
Abstract
Introduction:
There are limited data regarding the effect of thulium laser (Tm:YAG) and holmium laser (Ho:YAG) on upper urinary tract. The aim of this study was to compare soft tissue effects of these two lasers at various settings, with a focus on incision depth (ID) and coagulation area (CA).
Materials and Methods:
An ex vivo experimental study was performed in a porcine model. The kidneys were dissected to expose the upper urinary tract and the block samples containing urothelium and renal parenchyma were prepared. The laser fiber, fixed on a robotic arm, perpendicular to the target tissue was used with a 100 W Ho:YAG and a 200 W Tm:YAG. Incisions were made with the laser tip in contact with the urothelium and in continuous movement at a constant speed of 2 mm/s over a length of 1.5 cm. Total energy varied from 5 to 30 W. Incision shape was classified as follows: saccular, triangular, tubular, and irregular. ID, vaporization area (VA), CA, and total laser area (TLA = VA + CA) were evaluated. Statistical analysis was performed using the SPSS V23 package, p-values <0.05 were considered statistically significant.
Results:
A total of 216 experiments were performed. Incision shapes were saccular (46%), triangular (38%), and irregular (16%) with the Ho:YAG, while they were tubular (89%) and irregular (11%) with the Tm:YAG. ID was significantly deeper with the Ho:YAG (p = 0.024), while CA and TLA were larger with the Tm:YAG (p < 0.001 and p < 0.005).
Conclusion:
ID was deeper with Ho:YAG, whereas CA and TLA were larger with the Tm:YAG. Considering surgical principles for endoscopic ablation of upper tract urothelial carcinoma, these results suggest that Tm:YAG may have a lower risk profile (less depth of incision) while also being more efficient at tissue destruction. Future in vivo studies are necessary to corroborate these findings.
Introduction
Over the several decades, various lasers have been incorporated into the armamentarium of endourology. The holmium-YAG laser (Ho:YAG) is the most widely used laser in the urologic community because of its versatility, efficiency, and coagulation characteristics being effectively used for the treatment of stones and soft tissues. 1 –4 The thulium-YAG laser (Tm:YAG) was introduced as an alternative laser for soft tissue treatment, especially for prostate surgery and bladder tumors, but there are fewer studies and less clinical experience reported with Tm:YAG compared with Ho:Yag. 5,6 Furthermore, few studies have reported the results and follow-up details of the use of Tm:YAG for treatment of upper tract urothelial carcinoma (UTUC). 7 –10
While both Ho:YAG and Tm:YAG are used in the endoscopic ablation of UTUC, there is only one study comparing the effects of these two lasers on kidney tissue. 11
The aim of this study was to compare soft tissue effects of these two lasers at various settings, with a focus on incision depth (ID) and coagulation area (CA).
Materials and Methods
An ex vivo experimental study was performed in a porcine model. Porcine kidneys were chosen because of their similar anatomy to the human kidneys. 12 Porcine kidneys were directly removed from cadavers in the slaughterhouse and they were dissected to expose the upper urinary tract (i.e., kidneys); the block samples containing urothelium and renal parenchyma were prepared as depicted in Figure 1. From each kidney, ∼12 blocks were obtained; each block was ∼2 cm in length.

Swine kidneys dissected to expose urinary system
The setup for this experiment includes a high-precision automated robotic arm that was firmly holding the firing fiber laser in contact with the specimen while moving longitudinally on a motorized rail along a straight axis at a continuous velocity of 2 mm/s, creating a fissure on the urothelium over a length of 1.5 cm (Fig. 1).
With this set up, an identical laser fiber, mounted on the automatic robotic arm, was alternately connected with a 100 W Ho:YAG (Cyber Ho, Quanta System, Italy) and a 200 W Tm:YAG (Cyber TM; Quanta System) machines. The diameter of the laser fiber used, manufactured by Quanta System, was 272 and 420 μm in core and external diameter, respectively. The incisions were made with the laser fiber tip in contact with the urothelium and with continuous highly precise movement determined by the robotic arm at a constant speed of 2 mm/s, creating a fissure on the urothelium over a length of 1.5 cm. The experiments were carried out using a broad spectrum of power settings ranging from 5 to 30 W (Table 1), and with short/medium/long pulse modalities for the Ho:YAG. Before laser activation, the block samples were submerged in 0.9% saline at room temperature. All the experiments were carried out by the same researcher (M.E.R.-S.), with the supervision and expertise of two senior researchers (S.P. and G.G.).
Experimental Settings for Both Thulium and Holmium Lasers Used in This Study
Ho:YAG = holmium laser; Tm:YAG = thulium laser.
After each experiment, samples were photographed, cataloged, labeled, and preserved in 0.4% formaldehyde. The fissures in each specimen were sliced into more than five 3-mm pieces, embedded in paraffin blocks, and stained with hematoxylin–eosin. All porcine blocks were analyzed with microscopy (Microscope ECLIPSE 50i; Nikon), in a blinded manner, by two independent pathologists.
