
Abstract
Purpose:
Metabolic syndrome (MetS) is a cluster of metabolic diseases that is linked to atherosclerotic cardiovascular disease. MetS has also been linked to increased nephrolithiasis. However, limited research has been conducted on MetS and its impact on stone-specific health-related quality of life (HRQOL). This study aims to examine the hypothesis that the presence of MetS is associated with decreased HRQOL.
Materials and Methods:
The Wisconsin Stone Quality of Life Questionnaire, a stone-specific HRQOL questionnaire, was used to survey 3051 patients with kidney stones. Medical history was collected from patients. These data were used to distinguish MetS patients from non-MetS patients. Among patients with current stones, a Wilcoxon rank sum test was used to compare HRQOL scores from MetS patients and non-MetS patients. HRQOL from patients with and without individual MetS components were also compared, and a multivariate analysis was conducted.
Results:
Statistical comparison between MetS patients (median score 102/140) and non-MetS patients (median score 106/140) demonstrated a lower stone-specific HRQOL in patients with MetS (p = 0.049). Among individual MetS components, patients with diabetes mellitus (DM) or body mass index (BMI) >30 had significantly lower HRQOL than patients without DM or BMI <30 (p = 0.028 and p < 0.001, respectively). The multivariate analysis supported this trend as MetS remained a significant predictor of decreased HRQOL (p = 0.002) after controlling for other variables assessed.
Conclusions:
This study indicates an association between MetS and a lower stone-specific QOL. This has important implications for stone prevention strategies in patients with MetS.
Clinical Trial Registration number: H14-01143
Introduction
Metabolic syndrome (MetS) is a constellation of metabolic comorbidities that has come under scrutiny by the medical community in recent years. It is a common cluster of conditions, affecting >40% of the population in the United States. 1 Obesity-induced insulin resistance is often a precursor to MetS, as it leads to hyperglycemia and hyperinsulinemia and culminates in the development of diabetes. 2 Primarily, MetS has been thought to directly initiate the onset of atherosclerotic cardiovascular disease. 3
Recently, MetS has also been associated with an increased risk of nephrolithiasis. 4 History of kidney stones is twice as likely to be observed in individuals with three criteria of MetS and three times as likely to be observed in individuals with all five MetS criteria. This result corroborates previous findings by Kohjimoto et al., where MetS was shown to increase the severity of kidney stone formation. 2 These results have led to suggestions that managing a patient's MetS may be an advisable course of action in kidney stone care. Although rate of recurrence is a significant aspect of nephrolithiasis, another central idea when treating kidney stones is patient quality of life (QOL). Health-related QOL (HRQOL) refers to patients' perceived impact of a given disease on their physical, social, and emotional well-being. 5
Often, asymptomatic stones may be left untreated under observation to avoid invasive procedures. Conversely, highly symptomatic stones have high priority for treatment because of their large impact on a patient's HRQOL. As such, factors that can affect kidney stone patient HRQOL should be identified to eliminate a potential aggravator of stone symptoms. We hypothesize that MetS is indeed such an aggravator and is thus associated with a decreased stone-specific HRQOL.
Materials and Methods
Study background
This is a multisite prospective observational study under the North American Stone Quality of Life Research Consortium. Institutional Review Board Ethics approval was obtained at all sites and the principal data coordination site was the University of Wisconsin-Madison (IRB Number H14-01143).
All sites used the Wisconsin Stone QOL (WISQOL) for data collection. The WISQOL is used to measure stone-specific HRQOL. This is important as the mere presence of MetS is known to impair HRQOL 6 —a questionnaire that only evaluates stone-specific HRQOL necessary to filter out differences in HRQOL that originate from MetS status alone. It was first presented in 2013 by Penniston and Nakada 7 and later validated in 2017 in a diverse population across eight North American sites. 8 The WISQOL questionnaire comprises 28 questions divided into four subdomains: section 1—social, section 2—emotional, section 3—stone-related symptom impact, and section 4—vitality.
Data collection
At each site, participants with kidney stones were approached in outpatient clinics to fill out the WISQOL. In addition to the 28 WISQOL items, patients were also asked to respond to questions asking if they currently had stone(s) and whether they were at that time experiencing stone-related symptoms. Eligibility criteria included a history of kidney stones, being 18 years of age or older, and the ability to read English. Patients were recruited between November 2014 and May 2019. The principal investigator at each site was an urologist, providing medical and surgical stone management.
