
Abstract
Objective:
The objective of this study is to compare the use of three-dimensional (3D) vision systems with traditional two-dimensional systems in laparoscopic urological surgery, analyzing the benefits, limitations, and impact of introducing this medical technology with regard to surgical performance and the surgeon's ergonomics.
Methods:
A systematic review with a structured bibliographic search was conducted in the electronic libraries (PubMed and EMBASE) until August 2019 and with no language restrictions. Studies on 3D visualization technology in laparoscopic urologic surgery, randomized controlled trials, and observational comparative studies were included. Relevant data were extracted and analyzed.
Results:
A total of 25 articles were obtained, of which 4 were clinical studies with patients, 2 studies were carried out in experimental animal models, and the remaining 19 were conducted in simulated environments. Regarding the European training program in basic laparoscopic urological skills, the results showed no significant differences in execution time using either imaging system. Three-dimensional vision led to a significant reduction in surgery time in pyeloplasty and radical nephrectomy. In addition, there was a reported decrease in blood loss in adrenalectomy, nephron-sparing nephrectomy, radical nephrectomy, simple nephrectomy, and pyeloplasty using 3D vision. Regarding ergonomics, the studies generally described no differences in side effects (headache, nausea, eye strain) when comparing the two types of visualization systems. Surgeons reported reduced workloads and stress with 3D vision than with traditional laparoscopy.
Conclusions:
Three-dimensional laparoscopic systems essentially advance surgical performance in less-experienced laparoscopic surgeons. Three-dimensional laparoscopy leads to improvements in surgery time, which is important for specific surgical procedures involving intracorporeal ligatures and sutures. The results achieved on the surgeons' ergonomics showed better depth perception and decreased stress and workloads during 3D vision with no differences in potential side effects.
Introduction
Minimally invasive surgery (MIS) has signaled an undeniable revolution in the field of surgery over the last 30 years, progressively replacing open surgical procedures due, in part, to technological developments such as advanced imaging systems and the introduction of surgical robotics, as well as acceptance by medical consensus of different laparoscopic techniques. 1 –3 This approach has been applied to numerous surgical procedures, and the general belief is that it will continue to spread in the coming years. 4
The scope of laparoscopic surgery is largely due to the clear benefits it brings to patients, causing less surgical damage, fewer complications and pain, and a faster recovery compared with open surgery. 5,6 However, this type of approach also entails some limitations for the surgeon due to the need to manipulate the instruments and devices at a distance using a two-dimensional (2D) image displayed through screens or monitors. Therefore, adequate training is mandatory before performing this type of surgical technique in a real surgical scenario. 7
The miniaturization of imaging systems and the current development of high-definition (HD and 4K) and three-dimensional (3D) video technologies provide a high-quality surgical vision similar to that offered by open surgery. 8,9 These innovative imaging technologies enable surgeons to have a shorter learning curve and greater surgical precision. 10
In the case of 3D vision technology, which has not yet been universally implemented, except in robotic laparoscopic surgery, the general feeling has been that it improves surgeon performance and reduces surgery time compared with classic 2D laparoscopy and that high-definition imaging can also provide benefits for optimal clinical results. 10 Therefore, in this work, we carry out a systematic review of the scientific literature with the aim of evaluating the effectiveness and safety of 3D laparoscopic vision, comparing the results with traditional 2D vision and paying special attention to surgical procedures in the urology specialty. This study will seek to determine the benefits, limitations, and impact of introducing this medical technology with regard to surgical performance and surgeon ergonomics.
Materials and Methods
Search strategy
A structured bibliographic search was conducted in the PubMed and EMBASE electronic libraries. We used the key terms “three-dimensional imaging,” “3D,” “Laparoscopy”, “Urology,” “Urological Surgery,” “Urologic Surgical Procedures,” “Performance,” and “Ergonomics” in appropriate combinations to identify relevant studies published up to August 2019 and with no language restrictions (see “Appendix A1” for the full search strategy). Studies on 3D visualization technology in laparoscopic urological surgery, randomized controlled trials, and observational comparative studies were also included.
