
Abstract
Purpose:
To assess the efficacy of dual-energy CT (DECT) in predicting the composition of urinary stones with a single index (dual energy ratio [DER]) and five indices.
Methods:
Patients undergoing DECT before active urolithiasis treatment were prospectively enrolled in the study. Predictions of stone composition were made based on discriminant analysis with a single index (DER) and five indices (stone density at 80 and 135 kV, Zeff [the effective atomic number of the absorbent material] of the stone, DER, dual-energy index [DEI] and dual-energy difference [DED]). After extraction, stone composition was evaluated by means of physicochemical analyses (X-ray phase analysis, electron microscopy, wet chemistry techniques, and infrared spectroscopy).
Results
: A total of 91 patients were included. For calcium oxalate monohydrate (COM) stones, the sensitivity, specificity, and overall accuracy of DECT with one index (DER) were 83.3%, 89.8%, and 86.8%, respectively; for calcium oxalate dihydrate (COD) and calcium phosphate stones—88.2%, 92.9%, and 91.2%, respectively; for uric acid stones—0%, 98.8% and 97.8%, respectively; for struvite stones—60%, 95.3%, and 93.4%, respectively. Discriminant analysis with five indices yielded the following sensitivity, specificity, and overall accuracy: 95.2%, 89.8%, and 92.3% for COM stones, 85.3%, 96.4%, and 92.3% for COD stones, and 100% in all three categories for both uric acid and struvite stones.
Conclusions:
DECT is a promising tool for stone composition assessment. It allowed for evaluation of chemical composition of all stone types with specificity and accuracy ranging from 85% to 100%. Five DECT indices have shown much better diagnostic accuracy compared to a single DECT index.
Introduction
Urolithiasis remains one of the most prevalent urologic diseases worldwide. Its prevalence varies between 1% and 20% depending on the country or population. 1 Overall, 25% of patients with urolithiasis require surgical intervention and almost 50% will have a recurrence. Currently, strategies for management of urolithiasis include observation, medical expulsive therapy, chemolysis, and surgical intervention (e.g., extracorporeal shock wave lithotripsy [SWL], percutaneous nephrolithotomy [PCNL], and ureteroscopy). However, specific stone formation patterns necessitate shaping the treatment strategy individually. 2 For example, an understanding of the respective stone composition is particularly helpful when identifying good candidates for SWL therapy. For calcium oxalate monohydrate (COM) or cystine stones, SWL is less effective due to their Young's modulus, fracture toughness as well as wave speed, so endourologic approaches may be the treatment of choice. 3,4 Therefore, diagnostic techniques that can reliably predict stone composition before surgical intervention are among the most sought-after.
Dual-energy CT (DECT), a novel form of CT technology, is being actively introduced into modern urologic practice. DECT operates by using different sources capable of generating radiation at various energy levels. Detectors can distinguish between them and estimate not only stone density but also its composition (based on the energy of the absorbed photon beam). This technique was first described in the 1970s but was only implemented into clinical practice in 2006, as technological advances were made in the field of CT imaging. 5 –10 Recent research studies have shown that DECT with one index can detect and differentiate between uric acid and calcium-containing stones. 11 However, we hypothesize that more DECT indices may provide a higher resolution image thus making detection easier for not only COM and uric acid stones but also other stone types. The aim of this study was to assess the efficacy of DECT in predicting the composition of urinary stones with only one index and five indices.
Materials and Methods
This single-center study was approved by the local Institutional Review Board. After approval, we started enrollment of patients with urolithiasis who were candidates for active treatment (SWL, PCNL, or ureteroscopy). Patients with stones <5 mm in diameter on CT were excluded. For CT and DECT imaging, we used an Aquilion One 640 system, a single-source dual-energy scanner with fast kilovoltage switching (Canon, Japan). All examinations were performed by a single radiologist (L.K.) in volumetric mode with the following settings: tube voltage of 120 kV for CT and 80/135 kV for DECT, tube current of 50/290 mA, slice thickness of 0.5 mm, field of view of ≤16 × 16 cm, and exposure time of 15 seconds. For DECT image analysis, we used the DE Stone Analysis software (Canon, Japan), which allowed for stone density mapping (Figs. 1 and 2). The analysis was performed by the same radiologist (L.K.). Only the preinstalled software was used. Conventional CT was used for anatomy assessment and precise stone location (for further surgery planning), whereas DECT was used for stone composition analysis. We had informed the patients on the possible adverse effects of two consecutive scans, and only after the written consent had been obtained, the patients were included into the study.

