheter. Venous anastomosis was done using Gore-Tex CV 6-0 (W.L. Gore Medical, Inc., Flagstaff, AZ) continuous running sutures. External iliac artery was clamped using Scanlan Reliance bulldog clamps, and arteriotomy was done using robotic Potts scissors. Artery was flushed with heparin saline using a ureteral catheter, and arteriotomy refashioned with Potts scissors. Arterial anastomosis was done using Gore-Tex CV 6-0 continuous running sutures. Graft perfusion was restored, and hemostasis ensured.
Modified Lich-Gregoir ureteroneocystostomy was done with a 6F 16 cm Double-J stent using polyglactin 910 (Ethicon, Inc., NJ) 4-0 continuous running sutures and the tunnel was refashioned using the same suture. Kidney was placed in the iliac fossa and peritoneal flap was reapproximated using Weck Hem-o-lok® clips to retroperitonealize the graft. Abdominal drain was placed and all port sites and insertion wound were closed in layers (Fig. 2).

Cosmetic outcome in male patient with body mass index 47 kg/m2.
OKT was performed in a standard manner using hockey stick incision. Right or left iliac vascular and ureteral anastomoses were done in the same manner as in robotic surgery.
Follow-up protocol
After surgery, patients were kept hospitalized for 7 days as a protocol. They were intensively monitored by body weight, urine output, hemodynamic parameters, and laboratory parameters. Indwelling Foley catheter was removed on POD 5 and drain on 2nd POD in RAKT/output less than 50 mL/24 hours in OKT. The tacrolimus/cyclosporine dosage was modified. Patients were followed twice weekly for 1 month.
After 1 month, outstation and international patients were referred back to their primary physicians. Other patients were followed as per institutional protocol. Patient's follow-up status was tracked using telephonic calls and emails, or review visits and data were maintained on Microsoft Excel sheet.
Any patient with rising serum creatinine was evaluated for calcineurin inhibitor levels, infection, and color Doppler ultrasound assessment of graft kidney. Graft biopsy was done as per clinical indications and patients managed accordingly.
Statistical analysis
Data were prospectively maintained. Comparison was done for donor GFR, recipient age, BMI, duration on dialysis, and preoperative hemoglobin. Chi-square test/Fisher exact test was done for categorical data, and Mann–Whitney U test was done for continuous data. Discrete variables were expressed in absolute numbers and percentages. For all tests, p < 0.05 was considered significant. Data were maintained on Microsoft Excel sheet, and SPSS v.24 (IBM, Inc., NY) was used for statistical analysis. All results were expressed as mean ± standard deviation or median with range.
Results
A total of 152 OKTs and 55 RAKTs were performed during the study duration. Demographic results, operative variables, and functional outcomes are summarized in Table 1.
Demographic Characteristics, Perioperative Variables, and Functional Outcomes
ATG, antithymocyte globulin; ATN = acute tubular necrosis; BMI = body mass index; CIT = cold ischemia time; GFR = glomerular filtration rate; HD = hemodialysis; OKT = open kidney transplant; RAKT = robot-assisted kidney transplant; SD = standard deviation; WIT = warm ischemia time.
Age of recipient, gender, and BMI were comparable between the two cohorts. Duration on hemodialysis (HD) was significantly higher in the RAKT group; hemoglobin rate and donor kidney GFR were significantly better in the RAKT group. Induction in RAKT group was skewed toward injection basiliximab probably because of better HLA matching between donors and recipients.
WIT and CIT were similar between the two cohorts. reWIT and blood transfusion were significantly higher in the RAKT cohort. The serum tacrolimus levels on POD-2 were also higher in the robotic cohort. Serum creatinine was significantly higher in the RAKT cohort at days 7 and 30, but became comparable by 3 months. On further follow-up, serum creatinine was maintained at a median follow-up of 27 (13–40) months in RAKT and 29 (12–40) months in OKT. BPAR and ATN were comparable between the two cohorts (Table 2). Higher incidence of slower recovery of graft function in RAKT cohort could be ascribed to higher reWIT and higher initial tacrolimus levels.
