
Abstract
Objective:
To evaluate and compare the ability of the Guy's stone score (GSS), the S.T.O.N.E. nephrolithometry, and the Clinical Research Office of the Endourology Society (CROES) nomogram to predict the outcome of mini-percutaneous nephrolithotomy (MPNL) in children, and to identify which of the predictors involved in these scoring systems can separately affect this outcome.
Patients and Methods:
All children younger than 14 years who had MPNL in our center over a period of 3 years were included prospectively. Bivariate analyses were done to evaluate the associations of the three scoring systems and the predictors composing them with single-session stone clearance and complications. Receiver operating characteristic (ROC) curve analyses of the three scoring systems were conducted to evaluate and compare their abilities to predict the outcomes. Decision curve analyses for the three scoring systems were conducted to evaluate the clinical benefit of using each of them to predict stone clearance.
Results:
We consecutively enrolled 92 renal units in 89 children with a median age of 9.5 years. Single-session stone clearance was achieved in 76 (82.6%) renal units. Complications occurred with 19 (20.7%) procedures. Stone multiplicity (p = 0.043), staghorn stone (p = 0.007), prior stone treatment (p < 0.001), number of calices involved (p = 0.006), stone burden (p = 0.003), GSS (p < 0.001), S.T.O.N.E. nephrolithometry (p = 0.012), and CROES nomogram (p < 0.001) had significant associations with stone clearance. Only stone attenuation was significantly associated with complications (p = 0.031). For prediction of stone clearance, CROES nomogram demonstrated the greatest area under the ROC curve and the greatest net benefit on decision curve analyses.
Conclusions:
For children undergoing MPNL, CROES nomogram is the best to predict stone clearance. However, none of the studied scoring systems predicted complications efficiently.
Introduction
After introduction of percutaneous nephrolithotomy (PNL) in adults, it took about a decade to be attempted in children. 1 This delay was due to special concerns in the pediatric population, including the effect of parenchymal violation on a growing kidney and the vulnerability of children for life-threatening complications such as hypothermia, sepsis, and electrolyte imbalance. Moreover, the concurrent advent of extracorporeal shockwave lithotripsy (SWL) as a less invasive technique hindered the initial progress of PNL in children. 2 Later on, experience broadening in adults, development of mini-percutaneous nephrolithotomy (MPNL), and unsatisfactory results of SWL augmented the indications of pediatric PNL. 3,4 Nowadays, PNL has already been established as the primary treatment option for children suffering from staghorn stones, renal stones >20 mm, lower caliceal stones >10 mm, and known cystine or struvite renal stones. 5
In the modern era of patient-centered medical care, appropriate preoperative patient counseling mandates the development of efficient predictive tools for the outcome of any surgical intervention. Such tools are also very helpful in procedure planning, learning curve benchmarking, and data standardization for clinical research. Multiple scoring systems were introduced for prediction of PNL outcomes. 6,7 An interesting observation is that the majority of the predictors composing these scores are different from one system to the other. 8 In spite of the numerous reports validating and comparing these nephrolithometric scoring systems (NSS), there is still no consensus regarding the superiority of a certain system to accomplish the target missions. 6,7
The most popular NSS are the Guy's stone score (GSS), 9 the S.T.O.N.E. nephrolithometry, 10 and the Clinical Research Office of the Endourology Society (CROES) nomogram 11 (Supplementary Appendix). Given that their development depended on data derived from adult populations, in addition to the anatomical and physiological peculiarities of children, doubts can be raised regarding the appropriateness of using these scores in pediatric settings. In this study, we evaluate and compare the ability of the mentioned NSS to predict the outcome of MPNL in children. We also aimed at identifying which of the predictors involved in these systems can separately affect the outcome.
Patients and Methods
During 2015, 2016, and 2017, after the permission of the local committee of medical research ethics, the data of all children younger than 14 years who were prepared for MPNL in our center were recorded prospectively. For patients who had bilateral renal stones, each renal unit had its own record. Preoperative noncontrast computed tomography was done for all patients. Any evident urinary tract infection was treated preoperatively.