Dual-energy CT. Calcium oxalate monohydrate stone mapping (blue). A stone measuring 2.25 × 0.96 × 2.36 cm with density of 1796.5 HU at 80 kV, 1297.9 HU at 135 kV, and 1102 HU at 120 kV is located in the upper calyx of the left kidney. DER = 1.384, DEI = 0.097, and DED = 498.6. Calcium oxalates are marked with blue, uric acid stones are marked with red; mixed stones are marked with blue, cyan, violet, and red. DED = dual-energy difference; DEI = dual-energy index; DER = dual-energy ratio; HU = Hounsfield unit.
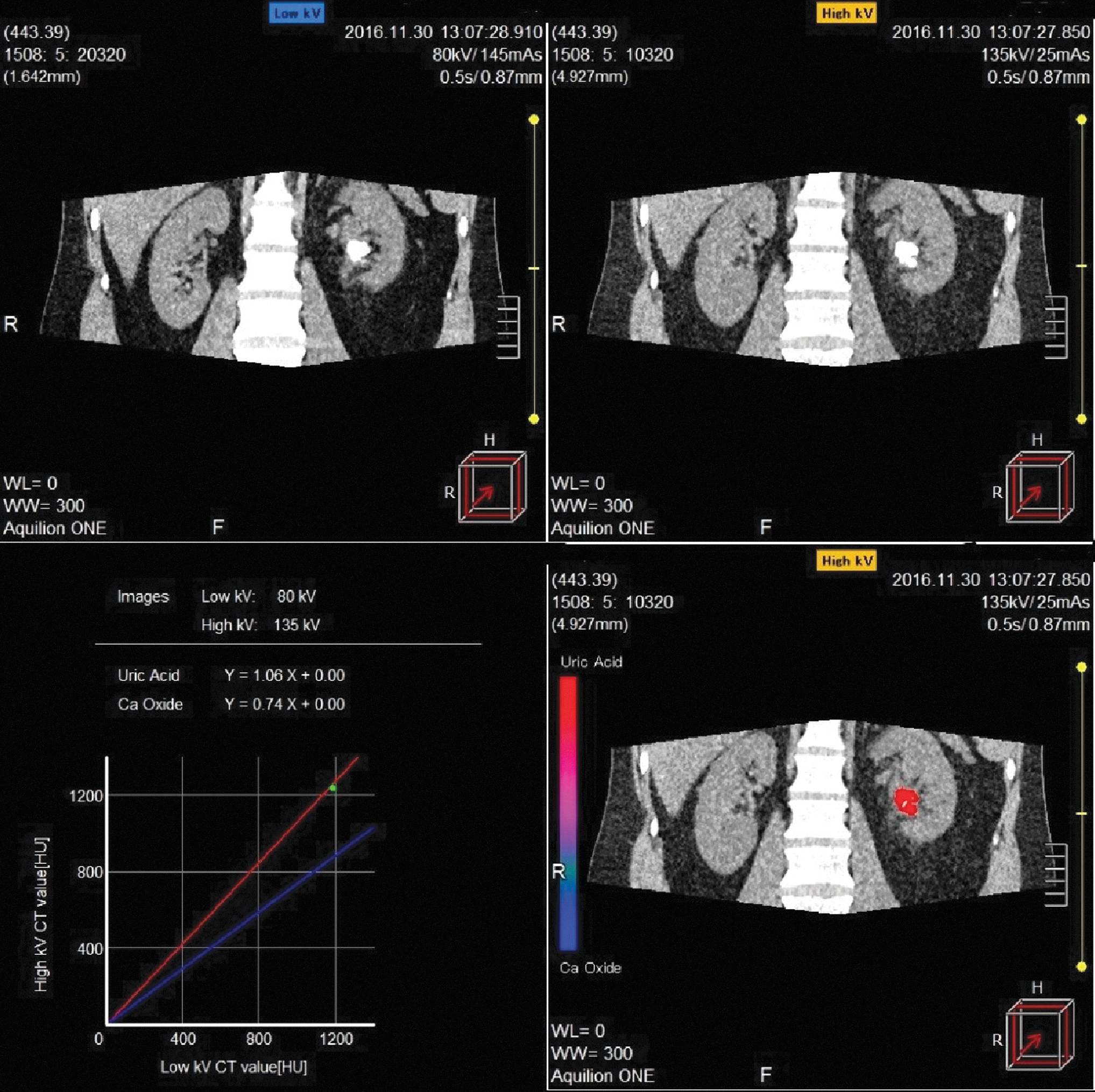
Dual-energy CT. Uric acid stone mapping (red). A stone measuring 2.4 × 1.8 × 1.3 cm with density of 454.4 HU at 80 kV, 432.4 HU at 135 kV, and 438.5 HU at 120 kV is located in the pelvis of the left kidney. DER = 1.051, DEI = 0.0076, and DED = 22.1. Calcium oxalates are marked with blue, uric acid stones are marked with red; mixed stones are marked with blue, cyan, violet, and red.