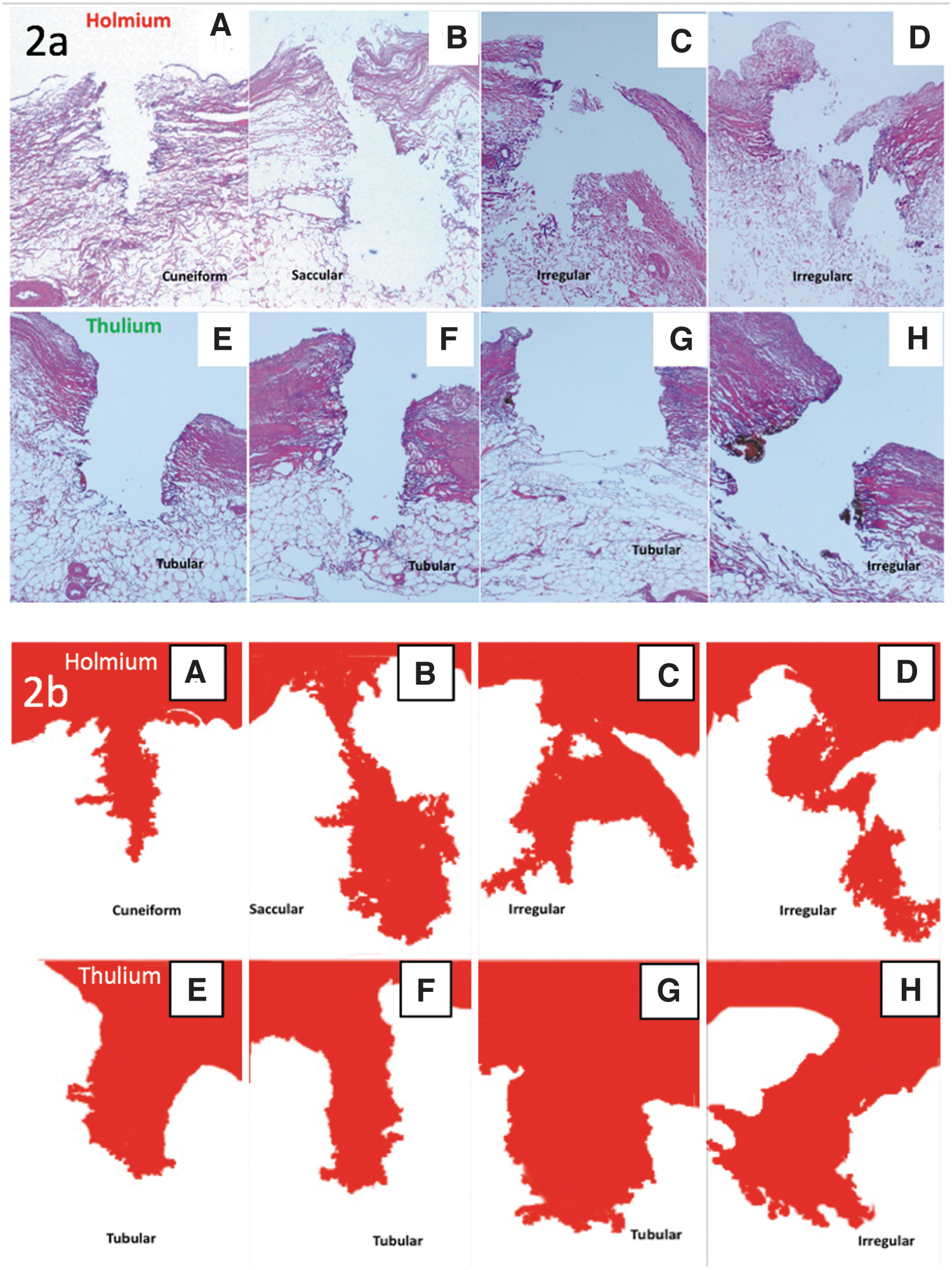
The shape of each laser incision was classified as follows: saccular, triangular, tubular, and irregular (Fig. 2). ID, vaporization area (VA), CA, and total laser area (TLA = VA + CA) were evaluated for each experimental laser incision by the pathologists (Fig. 3). Experiments and measurements were repeated three times for each emission combination. Data analysis was performed using the SPSS V23 package (IBM Corporation); χ 2 , Student t, and analysis of variance were used for statistical analysis. In addition, post hoc analysis was performed using the Bonferroni test, Welch's correction, and Games/Howell tests to evaluate variations and linear correlations between variables. Values of p < 0.05 were considered statistically significant. Tissue measurements were made by using a software specialized for microscopic image measurements (ImageJ; NIH, LOCI, University of Wisconsin).