Selection of articles
Articles that met any of the following criteria were excluded: case reports, retrospective observational comparative studies, studies that addressed only 3D laparoscopy without a comparison to 2D systems, conference abstracts, or articles published in a language other than English. A flowchart with the different phases of the systematic review was designed according to the recommendations of the PRISMA declaration. 11
Data extraction
In each article, general information such as population and detailed information about the task or surgical procedure and experience level of the surgeons were gathered. In addition, relevant data were extracted and analyzed, including the number of surgeons and/or patients, surgery time, estimated blood loss, complications and other assessment criteria for surgical performance, ergonomics and evaluation methods, including statistical significance where appropriate.
Data analyses
A meta-analysis was carried out to compare the surgical performance using 3D and 2D vision by analyzing the execution time and errors in laparoscopic training tasks, as well as surgical time in urological procedures. The results are presented as forest plots with 95% confidence intervals (CIs). A random-effects model was used, and the heterogeneity of the studies was assessed using the I2 statistic. Summary results are presented as diamonds whose extremities show the CI for the summary estimate. When individual studies were too dissimilar to determine an average estimation of the effect (meta-analytic), summary values were omitted. All statistical analyses were carried out using R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
The bibliographic search in the PubMed electronic library generated a total of 114 articles, of which 15 were not written in English and 72 corresponded to an incorrect subject. Moreover, we also found the presentation of a clinical case and 2 reviews, so the search was narrowed to 24 articles. Regarding the EMBASE search, once the established inclusion and exclusion criteria were