Graft Dysfunctions
GelPOINT was preferred in obese patients (having BMI >30 kg/m2), led to faster re-establishment of pneumoperitoneum, and a nonsignificant decrease in reWIT. There was no difference in functional outcomes between the two subgroups. However, it added a cost of US $750 to the procedure.
In one of the morbidly obese patients (BMI 47), arterial control was not achieved by a pair of Scanlon Reliance bulldog clamps; we had to apply two pairs before attempting anastomosis. In another two obese patients, after placing the patients in a steep Trendelenburg position and docking the robot, the bowel could not be retracted out of the pelvic cavity despite multiple manoeuvers; the cases had to be converted to OKT, followed by uneventful recovery.
Surgical-site infections (SSIs) as well as re-explorations were more common in OKT group. There were four perioperative mortality rates in the OKT group (three were due to fulminant sepsis and one secondary to myocardial infarction) and one in RAKT group (secondary to sepsis-induced cerebral infarction) (Table 3). There were two noninfectious wound complications (incisional hernia) in RAKT group during our initial experience. Both the patients were morbidly obese, had sheath closure with polyglactin 910 2-0 suture, and had postoperative respiratory complications.
Complications
There was one case of arterial stenosis and ureteral stricture each in the RAKT group. The arterial stenosis patient presented around 8 months post-transplant with raising serum creatinine. On evaluation, graft artery stenosis was diagnosed and managed with percutaneous transluminal angioplasty and stenting. Postprocedure, creatinine returned to baseline and is currently stable. The second patient presented around 3 months post-transplant with rising serum creatinine. He was diagnosed with hydronephrosis of graft kidney and was stabilized with US-guided per-cutaneous nephrostomy placement. After antegrade stenting failed, he was managed with native ureter to graft pelvis ureteropyelostomy.
In another case, the patient had increased drain output and was explored immediately. In view of only diffuse oozing seen, the wound was closed. Postoperatively, he developed sepsis with decreasing output and deteriorating graft function. First graft biopsy revealed ATN. Patient failed to improve on conservative management, and repeat evaluation revealed arterial thrombosis around 3 weeks post-transplant with cortical necrosis on repeat biopsy. Patient subsequently became dialysis dependent.
Discussion
OKT has been well established over the past six decades with proven functional outcomes. The surgical technique has been well defined and is carried out with little variation across different centers. Surgical complications are not common. However, these already debilitated patients have to bear with all the disadvantages of open surgery such as pain, poor cosmetic outcomes, and a higher risk of wound complications. The disadvantages are even more obvious in obese and diabetic patients. In this subgroup of patients, wound infection rates are higher and are associated with inferior graft outcomes. 1,9
The emphasis being on functional outcomes, literature is still silent on the cosmetic aspects of kidney transplantation. Although cosmetic aspects are often neglected in potentially life-threatening diseases such as ESRD, patients do yearn for better cosmetic outcomes if given a choice. This is especially more marked in case of young girls and children. 10 One of our patients consented for renal transplant only after she was convinced regarding better cosmetic outcomes with RAKT.
A randomized-controlled trial would be ideal to compare RAKT against OKT; significant cost difference between the two arms (US$ 3000) makes it difficult to justify randomization. Second best is propensity-matched comparison. Wide variation in demographic characteristics of our patient population made it difficult to do the matching. Herein, we have compared our first 50 cases of RAKT with 152 cases of OKT done during the study period. The study was approved by the institutional review board.
We have followed the technique described by Menon and colleagues with intracorporeal cooling using ice slush jacket around the graft kidney. 8 As all our donors were live, WIT and CITs were comparable and constant across the series. The kidney was placed inside the abdominal cavity in RAKT via either GelPOINT or via Pfannenstiel incision. We have calculated reWIT from the point graft was removed from ice slush/placed inside the peritoneal cavity till restoration of circulation. In RAKT, additional time was required to close insertion site, manipulate the graft kidney, and apply vascular occlusion clamps, leading to higher reWIT, which is comparable with other series. 10,12,13 Usually, 10–15 minutes are wasted in this maneuver, which is not required in open surgery. Vascular anastomosis time is around 35 minutes in RAKT and 30 minutes in OKT.