Scoring process
For S.T.O.N.E. nephrolithometry and the independent analysis, stone burden was estimated by summation of the products obtained by multiplying the length by the width for each stone, but for the CROES nomogram, these products were multiplied by 0.785, as mentioned in the original description of each score. 10,11 Because skin-to-stone distance was used in S.T.O.N.E. nephrolithometry only, it was measured by the same method described in this score. 10 Mean stone attenuation was obtained on preoperative noncontrast computed tomography. If a case had multiple stones, we registered the grand mean of their attenuations.
During the application of S.T.O.N.E. nephrolithometry, we found two vaguely described domains. To improve the reliability of this score, we had to standardize the way of assigning points for these two domains as follows. First, the demarcation between various degrees of hydronephrosis was not defined clearly. 10 So, we considered the obstruction that did not cause cortical thinning as mild hydronephrosis, which was assigned one point together with no obstruction; whereas the obstruction that caused cortical thinning was considered as moderate or severe hydronephrosis and assigned two points. Second, regarding the method of assessment of the number of calices, it was not clear how to account for pelvic stones. In addition, there was a contradiction between the text, the table, and the supplementary figure regarding the number of points assigned when two calices were involved. 10 We counted the pelvis as a calix, and assigned one point for stones present in one or two calices, two points for more caliceal involvement, and three points for staghorn stones.
A staghorn stone was defined as a stone that occupied the renal pelvis and branched into all calices, whereas a partial staghorn stone (which was assessed in GSS only) was defined as a renal pelvic stone that branched into more than one calix but not all calices. Malrotated kidney, horseshoe kidney, ectopic kidney, duplex system, ureteropelvic junction stenosis, and inclusion of an intestinal segment in the urinary tract were considered as anatomical abnormalities during determination of GSS. Although our center performs more than 200 percutaneous nephrolithotomies in adults yearly, we calculated our case volume according to the rate of pediatric cases only (30 cases/year). The whole scoring process was carried out by the same senior urologist for all patients.
Surgical technique
All procedures were done in prone position after fixation of a ureteral catheter under general anesthesia and antimicrobial prophylaxis. Percutaneous renal access was obtained under fluoroscopic guidance by using a 16-gauge Chiba needle to introduce a floppy-tipped guidewire into the pelvicaliceal system over which 8–10F coaxial dilators were passed. Another stiffer guidewire was then used to guide serial dilation of the tract to place an 18–20F access sheath. Stone disintegration was performed by using ballistic and ultrasonic lithotripters through a 12F rigid nephroscope with a removable 15F outer sheath. A 14F nephrostomy tube was routinely left through the tract and removed after verification of stone clearance followed by removal of the ureteral catheter 1 day later.
Outcome evaluation
Stone clearance was defined as the absence of residual stone fragments larger than 3 mm and was verified by renal ultrasonography and plain X-ray of the urinary tract the next day after the procedure. Complications that occurred within 30 days were recorded and graded according to the Uro-Clavien-Dindo classification system. 12 Operative time included both percutaneous access and endoscopy. Stone clearance after the initial procedure and complications were considered the primary outcomes, whereas blood transfusion and operative time were considered the secondary outcomes.
Statistical analysis
Bivariate analyses were done to evaluate the associations between the three scoring systems and all of the outcomes. We also evaluated the associations between each of the predictors composing the scores and the primary outcomes only. Receiver operating characteristic (ROC) curve analyses of the three scoring systems were done to evaluate their discriminative abilities as classifiers for the primary outcomes. For each ROC curve, the statistical significance of the area under the curve (AUC) was tested by the DeLong et al. method. Decision curve analysis was conducted for the three scoring systems to evaluate their clinical worth when used to guide the treatment decision based on the probability of achieving stone clearance. To plot the decision curves, logistic regression of clearance on each score was first used to obtain the predicted probabilities of clearance.
Two-tailed p-values <0.05 were considered significant. However, since multiple p-values were generated, p-values below an adjusted threshold of 0.001 were also flagged. Statistical methods were implemented on IBM® SPSS® Statistics 23, MedCalc Statistical Software 15.8, and StataCorp LP Stata®/IC 13.0.
Results
This study included 92 renal units in 89 children (Table 1). Stone clearance was achieved after the initial MPNL procedure in 76 (82.6%) renal units. For renal units with residual stones, five had second-look MPNL, six had SWL, and three had both. After these auxiliary procedures, nine more renal units became stone free, making the ultimate stone clearance rate 92.4%. Complications occurred with 19 (20.7%) procedures (Table 2).