applied, 199 articles were generated, of which 74 were duplicated in the PubMed search. Of the remaining 125 articles, one article was written in a language other than English, 35 were conference abstracts, and 88 corresponded to incorrect subject matter, reducing the search to 1 article. Therefore, the bibliographic search of the electronic libraries consulted (PubMed and EMBASE) produced a total of 25 scientific articles (Fig. 1).
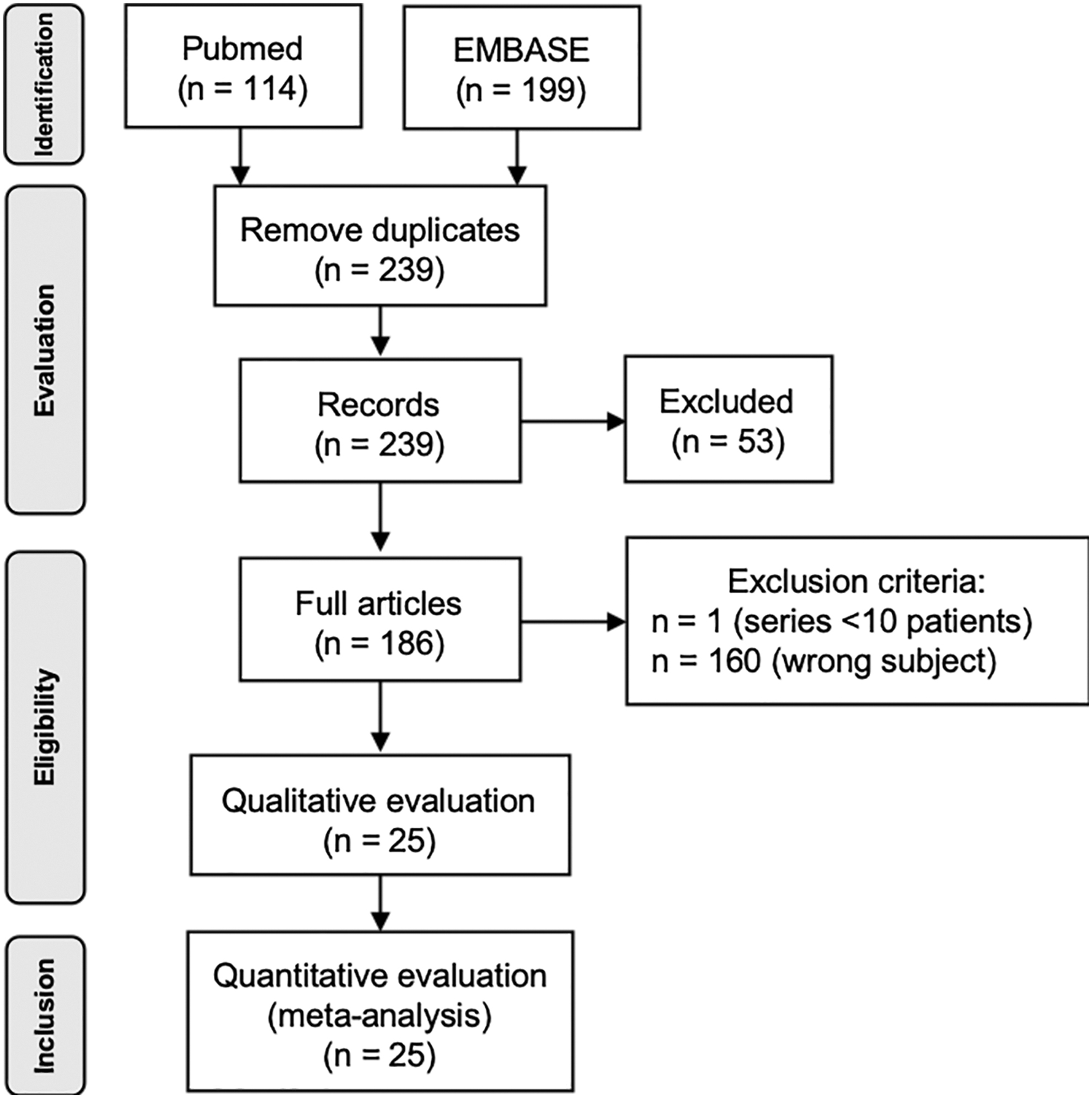
Screening flowchart.
Of the 25 studies included in the analysis, 4 were clinical studies with patients, 2 were carried out in experimental animal models, and the remaining 19 were conducted in simulated environments. The greatest number of articles on the subject analyzed were published in 2015. The first study in the scientific literature that compared the use of 2D and 3D vision systems in laparoscopic urology was from 1996. 12
The most commonly used 3D imaging systems were the Karl Storz FULL HD 3D System (Karl Storz GmbH & Co. KG, Tüttlingen, Germany) 13 –21 and the Viking 3D HD Laparoscopic Vision System (Viking Systems, Inc., La Jolla, CA). 22 –30 Additionally, the Einstein Vision 3D (Schoelly-Fibreoptic GMBH, Germany) was used in some studies. 31,32 Others, such as McDougall et al., conducted their studies with the Endolive Stereo Endoscope (Carl Zeiss, Oberkochen, Germany) and the StereoVu Video Laparoscopen (Welch Allyn Surgical Imaging Systems, Skaneateles Falls, NY) systems. 12 Sun et al. used the DeepVision 3D video system (Automated Medical Products Corp). 33 In addition, other studies used the 3D vision system implemented in the da Vinci Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA). 34 –36
Task time
With regard to the European training program for basic laparoscopic urological skills (E-BLUS), although there was a tendency to reduce the execution time with the use of the 3D vision, for both the novice and expert surgeon groups, the meta-analysis shows no statistically significant differences in the use of either imaging system (Figs. 2 and 3).