Both conventional CT and DECT were performed in the same session. DECT protocol: DECT stone composition was assessed by means of discriminant analysis with the following five indices: (1) dual-energy index (DEI) = (X low kV – X high kV)/(X low kV + X high kV +2000), where “X low kV” is stone density in Hounsfield unit (HU) at low energy level and “X high kV” is density at high energy level 12 ; (2) dual-energy ratio (DER) = (stone density in the low-energy image/density in the high-energy image) 13 ; (3) dual-energy difference (DED) = (stone density in the low-energy image – stone density in the high-energy image) 14 ; (4) Zeff, the effective atomic number of the absorbent material; and (5) stone density at 80 and 135 kV. For stones <2 cm, we performed a single density measurement in an area 1–5 mm in diameter that covered at least half of the region of interest of the stone. For stones >2 cm (including staghorn calculi), we performed multiple measurements to calculate average density. Conventional CT was used to assess stone location, size, volume, density at 120 kV, and zonal structure as well as the anatomy of the urinary tract.
Stone composition analysis
To asses the accuracy of DECT in prediction of stone composition, we collected stone fragments after surgical intervention (PCNL, retrograde intrarenal surgery or SWL). The fragments were sent for physicochemical analyses, which involved infrared spectroscopy, wet chemistry techniques, X-ray crystallography, and electron microscopy. Components composing at least 75% of the stone volume were considered prevailing (COM, calcium oxalate dihydrate [COD], uric acid, struvite), and mixed stones were excluded.
Statistical analysis
For statistical analysis, the SPSS Statistics 22.0 software (IBM, Armonk, USA) was used. The distribution of quantitative variable values in the groups was assessed with Shapiro–Wilk and Kolmogorov–Smirnov tests. Significant differences in measurements were checked by dispersion analysis for multiple comparisons and by t-criterion for independent samples for paired comparisons. For intergroup comparisons of quantitative variables (without normal distribution), the nonparametric Kruskal–Wallis test for multiple comparisons and the Mann–Whitney test for paired comparisons were used. Significant differences between categorical and ordinal parameters in multiple and paired comparisons were estimated using the Pearson's chi-square test with Yates' continuity correction. Cells with an expected value ≤5 were examined with the exact Fisher's test for 2 × 2 tables. A p-value of 0.05 was chosen as the threshold for statistical significance. Sensitivity, specificity, and overall accuracy were calculated using standard formulae.
To assess the homogeneity of covariance matrices for compared groups, a multivariate Box's M test was used. The connection between the discriminant function and the study groups was examined by canonical correlation coefficients ranging from 0 to 1. Discriminant functions were assessed using the Wilks' lambda test. For each discriminant function, the role of its components was estimated by comparing total variance and covariance matrices using the F-test.
Results
The study was conducted after Sechenov University Institutional Review Board approval (DECT-1, October 2016). Initially, 125 patients were enrolled. Of them, 28 were later excluded due to mixed composition of the stones and 6—due to failure to obtain stones for analysis. The study included a total of 91 patients with mean age of 42.7 years (range, 20–70 years); of these, 68 were males (74.7%) and 23 were females (25.3%). Mean body mass index was 27 kg/m2 (range, 19–30 kg/m2). Standard X-ray exposure of 4.5–5.0 mSv was used for both conventional CT and DECT. Mean stone size was 19.3 mm in the greatest diameter (range, 5.2–62.3 mm). Twenty-four patients (26.4%) had a distal ureteral stone, 22 patients (24.2%) had a kidney stone, and 17 patients (18.7%) had stones in the ureteropelvic junction. In addition, staghorn calculi were detected in 6 patients (6.6%) and multiple stones in renal calices were detected in 10 patients (11%). Each stone was assessed separately. The surgical interventions included SWL in 53 (58.2%) patients, PCNL in 20 (22.1%) patients, and ureteroscopy in 18 (19.7%) patients. A strainer was provided after SWL to catch stone fragments in urine. The strainer was used until no fragments were found for several days.