Summary of Preoperative, Operative, and Blood Transfusion Data for the 92 Mini-Percutaneous Nephrolithotomy Procedures
Expressed as count (%) for categorical variables and as median (minimum; IQR; maximum) for quantitative variables.
Not necessarily for intraoperative bleeding; in some cases for preoperative anemia.
CROES = Clinical Research Office of the Endourology Society; HU, hounsfield units; IQR = interquartile range; PNL = percutaneous nephrolithotomy; SWL = extracorporeal shockwave lithotripsy.
Complications That Occurred with Mini-Percutaneous Nephrolithotomy
According to the Uro-Clavien-Dindo classification system. 12
Stone multiplicity, presence of a staghorn stone, prior stone treatment, S.T.O.N.E. score for the number of calices involved, and stone burden as a continuous variable and as classified in S.T.O.N.E. nephrolithometry had significant associations with stone clearance after the initial procedure (Tables 3 and 4). For complications, none of the predictors was significant except for stone attenuation as a continuous variable. Meanwhile, stone attenuation as classified in S.T.O.N.E. nephrolithometry (less than vs greater than 950 Hounsfield units) did not show a significant association with complications (Tables 3 and 4).
Associations Between the Nominal Predictors and the Primary Outcomes
0.5 is added to all four cells of the contingency table if there are no events in either group.
Calculated according to Altman.
By Fisher's exact test.
Involved in Guy's score.
Involved in CROES nomogram.
Significant at the 0.05 level.
Involved in S.T.O.N.E. nephrolithometry.
Significant at the adjusted 0.001 level.
CI = confidence interval; RR = relative risk.
Associations Between the Quantitative and the Ordinal Predictors and the Primary Outcomes