Forest plots. Execution time for the E-BLUS tasks performed by novice surgeons:
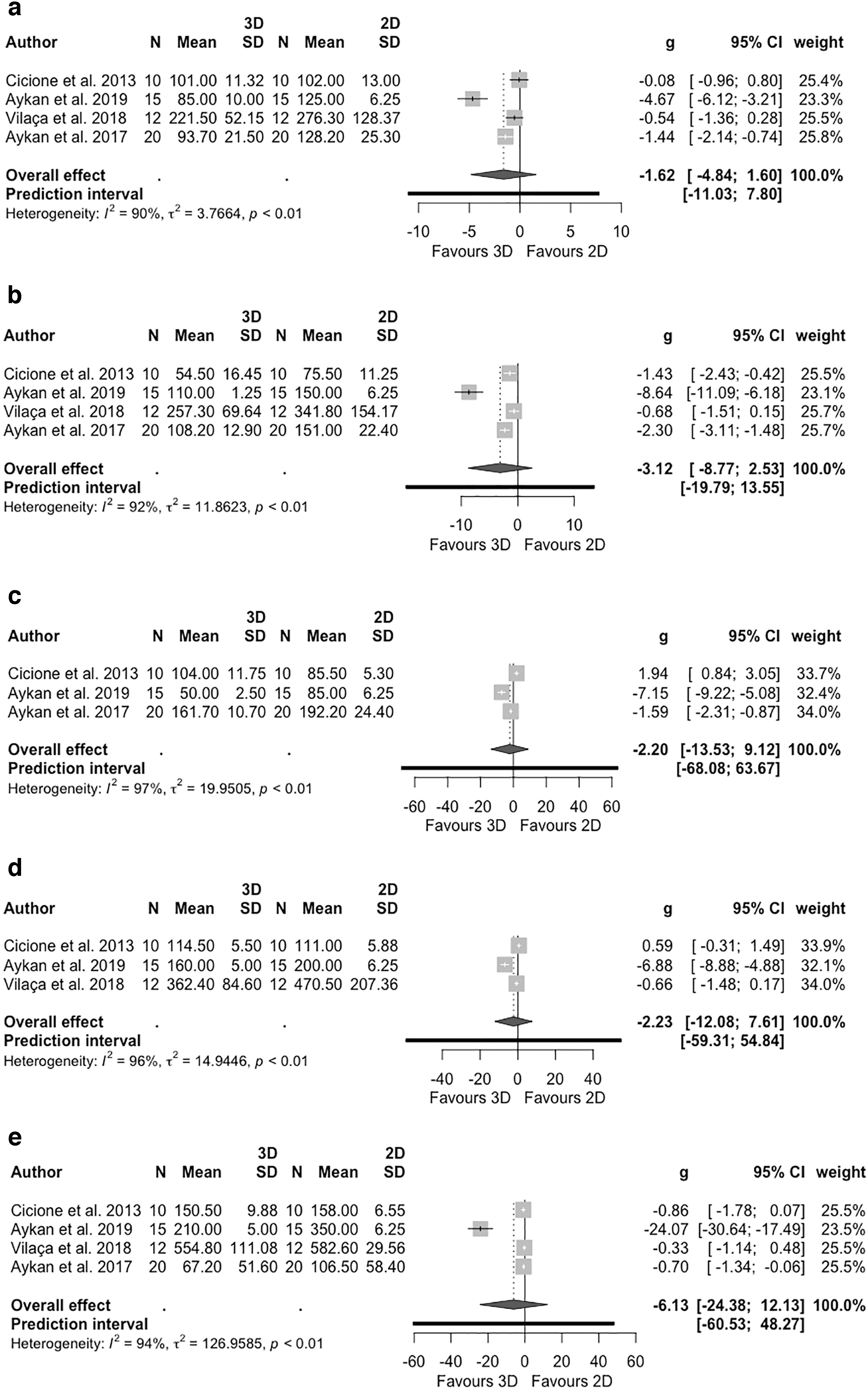
Forest plots. Execution time for the E-BLUS tasks performed by experienced surgeons:
The time required to complete the peg transfer (elastic bands and pegs), 26,30,34 needle guidance, 25,28,34 and cutting and suturing 26 tasks was shorter for all groups of surgeons (novices, intermediates, and experts) using 3D vision (Table 1). The overall time for the fundamentals of laparoscopic surgery (FLS) tasks was better for novice surgeons with 3D vision than with 2D vision. 31 In addition, 3D vision shortened the operative time for vesicourethral anastomosis for novices and expert surgeons. 22,35 It was observed that the execution time and the accuracy of linear cutting and suturing, curved cutting and suturing, dorsal vein complex suturing, and vesicourethral anastomosis were improved for novice surgeons using 3D vision. 29
Results for the Surgical Performance in a Box Trainer Setting Using Three-Dimensional and Two-Dimensional Imaging Systems
CI = confidence interval; 2D, two-dimensional; 3D, three-dimensional; E = experts; FLS = fundamentals of laparoscopic surgery; I = intermediates; N = novices; NA = not available; NS = not statistically significant; VUA = vesicourethral anastomosis.