Data comparison between DECT and physicochemical analyses revealed that DECT correctly classified almost all the stones (Tables 1 and 2). DECT with a single parameter (DER) (Table 3) showed the following sensitivity, specificity, and overall accuracy, respectively: 83.3%, 89.8%, and 86.8% for COM stones (whewellite): 88.2%, 92.9%, and 91.2% for COD stones (weddellite and brushite); 90%, 98.8%, and 97.8% for uric acid stones; and 60%, 95.3%, and 93.4% for struvite stones (Table 4). No cystine stones were found. The calculated asymptotic p-value of 0.376 (two-sided) indicated no significant differences in stone composition assessment between DECT and physicochemical tests).
Preoperative Prediction of the Chemical Composition of the Stones According to Dual-Energy CT Data Based on Dual-Energy Ratio Threshold Values and Actual Stone Composition as Determined with Wet Chemistry Techniques
COD = calcium oxalate dehydrate; COM = calcium oxalate monohydrate; DECT = dual-energy CT.
Correct and Incorrect Predictions Stone Composition by Dual-Energy CT Based on Dual-Energy Ratio Threshold Values and Five Indices in Comparison with the Results of Physicochemical Analyses
Dual-Energy Ratio Threshold Values for Classification of Stones on Dual-Energy CT
DER = dual-energy ratio.
Diagnostic Value of Dual-Energy CT in Assessing the Composition of Urinary Stones Based on a Single Dual-Energy Ratio Index and Five Indices
DECT analysis with five indices showed better sensitivity, specificity, and overall accuracy than DECT analysis with a single index (Tables 2 and 4). The sensitivity, specificity, and overall accuracy for DECT analysis with five indices were 95.2%, 89.8%, and 92.3% for COM stones; 85.3%, 96.4%, and 92.3% for COD stones; and 100% in all three categories for uric acid and struvite stones (Table 4). The average densities (HU) at 80, 135, and 120 kV for COM stones were 1476.2, 1079.1, and 1188.1, respectively, and for COD stones—1585.8, 1068.4, and 1199.2, respectively.
Discussion
The current study is one of the first to prove the value and efficacy of five-index DECT imaging in urolithiasis. While a number of previous works were able to show that DECT could be effective in stone type assessment, 15 this study demonstrated that five indices improved DECT accuracy in stone composition evaluation (compared to a single DER index). This data give credence to the notion that detection of uric acid calculi on diagnostic imaging may warrant a beneficial shift from surgical intervention to chemolysis as a primary treatment modality. 1 Previously, chemolysis as initial therapy was shown to dissolve 70%–80% of stones. 16 However, accurate detection of struvite stones with DECT may also encourage urologists to pursue a treatment course that involves complete surgical stone removal. Body mass index may possibly affect the quality of images and thus the accuracy of the described method. In this study, there were no patients weighing over 100 kg, so we were not able to test this hypothesis.
The number of articles which explore the utility of DECT in treatment planning for urolithiasis is increasing. Ferrero and colleagues 17 and Largo and colleagues 18 demonstrated that data obtained from DECT imaging protocol (DER and DEI) combined with information on the stone volume, flatness of the surface, and density of the stone were the main prognostic signs used to determine whether SWL would benefit a patient. 17,18 CT attenuation/DEI of stones calculated from DECT acquisitions was a significant independent predictor (p < 0.01) for the number of required shock waves. 18 Habashy and coworkers also examined the impact of DECT as a conservative therapy that would guide the management of urinary calculi. 19 In this study, the authors highlighted that identification of uric acid stone composition by DECT altered the treatment of 15/303 (5.0%) patients and thus was effective in allowing 12 patients to avoid surgery.