Exact p-values by the independent-samples Mann–Whitney U test.
Involved in S.T.O.N.E. nephrolithometry.
Involved in CROES nomogram.
Significant at the 0.05 level.
Significant at the adjusted 0.001 level.
The three scoring systems had significant associations with stone clearance after the initial procedure; none of them was significantly associated with complications (Table 4). All of them had significant associations with both operative time and blood transfusion (Table 5).
Associations Between the Three Nephrolithometric Scoring Systems and the Secondary Outcomes
Exact p-values by the independent-samples Mann–Whitney U test.
CI, where p-values and bias-corrected and accelerated CIs are based on 10000 bootstrap samples.
Significant at the adjusted 0.001 level.
Significant at the 0.05 level.
On ROC curve analyses for the three scoring systems as predictors of stone clearance, each of them showed an AUC that was significantly more than 0.5, with the greatest AUC and Youden index for the CROES nomogram (Fig. 1). For complications, no scoring system showed an AUC significantly different from 0.5 (Fig. 2).
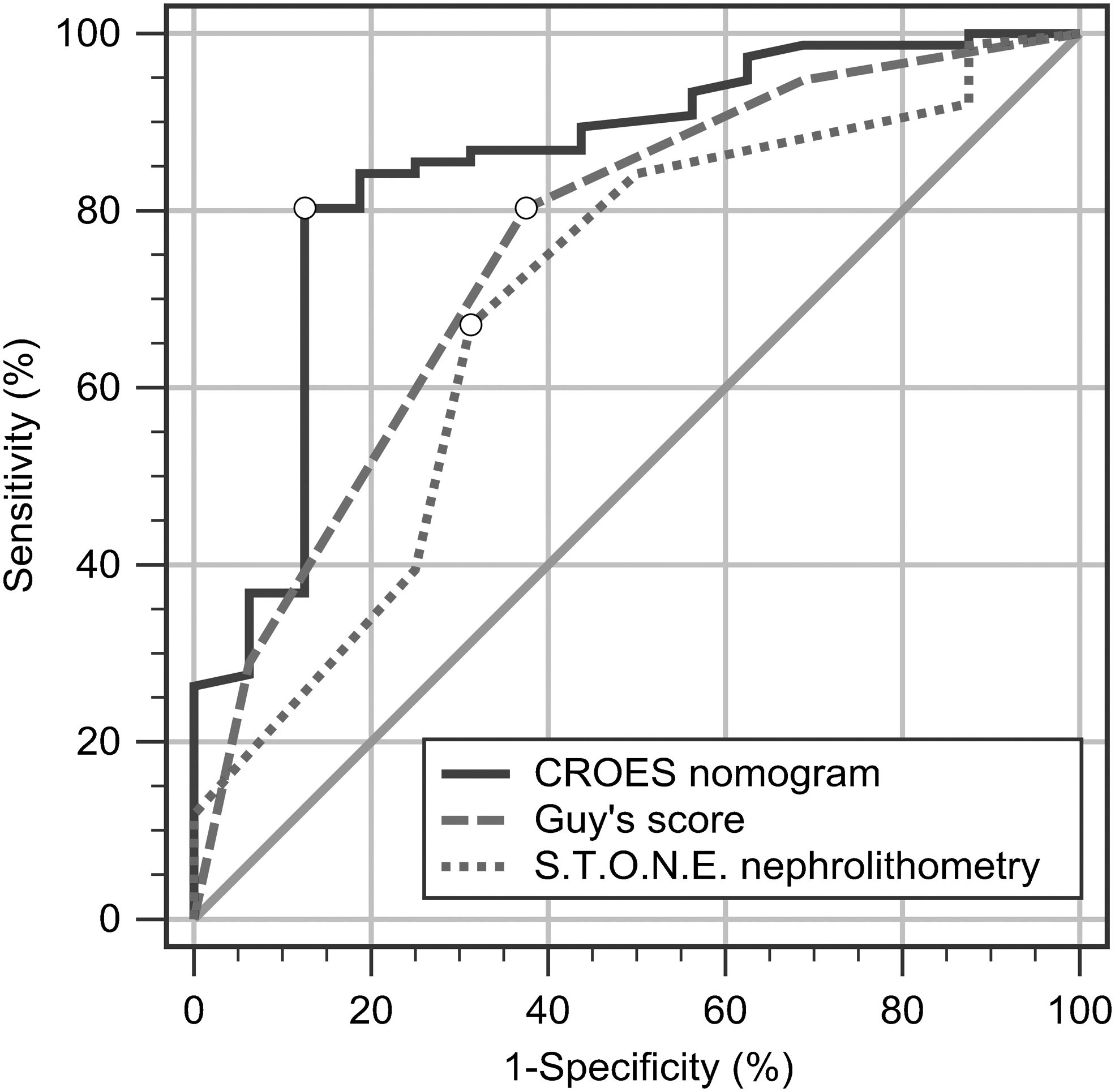
Receiver operating characteristic curves for the three nephrolithometric scoring systems as predictors of stone clearance after a single session of MPNL in children. Circle markers indicate the criteria associated with Youden indices. The area under the curve (binomial exact 95% CI; p-value) is 0.847 (0.757–0.914; p < 0.001) for CROES nomogram, 0.757 (0.657–0.841; p < 0.001) for Guy's stone score, and 0.694 (0.589–0.786; p = 0.011) for S.T.O.N.E. nephrolithometry. CI, confidence interval; CROES, Clinical Research Office of the Endourology Society; MPNL, mini-percutaneous nephrolithotomy.