Errors
Analyzing the errors during the E-BLUS tasks, the novice surgeons reduced the number of mistakes during the eye/hand coordination, cutting and suturing tasks when using 3D vision 21,26,28,32 (Fig. 4). On the other hand, although the expert surgeons reduced the number of errors during the needle guidance task using 3D imaging, the novice surgeons showed an increase with respect to 2D vision. 14 In addition, the surgeons showed fewer errors in favor of the 3D vision systems during the performance of peg transfer, eye/hand coordination, and cutting and suturing tasks. 26,32
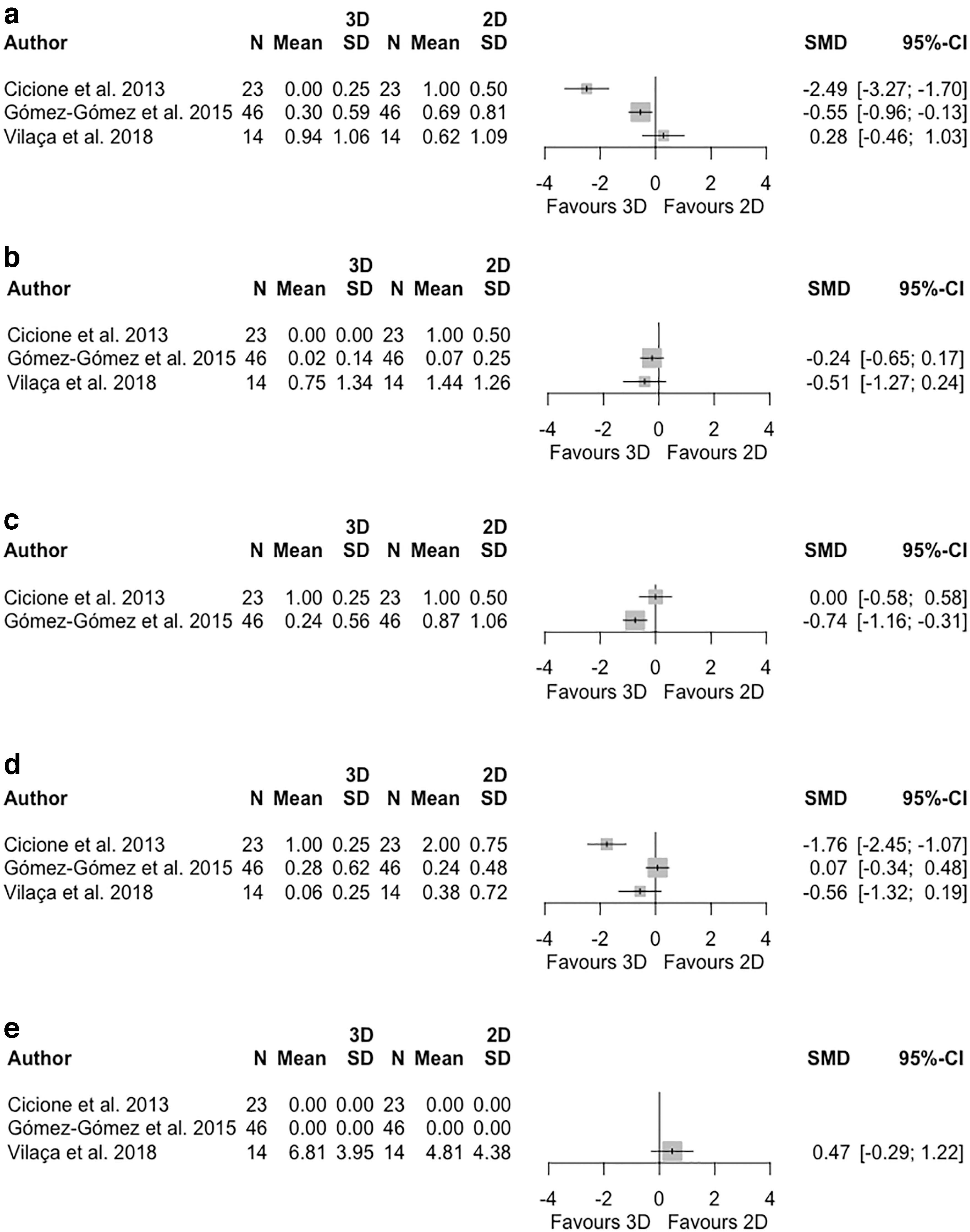
Forest plots. Errors for the E-BLUS tasks performed by novice surgeons:
Surgery time
The results of the meta-analysis show that the use of 3D imaging systems led to a significant reduction in surgery time in pyeloplasty and radical nephrectomy (Fig. 5). In addition, this reduction was also reported in nephron-sparing nephrectomy and ureterolithotomy 13 procedures (Table 2). The time required to complete the critical steps during adrenalectomy, nephron-sparing nephrectomy, radical and simple nephrectomy, pyeloplasty, and ureterolithotomy was shortened using 3D vision. 13 Furthermore, a reduction in dissection time was reported for simple nephrectomy 23 and pyeloplasty 19,23 when using 3D vision systems. The efficiency score for pyeloplasty and partial nephrectomy was better using 3D imaging compared with conventional 2D technology. 19 Similarly, novice surgical assistants performed surgical tasks more efficiently during radical prostatectomy using 3D vision. 27 There was a reported decrease in blood loss during adrenalectomy, nephron-sparing nephrectomy, radical nephrectomy, simple nephrectomy, and pyeloplasty using 3D vision. 13,23

Forest plots. Surgery time for
Results for the Surgical Performance in an Operating Room Setting and with Experimental Models Using Three-Dimensional and Two-Dimensional Imaging Systems
A = physician assistant; OR = operating room.
Ergonomics