Microscopic analysis
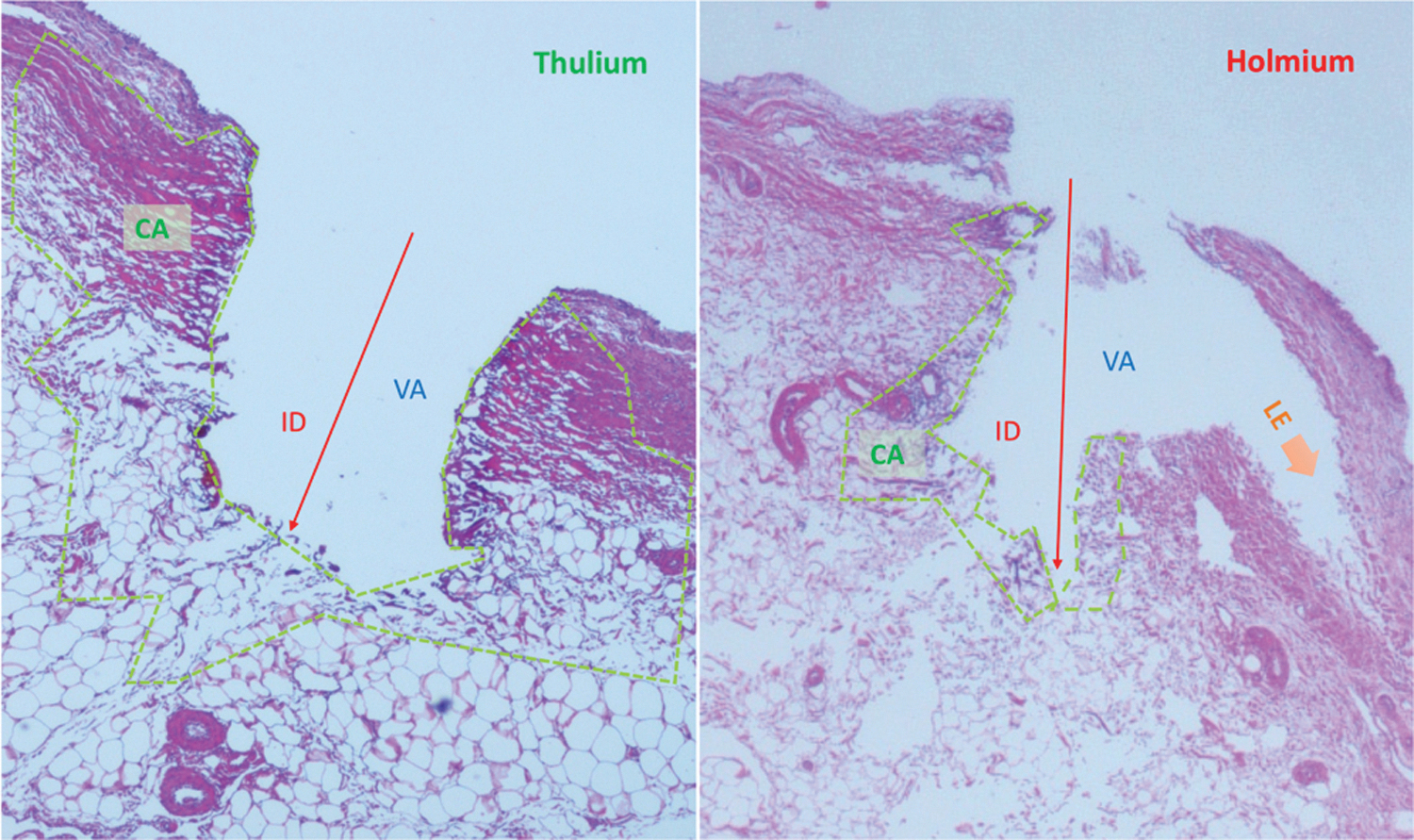
Microscopic measurements of Tm:YAG and Ho:YAG effects on soft tissue (swine kidney) with 10 W and 1 J at 10 Hz and long pulse, respectively. In the picture ID, VA, and CA are shown, used for calculation of TLA = VA + CA. Orange arrows show LE dissection with Ho:YAG. CA = coagulation area; ID = incision depth; LE = lateral energy; TLA = total laser area; VA = vaporization area; TLA = total laser area.
The ImageJ software is an open-source Java imaging processing program. Setting the scale, according to the characteristics of the microscope used, it allows the measurement of diameters, areas, and many other parameters from pictures taken from the microscope. The data are automatically stored in a database.
Results
A total of 216 experiments were performed. Incision shapes were saccular (46%), triangular (38%), and irregular (16%) with the Ho:YAG, while they were tubular (89%) and irregular (11%) with the Tm:YAG (Fig. 2).