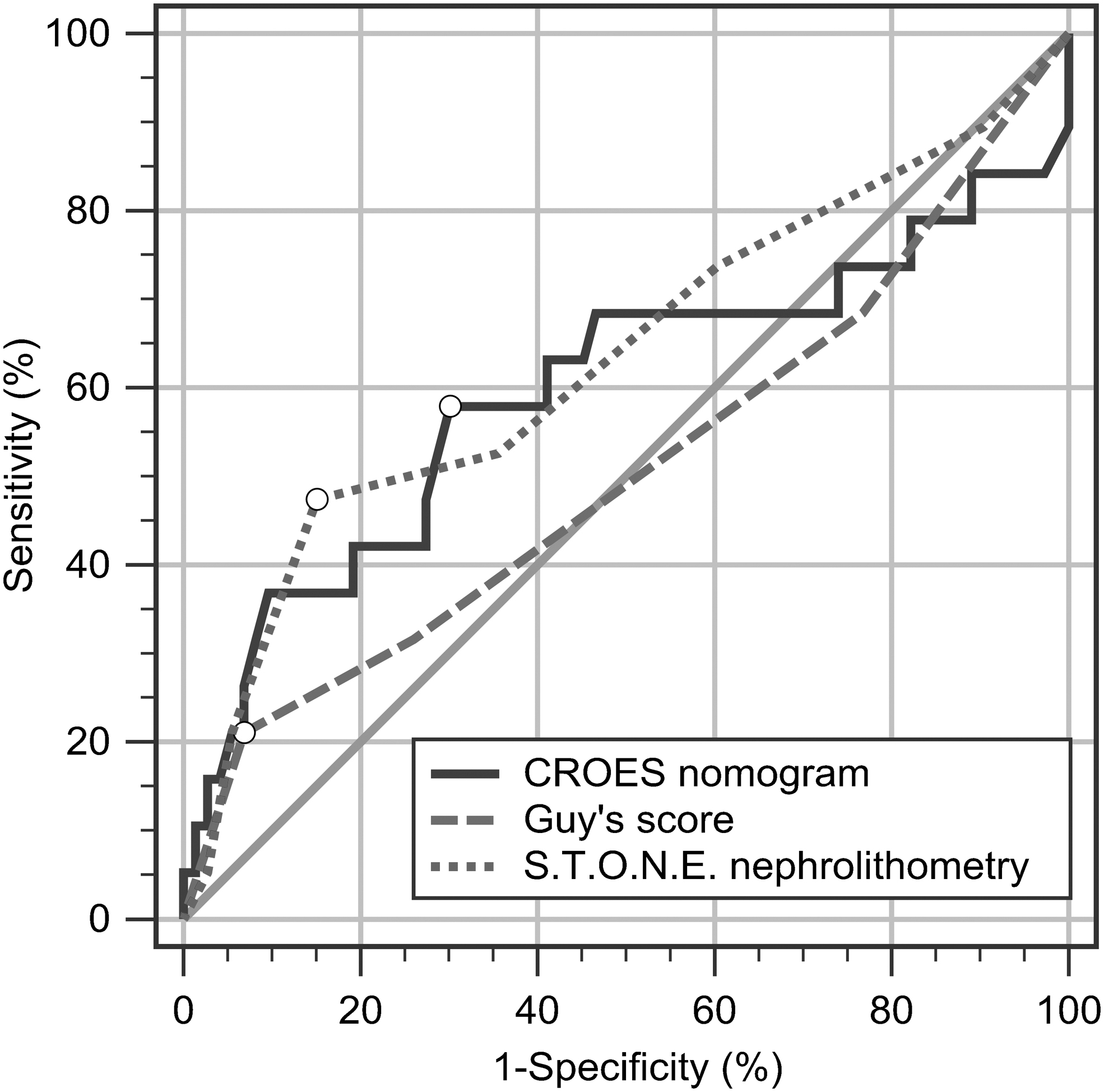
Receiver operating characteristic curves for the three nephrolithometric scoring systems as predictors of complications of MPNL in children. Circle markers indicate the criteria associated with Youden indices. The area under the curve (binomial exact 95% CI; p-value) is 0.596 (0.489–0.697; p = 0.28) for CROES nomogram, 0.507 (0.401–0.613; p = 0.93) for Guy's stone score, and 0.632 (0.525–0.730; p = 0.10) for S.T.O.N.E. nephrolithometry.
On decision analysis curves (Fig. 3), the greatest net benefit was obtained when the treatment decision was based on the CROES nomogram, starting at a threshold probability for stone clearance as low as 40% and consistently at higher probabilities. On the contrary, S.T.O.N.E. nephrolithometry demonstrated an inconsistent curve that lies below the treat-all curve in the threshold probability interval between 60% and 70%.