The studies generally reported no differences in side effects (headache, nausea, eye strain) when comparing both types of visualization systems 22,26 (Table 3). However, the study from Gómez-Gómez et al. described significantly higher incidences of headache and visual distress using the 3D imaging system. 17 In contrast, the study from Özsoy et al. reported better visual comfort when using 3D vision. 18 Novice surgeons reported a significant reduction in overall workload when using 3D vision compared with 2D vision during laparoscopic training 17,18 (Table 3). However, their satisfaction with the surgical performance was more favorable with 2D vision. 17 Regarding the stress experienced by surgeons during the surgical procedures, the use of 3D imaging systems in laparoscopic urological procedures resulted in lower stress than using traditional laparoscopy. 13,23
Results for the Surgeon's Ergonomic Factors Using Three-Dimensional and Two-Dimensional Imaging Systems
p < 0.05, ** p < 0.01, *** p < 0.001.
IQR = interquartile range; NASA-TLX = NASA task load index; STAI-6 = State-Trait Anxiety Inventory for Adults.
Discussion
The lack of depth perception is one of the main limitations of traditional 2D imaging systems. 14 Three-dimensional vision can effectively improve spatial orientation and depth perception during laparoscopic procedures and facilitate the performance of certain complex surgical maneuvers. 18,32 Following early research, 37 which determined that 3D vision could enhance laparoscopic skills in a laboratory, many studies have been conducted to determine the contribution of 3D vision to laparoscopic training and surgery. 38 –40 However, a Cochrane review in 2011 showed no significant differences during a standard laparoscopic procedure, such as laparoscopic cholecystectomy, in the use of 3D or standard 2D vision. 39 On the other hand, more recent studies suggest that 3D systems bring improvements to laparoscopic practice. 13,14,22 Therefore, this topic, which has been discussed since its origins, should be the subject of further research.