ID was significantly deeper with the Ho:YAG (p = 0.024), while CA and TLA were larger with the Tm:YAG (p < 0.001 and p < 0.005).
In particular, factoring in all the different combinations altogether, the ID was 0.458 ± 0.194 mm with Ho:YAG and 0.346 ± 0.120 mm with Tm:YAG (p = 0.024). CA was 0.066 ± 0.035 mm2 with Ho:YAG and 0.125 ± 0.020 mm2 with Tm:YAG (p < 0.001). TLA was 0.125 ± 0.055 mm2 with Ho:YAG and 0.264 ± 0.146 mm2 with Tm:YAG (p < 0.005). Conversely, there was no difference in VA for Ho:YAG and Tm:YAG (0.066 ± 0.46 mm2 and 0.070 ± 0.45 mm2, respectively, p = 0.572) (Table 2).
Outcomes of Thulium and Holmium Lasers on Soft Tissue
p < 0.05.
CA = coagulation area; ID = incision depth; SD = standard deviation; TLA = total laser area; VA = vaporization area.
For both lasers, as power increased, significant increments were observed in the ID and TLA (p < 0.001) (Fig. 4). Whereas for CA, evidence was found for a significant increase with Ho:YAG but not Tm:YAG, where the slight increase observed was nonsignificant (Fig. 5).
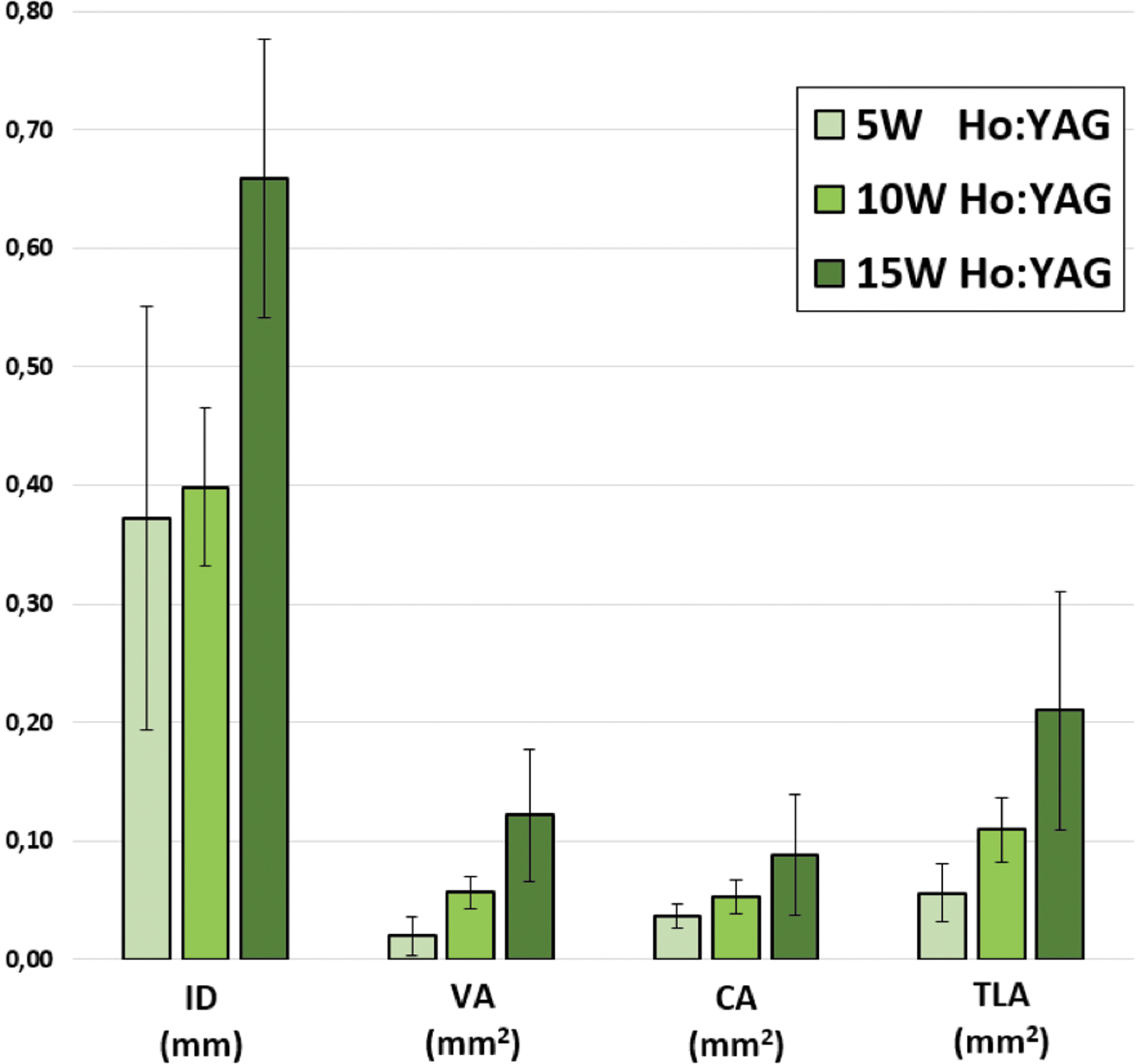
Differences among ID, VA, CA, and TLA among different power outputs with Ho:YAG. To study the overall effect resulting by a certain holmium power, different energy/frequency/duration combinations having the same overall power were grouped together.