Consent was obtained for each participant by a member of the study team at each site. The WISQOL was administered to each participant. Demographic information was collected along with medical and surgical data. Secure methods, approved by the institutional review boards, were used for data storage and transmission.
MetS diagnosis
Confronted with multiple differing criteria for MetS (Table 1), guidelines were adopted that most closely aligned with the medical history data points that had been collected from participants. The National Cholesterol Education Program—Adult Treatment Panel III (NCEP-ATP III) criteria were chosen because it reflected the diagnosis conditions for hyperlipidemia (HLD), hypertension (HTN), and diabetes mellitus (DM). NCEP-ATP III criteria for MetS is three of the following five conditions: triglyceride levels ≥1.69 mM, high-density lipoprotein-cholesterol (HDL-C) <1.03 mM in men or <1.29 mM in women, blood pressure ≥130/85 mm Hg, blood glucose levels ≥5.6 mM, and a waist circumference ≥102 cm in men and 88 cm in women. 9
Metabolic Syndrome Criteria
BMI = body mass index; EGIR = European Group for the Study of Insulin Resistance; HDL-C = high-density lipoprotein-cholesterol; HTN, hypertension; IFG = impaired fasting glucose; IGT = impaired glucose tolerance; NCEP-ATP III = National Cholesterol Education Program—Adult Treatment Panel III; T2D = type 2 diabetes; TG = triglycerides; WC = waist circumference; WHO = World Health Organization; WRH = waist-to-hip ratio.
HLD was diagnosed when triglyceride levels ≥1.69 mM and/or HDL levels were <1.03 mM. 10 Because a HLD diagnosis combines two of the five criteria into one category, it was considered fulfillment of only one criterion to avoid any misdiagnosis of MetS in participants. HTN was diagnosed when blood pressure was ≥130/85 mm Hg, 11 which was identical to the MetS criteria. DM was diagnosed with a fasting glucose of 7.0 mM. 12 This incorporates the MetS criteria of hyperglycemia at 5.6 mM. This study deviated from NCEP-ATP III criteria by replacing waist circumference with the criterion for body mass index (BMI) used in the World Health Organization (WHO) MetS definition. Based on WHO criteria, the BMI cutoff of >30 kg/m2 was used.
MetS diagnosis was determined from health record information. Binary data indicating whether participants had HLD, HTN, or DM were collected. A numerical BMI was recorded for study participants. Patients who met three of the four collected conditions were considered by this study to have MetS.
Statistical analysis
Any blank responses left by participants in the questionnaire were addressed by using the average of all answers for that question (from all 3051 participants). The data from all sites were compiled and filtered to only include the questionnaires completed at a time when the patient had kidney stones (population: active stone formers). A patient's status of an active stone former is verified through radiologic imaging. These active stone formers also self-reported that they were experiencing stone symptoms. Of the patients selected, the recorded medical data were surveyed to identify those who had MetS. Patients without MetS functioned as the control group.
The R Studio Statistical Analysis Suite was used to conduct a Wilcoxon rank sum test to compare the HRQOL scores of each group. Among active stone formers, individual criterion for MetS were also tested using a Wilcoxon rank sum test (DM vs non-DM, HLD vs non-HLD, HTN vs non-HTN, BMI >30 vs BMI <30). To lend further support to initial results, multivariate analysis was conducted that incorporated MetS status, age, gender, stone recurrence, and past interventions into a linear regression model. This model was designed to predict patient HRQOL scores and the significance of each respective dependent variable on the consequent prediction.
The questionnaires filled by patients without any stones at time of completion were also compiled into another subpopulation (population: prior stone formers). The recorded medical data were surveyed again to identify those who had MetS. Within this subpopulation, those with MetS were compared with those with no MetS using a Wilcoxon rank sum test. As was performed among active stone formers, individual criterion for MetS was tested using a Wilcoxon rank sum test in the prior stone formers subpopulation.
Results
There was a total of 3051 patients whose data were collected (Table 2). Of these patients, 1563 (51.2%) were men and 1488 (48.8%) were women. The mean age of the group was 54.1 years. Most patients were white (83.1%), whereas Latino/Hispanic and Asian populations made up 6.0% and 5.0% of the population, respectively. Other ethnicities included American Indian or Alaska Native, Black or African American, Native Hawaiian, or other Pacific Islander. Of the 3051 patients, 1625 had stones at the time of questionnaire completion. A total of 193 patients who had stones (11.9%) also had MetS.
Demographics
MetS = metabolic syndrome.