In literature, grafts with more than two arteries have been implanted after ex-vivo reconstruction, 11 but we have utilized only grafts with up to two renal arteries in our initial experience.
In the postoperative period, a delayed fall in creatinine was observed in RAKT group at days 7 and 30 compared with OKT group. Serum creatinine values at 30 days in the current series were comparable with other published ones. 12,14 The difference became nonsignificant at 3 months, a finding observed by other authors too. 8,13,15 Breda and colleagues did not find any correlation between postoperative creatinine levels and total operating/rewarming time. 12
In our series, the tacrolimus level in RAKT cohort was significantly higher on POD 2. The reason could be secondary to altered bowel function secondary to the intraperitoneal nature of surgery and placing of ice slush in close contact with bowels. More data will be helpful in redefining the initial tacrolimus dosage in RAKT patients.
One patient with RAKT expired on 25th POD due to massive intracranial bleed secondary to disseminated mucormycosis. She was a known case of juvenile diabetes mellitus, on maintenance hemodialysis (MHD) for 36 months.
Rare cases of graft artery stenosis have been described in RAKT literature, but are in immediate postoperative period. 16 Our series had a single case of graft renal artery stenosis presenting at 8 months post-transplant.
Two of the obese patients having short stature and abdominal obesity with high BMI (39 and 41, respectively) planned for RAKT had to be converted to open. In both of these cases, small bowel could not be mobilized away from the pelvic cavity. Thick mesentery secondary to high fat content was suspected. Post-OKT course was uneventful and the patients were discharged with stable creatinine levels.
Three of the patients in RAKT group (BMI 42, 43, and 47) developed postoperative chest infection with sepsis and required mechanical ventilatory support along with per-enteral colistin. The patients eventually recovered, but had delayed fall in creatinine. All these three patients had graft kidney inserted via GelPOINT using periumbilical incision, which was closed using polyglactin 310 1-0 suture on sheath. Over 6 months of follow-up, two of these three patients had developed incisional hernia, which required mesh hernioplasty. We have modified our closure technique using polypropylene 1-0 suture (Ethicon, Inc.) for sheath closure in all patients with periumbilical midline incision. After that, no incisional hernia has been observed.
Obesity is a proven risk factor for surgical wound complication. Lynch and colleagues have proven the association of SSI with inferior graft outcomes in obese patients with comparable BMI. 1 At the same time, obese patients have poorer outcomes on MHD. Authors have described significantly lesser wound complications with improved graft outcomes in obese patients undergoing RAKT. 15,17 In our series, six percent of OKT patients developed wound infection (SSI), while none of RAKT patient faced SSI.
Till date, only Tugcu and colleagues have compared open and robotic renal transplant. They have compared their first 40 OKTs (historical control) with first 40 RAKTs. 18 As opposed to other publications, they did not find any difference in postoperative functional outcomes between OKT and RAKT. Postoperative pain was significantly less in the RAKT group. Even though the study has a small number and is retrospective in nature, the authors have published the first comparison between the two techniques with encouraging results of RAKT.
We believe ours is the first study comparing RAKT with OKT done during the same period with midterm follow-up. Our study is also not without limitations. Although the study is prospective in nature, randomization could not be done due to a significant difference in procedure cost to the patient. Propensity matching could not be done due to wide variation between the two patient populations. Outcomes can be affected as we have included our initial experience of RAKT. Although functional equivalence was achieved at 3 months and maintained in midterm, a longer follow-up would give more information about long-term outcomes of RAKT.
Conclusion
RAKT is coming up as a noninferior alternative to OKT in terms of functional outcomes. It is advantageous in terms of better pain scores, cosmetic outcomes, and lesser wound complication rates. Delayed normalization of serum creatinine and higher ATN remain an issue. More work is needed to maintain graft hypothermia till reperfusion starts and optimization of initial tacrolimus dosage. Studies with longer follow-up are required.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.