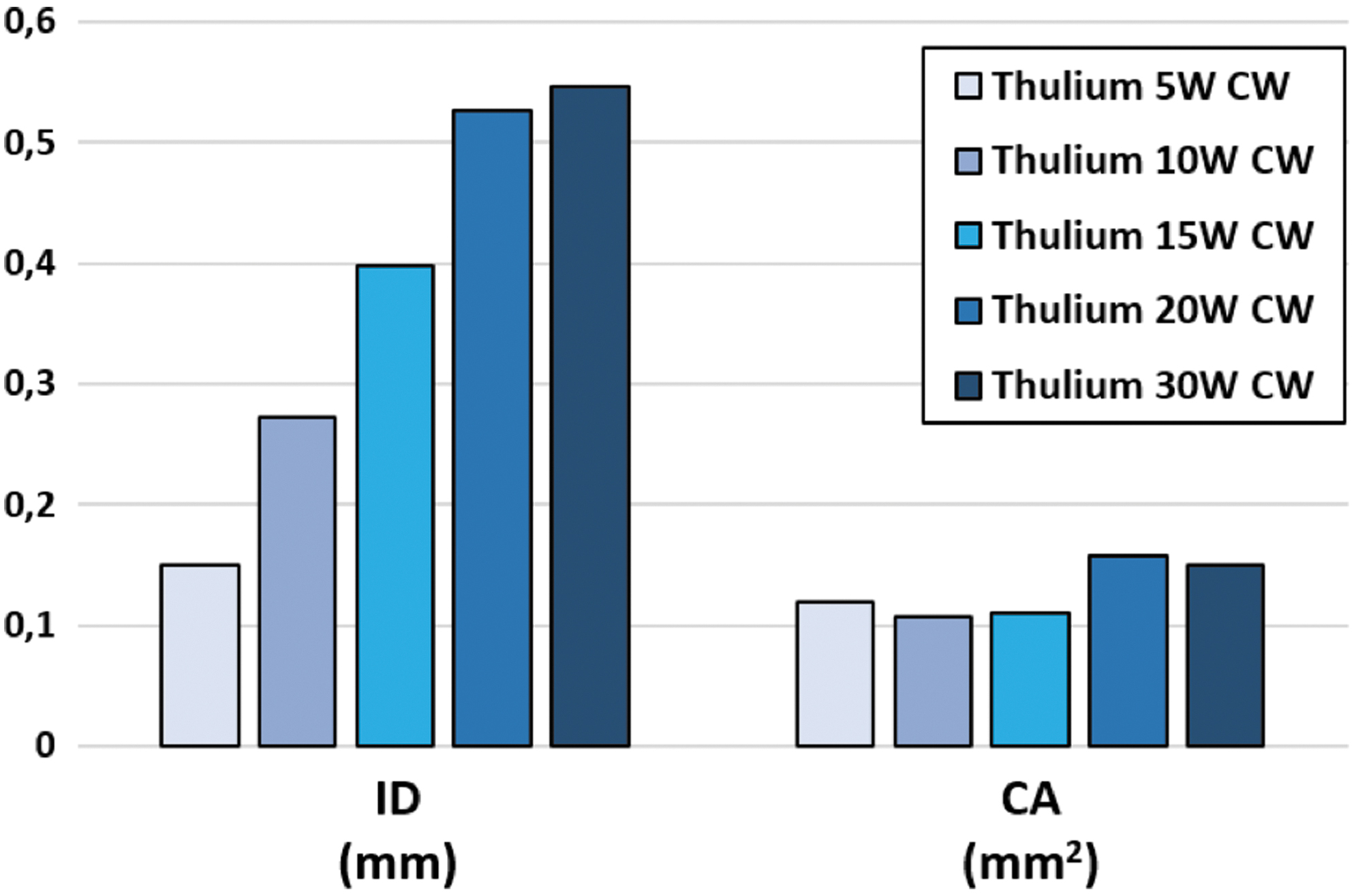
ID and CA of soft tissue treated with Tm:YAG with continuous emission within the 5–30 W power range.
The pulse length of Ho:YAG did not affect any parameter evaluated and no statistical differences were noted between short/medium/long pulse length modalities; however, CA and TLA were wider for the Tm:YAG compared with all pulse lengths of the Ho:YAG (Table 3; Fig. 6).