A comprehensive analysis with five DECT indices yielded high sensitivity, specificity, and overall accuracy (reaching 100%) for uric acid and struvite stones. However, such values could stem from small group size. Similar findings were obtained by Akand and colleagues with perfect sensitivity results. 20 McGrath and coworkers in their systematic review and meta-analysis summarized the available data and found that DECT could be an accurate replacement test for diagnosis of uric acid calculi in vivo with mean sensitivity of 82% (95% confidence interval [CI] 0.73–0.89) and mean specificity of 97% (95% CI 0.94–0.98). 15
Most previous studies that examined the ability of DECT to assess the composition of urinary calculi only explored one or two DECT indices (predominantly DER and Zeff). 21 –23 Kulkarni and associates showed that a Zeff range of 6.2–7.8 is typical for uric acid stones, 11.2–14.4 for COM stones, 9.2–10.0 for struvite stones, and 10.2–11.8 for cystine stones. 21 Matlaga and colleagues, 14 Hidas and associates, 22 and Thomas and coworkers 23 mentioned that the DER for uric acid stones was 1.04–1.09, <1.1, and 0.88–1.18, respectively. Our findings are similar to these results (Table 3).
Acharya and colleagues showed that a cutoff DER of 1.385 to detect calcium-containing stones had sensitivity of 65.6% and specificity of 82% and that DER values <1.335 for calcium-containing stones were only typical for COM stones. 24 Our study yielded similar findings (Table 3).
Single-index DECT proved less efficient than five-index DECT (Table 4), which includes stone density at 80 and 135 kV, Zeff of the stone, DER, DEI, and DED. Five-index DECT may substantially improve diagnostic efficiency, sensitivity, specificity, and overall accuracy. For example, sensitivity of DECT for COM stones was only 83.3% if only one index (DER) was used and 95.2% if five indices were used (Table 4).
Another important issue is correlation between DECT data and the results of physicochemical analyses. In a recent meta-analysis, Zheng and colleagues mentioned that DECT is only able to effectively detect uric acid stones. Several authors also reported that DECT has good diagnostic accuracy and 100% accuracy in differentiating between uric acid and nonuric acid stones. 23,25 Our findings support the fact that DECT can also effectively individually differentiate between COM, COD, and struvite stones with high specificity and sensitivity.
Similarly to Acharya and associates, we demonstrated the capabilities of DECT for more accurate characterization of calcium-containing stones and for detecting stones which are more resistant to fragmentation during SWL, such as COM. 24 Thomas and colleagues classified a mixed-composition stone containing calcium oxalate and struvite as a uric acid stone since the DER of struvite closely matched that of uric acid. 23 We obtained similar findings for struvite stones when only a single DER index was used: specificity of 60% and sensitivity of 95.3%. However, when five DECT indices were analyzed, the specificity and sensitivity significantly improved.
Another factor worth considering is body mass index. Weight over 100 kg was previously considered to be a limiting factor for DECT analysis. However, Kordbacheh and associates were able to show that DECT is effective in patients up to 163 kg. 26 In their study of 197 patients, DECT was able to predict stone composition in 95.6% of patients. In our work, we were unable to asses DECT applicability in overweight patients due to their absence in the initial cohort. This aspect requires further research.
This was a preliminary research study that aimed to investigate the abilities of DECT in characterizing composition of various urinary calculi. Among the study limitations are small cohort and absence of cystine stones due to the preliminary nature of this study. In addition, we did not examine mixed-composition stones. It is also important to stress that being a preliminary study, it only compared five-index to single-index DECT, without the estimation of each index or their combinations separately. Standard physicochemical analyses of stones may fail to correctly identify several stone types; therefore, we carried out additional tests (electron microcopy and spectroscopy). It should also be mentioned that five-index DECT requires a skilled radiologist and may be twice as time-consuming. Another limitation is the absence of overweight patients in the study. DECT efficacy should be investigated for this specific cohort of patients. Further studies regarding the clinical efficacy of DECT with larger cohort are required.
Conclusion
DECT is a promising tool for stone composition assessment. It was able to predict chemical composition of all stone types with specificity and accuracy ranging from 85% to 100%. Five DECT indices showed much better diagnostic accuracy compared to a single DECT index.
Ethical Approval
The study was approved by the Sechenov University (Moscow, Russia) Institutional Review Board.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.