Statistical analysis was carried out on active stone formers (Fig. 1). QOL scores of patients with both stones and MetS were compared with QOL scores of patients with stones and no MetS using a Wilcoxon rank sum test, yielding a p-value of 0.049. The median QOL score for the entire population was 105 of a maximum 140 points. Patients with MetS had a median score of 102, and patients without MetS had a median score of 106.
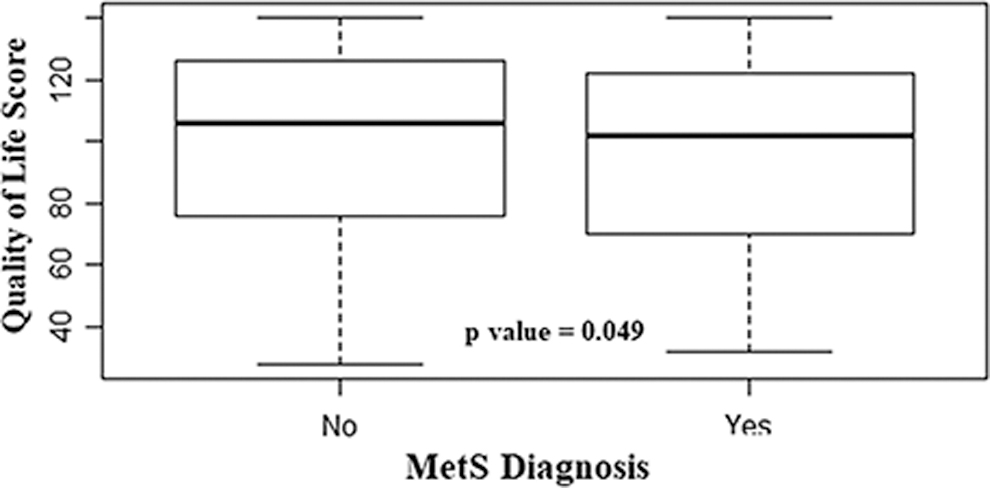
MetS vs no MetS patient comparison. x-axis label: “MetS Diagnosis.” y-axis label: “Health Related Quality of Life Score.” Box plot comparing MetS patients with non-MetS patients. The bold line within each dataset is the median. The median of the population with a positive MetS diagnosis is 102/140, whereas the median of the non-MetS population is 106/140. The dataset was compared using a Wilcoxon rank sum test, which yielded a p-value of 0.049. This result indicates a significant difference between the two populations. MetS = metabolic syndrome.
In the comparisons of individual MetS components among active stone formers, patients with BMI >30 had a significantly lower HRQOL compared with patients with BMI <30 (p < 0.001). DM patients also had a significantly lower HRQOL compared with non-DM patients (p = 0.028). Comparisons with HLD and HTN yielded insignificant results. On multivariate analysis, MetS continued to be a significant predictor of decreased stone-specific HRQOL (p = 0.002) after controlling for other variables including age, gender, stone recurrence, and past interventions. Similar analysis carried out on prior stone formers yielded an insignificant result (p = 0.24), with both MetS and non-MetS patients in this subpopulation yielding a median score of 126.5 of a maximum score of 140. Furthermore, comparisons between patients with and without individual MetS components also yielded insignificant results among prior stone formers.
Stone composition data were also collected (Table 3). In the population of patients with MetS, 65.52% of patients who had prior stones comprised primarily of calcium oxalate (CaOx), 5.17% had primarily calcium phosphate (CaPhos), 3.45% of patients had 50/50 (CaOx and some other stone composition), 20.69% had primarily uric acid, 1.72% of patients had struvite, and 3.45% of patients had cystine. In comparison with the total population, two differences became apparent. Compared with patients without MetS, patients with MetS less commonly had CaPhos (5.17% vs 19.25%) and more commonly had uric acid stones (20.69% vs 9.63%).
Stone Composition
Discussion
Urologists are faced with a variety of management decisions in treating patients with urolithiasis. Asymptomatic or mildly symptomatic stones may be managed conservatively, whereas others with more significant symptoms often require intervention. Several studies have demonstrated lower HRQOL in stone formers compared with individuals without stones. 13,14 Therefore, factors that influence the severity of kidney stone symptoms can be impactful as they have the potential to determine whether kidney stones need to be actively treated. In this prospective study, we evaluated the impact of MetS on kidney stone symptoms by studying stone-specific HRQOL.