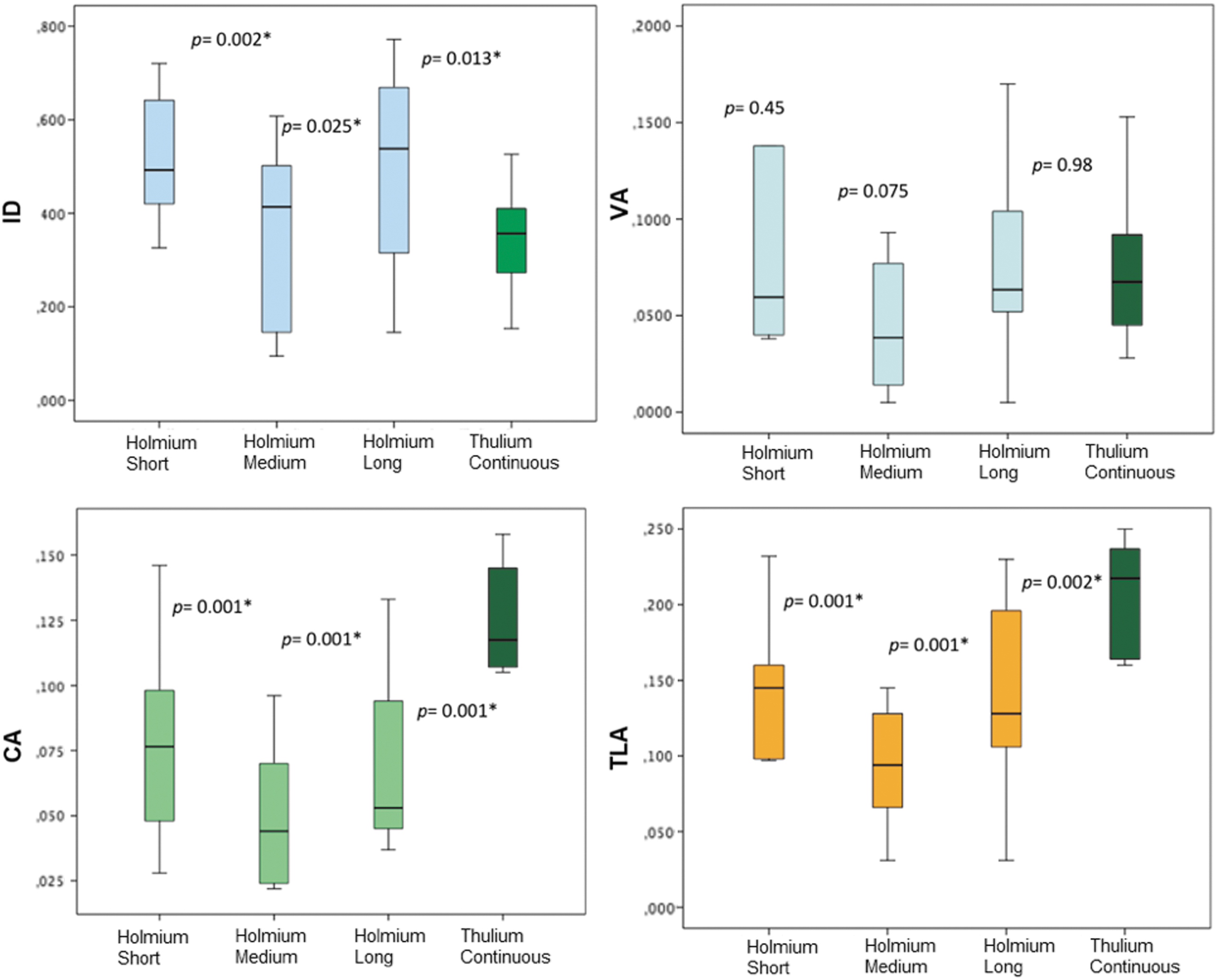
Differences among ID, VA, CA, and TLA when comparing Ho:YAG pulse modalities (short/medium/long pulse) and Tm:YAG (continuous mode). These plots visually display the outcomes reported in Table 3.
Differences Among Incision Depth, Vaporization Area, Coagulation Area, and Total Laser Area When Comparing Thulium Laser (Continuous Mode) and Holmium Laser Pulse Modalities (Short/Medium/Long Pulse)
p < 0.05.