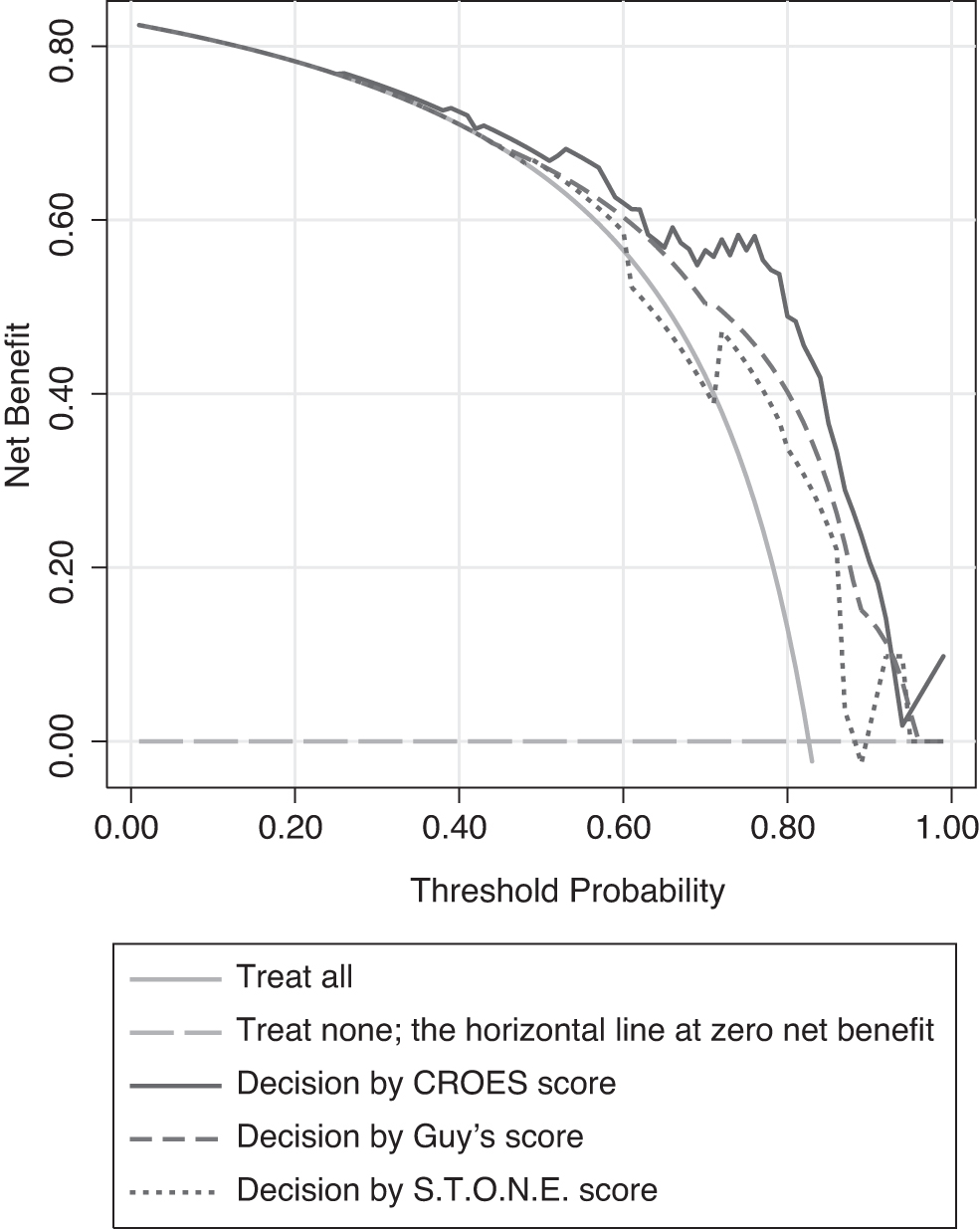
Decision curves for the three nephrolithometric scoring systems comparing the net benefit of using the scores in children to make the decision of MPNL based on the probability of stone clearance.
Discussion
Despite the cautious introduction of PNL in children, it passed the test of time over the past three decades and showed high safety and efficacy with no age limit and an insignificant adverse effect on renal function. 13 –16 The MPNL became favored in children after achieving an efficacy similar to that of using adult-size instruments, with fewer complications. 14,17 Although the NSS have been extensively used, studied, and compared in adult populations, 6,7 the data about their applicability in children are limited and entirely based on retrospective studies. In agreement with our results, they demonstrated the ability of the three NSS to predict stone clearance, but they reported conflicting results regarding prediction of complications. 18 –21
Only two studies were similar to the present work as regards comparing the three NSS in children. 22,23 Contrary to our results, Aldaqadossi et al. 22 found that S.T.O.N.E. nephrolithometry had the highest accuracy for prediction of stone clearance. Also, they found that GSS was associated with complications. These differences may be due to variation in the scoring process that was not clearly delineated in their study. For example, they excluded patients with previous open stone surgery, which is one of the components of the CROES nomogram and was found to affect stone clearance in our cohort.