In the active stone formers patient subpopulation, it was demonstrated that patients with MetS had a noticeably decreased stone-specific HRQOL compared with patients without MetS. This was corroborated by a multivariate analysis that indicated MetS was the most significant contributor to a decreased HRQOL even in the presence of several confounding variables. We propose that this is because MetS increases the severity of kidney stone disease. There are some data to support this contention, including work by Kohjimoto et al. In that study, severity was determined by increased urinary calcium, uric acid, and oxalate excretion, and decreased urinary citrate excretion. 2 Future work includes a longitudinal study evaluating this contention.
Patients with DM and BMI >30 were associated with a decreased stone-specific QOL as well. Insulin resistance has been cited as a primary attribute of MetS. 2 DM and BMI >30 are closely related to insulin resistance—obesity is thought to induce insulin resistance, whereas DM is a consequent downstream effect. 2 We posit that patients with either DM or BMI >30 exhibit pseudo-MetS characteristics and subsequently also have decreased HRQOL. Previous research exists pointing to a relationship between MetS and stone recurrence, 2,4 but the literature is lean with regard to HRQOL. This study provides an important link between MetS and HRQOL in urolithiasis patients.
Our study also found that the subpopulation of prior stone formers demonstrated similar HRQOL across the board irrespective of whether patients had MetS. This finding indicates MetS alone is not enough to result in a significant difference in HRQOL as measured by the WISQOL. This result has two implications. First, it verifies that the WISQOL measures HRQOL only as it relates to kidney stones—not general HRQOL. This finding is important given that a patient with MetS will generally have a lower HRQOL compared with another patient with no MetS. 6 Second, it validates the supposition that it is indeed the combination of stones and MetS that is resulting in a decreased stone-specific HRQOL. Similar insignificant results were obtained for this subpopulation in the comparisons of individual MetS components. This corroborates the two implications mentioned previously.
There are substantial data revealing an association between MetS and disorders ranging from psoriasis to female sexual dysfunction. 15,16 However, there is a dearth of studies investigating the effect of MetS on patients' tolerance of associated diseases. Although the link between MetS and nephrolithiasis is established, we believe this is the first study to demonstrate an adverse effect on the HRQOL of patients with active stone disease and MetS. To our knowledge, there has been no published mechanism put forward to account for the association of these phenomena. MetS is known to be associated with chronic, low-grade inflammation. 17 Similarly, markers of inflammation have been demonstrated in the urine of nephrolithiasis patients. 18 We propose that inflammation may play a role in the exacerbation of stone symptoms. Further work must be carried out to investigate this connection.
Overall, these findings support a more holistic view of outpatient stone prevention. Physicians may consider advising lifestyle and diet changes that are aimed at reducing the severity of MetS in addition to treating kidney stones. This approach will potentially improve patient HRQOL and may also limit the rate of recurrence or symptomaticity of stones. Identifying techniques successful at improving HRQOL during active stone episodes would be ideal. Further work investigating the effect of directed therapy aimed at tackling MetS on HRQOL in nephrolithiasis patients is necessary. Whereas the North American Stone Quality of Life Research Consortium oversees a longitudinal study of kidney stone patients, our data here are cross-sectional. It will be necessary to follow these patients prospectively to determine whether and how changes in MetS status affect HRQOL.
The assessment of stone composition revealed that the subpopulation of patients with MetS had a higher incidence of uric acid stones (20.69%) compared with the total patient population (9.63%). This finding is well documented in the literature. 19,20 These studies have presented data linking increased uric acid stone formation to type 2 DM, suggesting an abnormally low urine pH may be characteristic of MetS. 21
This study has several limitations that may have impacted our results. The first is with regard to the MetS criteria. The medical history data collected contained data for HLD, HTN, diabetes, and BMI. Waist circumference was not measured across all study sites. We have attempted to address this by using BMI as an approximate for waist circumference as per WHO parameters. 7 This may result in some discrepancy. Another limitation is the cross-sectional nature of this study, which limits the analysis to a single point in time and thus lacks temporal insight.
Conclusion
This study establishes that MetS is associated with intensified kidney stone symptoms to the extent that the WISQOL can distinguish a difference in HRQOL between patients with MetS and those without. Application of this conclusion can include dietary and lifestyle guidance from urologists as a means of improving patient QOL. Taken together with previous findings that suggest a link between MetS and stone recurrence, MetS is an important consideration for physicians with regard to kidney stones. This lends further support to multifactorial, personalized approaches to patient care for stones.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.