Discussion
Both Ho:YAG and Tm:YAG have been studied for the ablation of soft tissue with urologic applications. Interactions between laser and tissue are extremely complex and depend on multiple factors, such as laser characteristics (wavelength, absorption coefficient, power, and pulse characteristics), tissue characteristics (water concentration, hardness, absorption coefficient for each tissue), environment (air, liquid), and distance and inclination angle between fiber tip and tissue. 13,14
Our results demonstrate that ID was significantly deeper with Ho:YAG (p = 0.024), while CA and TLA were larger with Tm:YAG (p < 0.01) in the upper urinary tract urothelium of a porcine model. Theoretically, this shallower incision penetration together with increased CA could represent an advantage for the use of Tm:YAG with regard to bleeding. It is known that capillaries in the ureter are just below the urothelium at the lamina propria, while the muscular layer starts about 0.1–0.2 mm from the lumen. The first vascular structures are seen at a depth of 0.4 mm and the adventitia starts 0.6–0.7 mm from the lumen containing the larger periureteral vessels. 3 The shallower penetration associated with the use of Tm:YAG may thus allow the surgeon to adequately resect tissue while at the same time avoiding the deeper vascular structures.
Surprisingly, Figure 5 shows that CA remains relatively stable as the emission power increases with the Tm:YAG. Even though the parameters analyzed are different (area vs diameter), these findings appear in accordance with the depth of penetration generally reported in literature for Tm:YAG (0.1–0.2 mm). Furthermore, these results appear in accordance with Bach and colleagues, who reported that the extent of coagulation and the necrotic tissue zone remained stable with increased power output with Tm:YAG. 15
Our findings on coagulation profile of Tm:YAG compared with those of Ho:YAG reflect the different physical characteristics of these lasers. Although Tm:YAG has similar absorption characteristics to the Ho:YAG (both wavelengths are highly absorbed by water), its continuous-wave output may be advantageous. In contrast, the pulsed emission of the Ho:YAG leads to explosive vaporization of the tissue; between laser pulses, the generated heat dissipates into the surrounding tissue producing microscopic fractures and tissue dissection irregularities. This concept is in line with the several incision shapes (irregular, triangular, saccular) noted in our study with Ho:YAG compared with the more regular incision shapes created by Tm:YAG, as shown in Figure 3. In conservative UTUC treatment, this concept could be translated into a more precise and safer coagulative profile of the Tm:YAG compared with that of the Ho:YAG.
In addition, the “anarchic” energy explosions of the Ho:YAG create agitation of the medium explaining the formation of lateral fractures observed in the tissue treated, which we called lateral energy (Fig. 2). These microexplosions obtained with Ho:YAG, characterized by detonations and other periods without energy, 1 are linked to stone retropulsion during lithotripsy, whereas in soft tissue they produce the effect of “tissue fractures” and irregularities.
Typically, the Ho:YAG pulse duration is <1 ms even for lasers with “long pulse duration” settings. The holmium laser pulse (<1 ms) is followed by a period of silence, in which the laser is not active (no emission), and the duration of this pause is 20–100 times longer in duration (depending on pulse frequency) than the actual laser emission phase. This results in Ho:YAG pulses releasing bursts of high energy in an extremely short time, generally reaching high peak power levels of 2000–10,000 W (2–10 kW). 15,16
By comparison, Tm:YAG, if used with continuous energy emission, have a peak power value equal to the average power (max. 200 W in surgical Tm:YAG currently available in the market) but without interruptions of emission. The application of low peak power and continuous emission create different thermal and ablative effects (i.e., there is no cooling period allowed in the pauses in between, as happens between the Ho:YAG pulses). We hypothesize that these characteristics of the Tm:YAG are responsible for the findings in our study: Tm:YAG, compared with Ho:YAG, results in more regular tissue edges and greater hemostatic properties. This low peak power is also the reason that Tm:YAG is extremely inefficient for lithotripsy of stones and why it is not used for that treatment.
In literature, there are few ex vivo experimental studies on this topic. Huusmann and colleagues analyzed different parameters in ambient air and in saline, comparing Ho:YAG and Tm:YAG; in the saline experiments, the laser damage zone was 0.550 ± 0.137 mm (Tm:YAG) vs 0.447 ± 0.065 mm (Ho:YAG) on the low-power settings and 0.653 ± 0.137 mm (Tm:YAG) vs 0.677 ± 0.134 mm (Ho:YAG) on the high-power settings (80–120 W output). The ID was 1.214 ± 0.888 mm for Ho:YAG, whereas Tm:YAG did not cut tissue at 5 W in saline. On the high-power setting, the ID was 4.050 ± 1.058 mm (Tm:YAG) vs 4.083 ± 0.520 mm (Ho:YAG). 11
In contrast to the work by Huusmann and colleagues, 11 our ID with both lasers was more superficial. These differences may be attributable to the fact that in that study, both lasers were activated on the renal cortex and not on the upper urinary tract urothelium as in ours, and more importantly, with a broader and significantly higher overall power spectrum (5–120 W vs 5–30 W).
For UTUC treatment, setting combinations have been reported within ranges of 5–10 W and 10–20 W for Ho:YAG and Tm:YAG, respectively. 6,17 –19 According to these studies, we decided to analyze a spectrum of relatively low-power settings (5–30 W) by using small laser fibers (272 μm), as in common clinical practice for endoscopic treatment of UTUC.