Recently, Çitamak et al. 23 applied the three NSS on a large dataset and found that the CROES nomogram was the best to predict both success and complications. They also proposed a genuine simple scoring system for prediction of outcomes of PNL in children: the stone-kidney size score. It depends on the number of stones and the relationship between stone burden and renal length. Their new score achieved reasonable performance in prediction of success but questionable ability to predict complications. This score categorizes patients into just three grades that cannot accommodate the whole spectrum of renal stone complexities. Moreover, it still needs further evaluation as it was derived from a retrospective dataset extending over 20 years and involving heterogeneous imaging methods, surgical techniques, and instrument sizes.
The development of GSS was based on a literature review, expert opinions, and a plan/do/study/act process. 9 Oddly, it did not include a direct evaluation of stone burden in spite of its proven effect on the outcome of PNL. 24,25 Of the predictors involved in this score, stone multiplicity and presence of a staghorn stone were found to affect stone clearance in our study. Our cohort did not include any case with a caliceal diverticulum, spina bifida, or spinal injury, so these items were not evaluated. The GSS was unique to involve the abnormal renal anatomy among its predictors. However, many studies denied the effect of renal anatomical abnormalities on the outcome of PNL. 26,27 Moreover, the absence of concrete definitions for an abnormal renal anatomy and a partial staghorn stone threatens the reproducibility of the score, as mentioned by its creators. 9
S.T.O.N.E. nephrolithometry contains five predictors that were determined after a systematic review of the literature and a retrospective pilot study. 10 Two predictors were found to affect stone clearance in our study: stone burden and S.T.O.N.E. score for the number of calices involved, which also entails the presence of a staghorn stone. However, the indeterminate description of the method of counting the involved calices weakens its reliability. 28 The other three predictors are exclusive for this score and essentially did not show a significant effect on stone clearance even in the initial report of the score. 10 Although there are some conflicting reports about the adverse effects of obesity and a long stone-to-skin distance on the outcome of PNL in adults, 25,29 it is of negligible importance in children due to the constantly short stone-to-skin distance.
The CROES nomogram was derived through a multivariate logistic regression analysis of multi-institutional data of 2806 patients. 11 This can be considered the most powerful and rigorous method in comparison with the other scoring systems. All of the predictors included in this score showed a significant effect on stone clearance in our study except for stone location. This can be attributed to the dealing with multiple stone locations as a single entity without discrimination according to the number and sites of involved calices. The main concern against this score is its complexity, which may hinder its clinical use. This can be solved by developing a software application that directly calculates the chance of stone clearance.
Although morbidity is not less important than efficacy as a surgical outcome, all of the three NSS share the same weakness and inconsistency in predicting complications. 6 In our study, stone attenuation was the only predictor that was significantly associated with complications. This can be explained by the need of harder stones for more manipulations during disintegration. In a large-scale study, Onal et al. 14 found that operative time, sheath size, a midcaliceal access, and a partial staghorn stone are the independent factors influencing complications of PNL in children. Most of these factors are intraoperative and so cannot be included in a preoperative score.
Another confusing issue in the assessment of renal stone complexity is the exact description of a staghorn stone. Attaining variable volumetric and morphological criteria, staghorn stones cannot be dealt with as a one-grade item to the extent that Mishra et al. 30 developed a specific classification system to assess their complexity.
As these NSS were developed primarily for adults, they did not take age into consideration. Although we did not find significant associations between age and MPNL outcomes, sub-stratification of pediatric patients according to age may reveal a substantial difference in the performance of NSS among different pediatric age groups.
In this study, the sample size was inadequate for a multivariate analysis. A meta-analysis, future extension of the study, or multi-institutional cooperation may yield a more powerful sample size. Another limitation in our study is that we did not assess the interobserver variability for the proposed NSS.
Conclusions
The CROES nomogram is the best among the studied NSS to predict single-session stone clearance of MPNL in children. More accuracy may be achieved after modification of the stone location item and grading of the staghorn stone item. None of the studied NSS is efficient regarding prediction of complications. A thoughtful eye is needed to put the edges of this puzzle together and invent a comprehensive scoring system for prediction of the outcome of MPNL in children.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.