Emiliani and associates showed in a bovine model that higher power used with Ho:YAG was associated with increased depth and width of the incision (p < 0.01 and p < 0.008, respectively). 3 The experiments were performed only in the bovine renal cortex and with a broad overall power spectrum (2.5–80 W); again, these methodologic differences explain the differences in the results of the two studies. As a matter of fact, in our study the mean ID of Ho:YAG was 0.458 ± 0.194 mm compared with the overall mean of 2 mm (0.25–4.39 mm range) ID reported by Emiliani and colleagues. 3 Our findings are more consistent with the study of Johnson and et al., 20 who showed a mean ID of 0.4 mm (0.1–0.65 mm).
One of the unique aspects of our study is how we measured the effects of the two lasers on the urothelium. In previously mentioned studies, CA was measured in diameter, whereas we evaluated VA, CA, and TLA by using specific software for microscopic image measurements. We feel that for better understanding of the effective coagulation properties of one laser compared with another, it might be more appropriate to express this concept with area measurement (mm2) instead of with diameter (mm), especially considering that the incision shapes are often not regular or circular.
Using an ex vivo porcine model, Becker and colleagues 21 analyzed the different effects between continuous and superpulsed thulium fiber laser (TFL) on soft tissue, evaluating the diameter of both coagulation and carbonization zones. Their study demonstrated less carbonization area with superpulsed TFL rather than with continuous TFL. 21 Therefore, TFL appears promising not only for stones but also for soft tissue. 21,22 Further studies are, however, needed to investigate the differences between TFL and Tm:YAG on soft tissue and in particular on the upper urinary tract urothelium.
Surprisingly, in our study, the analysis of the results failed to demonstrate differences among different pulse lengths of the Ho:YAG (short/medium/long pulse) in terms of coagulation profiles. These findings are similar to those observed in the study of Emiliani and colleagues, where they reported that varying pulse lengths did not affect the outer mean coagulation depth or ID, although the mean width with the short pulse was greater than with the long pulse (p = 0.04). 3 Conversely, the VA related to the short pulse (high peak power) was fourfold greater than the VA for medium and long pulse. The high peak power of Ho:YAG may create greater tissue trauma and we plan to investigate this hypothesis in future studies.
The continuous mode of the Tm:YAG allows excellent hemostasis and may provide operative advantages over the Ho:YAG for the indications described in this article. The ubiquity of target chromophore (water molecules) provides constant conditions for the laser tissue heated by the laser beam up to the boiling point; the tissue left behind after each laser pass is covered by a coagulated seam of tissue, which provides hemostasis. 23 These characteristics of the Tm:YAG may result in less bleeding and better visibility when used for the treatment of UTUC, which, in turn, could lead to a more efficient, faster, and safer tumor ablation. This hypothesis should be confirmed in further ex vivo and in vivo studies. To our knowledge, the current study provides the first experimental data comparing the coagulation effects of Tm:YAG and Ho:YAG on the urothelium of upper urinary tract in a porcine model, by using small laser fibers and low-power settings as needed in the UTUC endoscopic treatment.
As with any ex vivo study, this study is not without limitations. One limitation of this study may be that the experiments were not performed in live animals, and thus, the kidneys studied were not perfused as they would be in an in vivo model. 24,25
Nevertheless, Khoder et al. demonstrated that the laser damage zones are similar in perfused and nonperfused porcine kidneys. 26 The in vivo kidney perfusion might have a different effect on heat absorption and therefore may vary the results. Another limitation is that fibers >500 μm were not used; however, we chose a small fiber size to simulate the conditions in real-world flexible ureteroscopy—modern ureteroscopes can accommodate laser fibers up to 365 μm in core diameter but not the larger fiber sizes.
A final limitation of this study is that any comparison of a pulsed laser with continuous wave may be challenging due to fundamental differences in laser beam–tissue interaction by the properties of heat conduction and heat excess-thermal relaxation time.
Conclusion
This ex vivo study shows several potential advantages of the Tm:YAG over the Ho:YAG for the treatment of UTUC, namely the following: shallower ID, greater CA, and greater TLA. Considering the surgical principles for endoscopic ablation of UTUC, these results suggest that Tm:YAG may have a lower risk profile (less depth of incision) while also being more efficient at tissue destruction. Further in vivo studies are needed to confirm these findings.
Footnotes
Author Disclosure Statement
G.G.: consultant for Coloplast, Rocamed, Olympus, Boston Scientific, BD-Bard, Cook Medical, Quanta System. S.P.: consultant for Quanta System. B.H.E.: Consultant for Boston Scientific, Olympus, Kalera Medical, SonoMotion. M.E.R.-S. was supported by the EUSP scholarship from the European Association of Urology. The other authors have no conflicts of interest to declare.
Funding Information
No funding was received for this article.