Of the 25 studies included in this review, most (19 in total) were carried out in a box trainer setting, including one study on single-port laparoscopic surgery 14 and another combined with the ETHOS™ operating ergonomic chair (ETHOS Surgical, Portland, OR, USA). 16 There were two studies on an experimental model 12,19 and only four clinical studies. 13,15,23,27 Considering the above, it is clear that more clinical studies are needed in urological surgery to reinforce conclusions regarding the influence of 3D vision in this surgical discipline. Apart from the present analysis, we found previous studies that examined the use of 3D imaging in urological procedures but did not take into account training programs or ergonomic aspects as well as a European consensus regarding its use in different laparoscopic surgical disciplines. 41,42 To the best of our knowledge, this is the first systematic review and meta-analysis carried out with respect to surgical performance and the surgeon's ergonomics in 3D laparoscopic urological surgery, including both training tasks and surgical procedures.
The European Association of Endoscopic Surgery (EAES) presented in 2018 a consensus to establish a set of evidence-based statements and recommendations for the use of 3D vision in laparoscopy. 41 They included randomized controlled trials and prospective studies, addressing different subjects such as general topics, organ-specific data, and ongoing trials. For the organ-specific studies, the impact of 3D vision on operative time and complications were mainly analyzed. Dire et al. also examined the effect of the use of this vision technology on operating time and estimated blood loss in urological procedures. 42 However, the procedures were limited to partial nephrectomy, pyeloplasty, and radical prostatectomy. Laparoscopic training tasks, execution errors, and ergonomic parameters were not taken into account.
It seems that laparoscopic 3D imaging may be beneficial during the initial learning process, especially for less advanced surgeons using physical simulators. The results showed that, in general, the use of 3D vision technology led to a reduction in the execution time for laparoscopic training tasks. 19 The time required to complete eye/hand coordination tasks such as peg transfer, elastic bands, or needle guidance was shorter using 3D vision compared with conventional 2D. 25,26,28,30,34 In addition, the number of achieved goals and transferred objects during the same period of time were also higher during needle guidance and peg transfer tasks, respectively. 18
The use of 3D vision technology clearly provides better depth perception and spatial location and therefore assists in the execution of eye/hand coordination tasks. Similarly, it was reported that surgeons required less time, improving cutting accuracy and average cutting time using 3D imaging systems. 18,22,26,29 Regarding the suturing tasks, such as knot tying, simple suturing or complex suturing, 3D vision improved the surgical performance regardless of the experience of the surgeon. These improvements were mainly in the number of knots, execution time, and accuracy. 18,22,26,29
In general, surgeons showed an improvement in the execution time established in the European training in basic laparoscopic urological skills (E-BLUS) program when using 3D vision. 21 These results were remarkable during eye/hand coordination tasks such as peg transfer or needle guidance, 18,22,25,26,28 –30,34 which were mainly designed to assess ambidexterity, among other surgical skills. 43 Novice and expert surgeons also required less time to complete vesicourethral anastomosis compared with conventional 2D vision, 22,35 showing a higher procedural accuracy among the novice group. 29
In the case of the FLS program, there was a low number of experienced participants. Only one study examined the overall execution time, 31 which was significantly improved in the group of novice surgeons using 3D vision. That expert surgeons had similar results using 2D and 3D vision in the development of basic laparoscopic tasks could be due to having been trained mainly with traditional 2D imaging systems, which has given them certain skills to overcome several of its limitations.
There was an overall reduction in the number of errors made in eye/hand coordination, and cutting and suturing tasks using 3D vision technology. 18,21,26,28,32 This may be due to improvements in depth and spatial orientation over traditional 2D displays. Another study also stated that the use of 3D imaging systems improves laparoscopic box trainer task completion time and error rate. 41
Studies involving the E-BLUS program showed a high disparity in the type of tasks used, thereby increasing the variability of the results obtained and hampering the statistical analysis (meta-analysis) (Fig. 4). Overall, a reduction in the number of errors was shown when using 3D vision. 17,22 Specifically, novice surgeons made fewer errors using 3D imaging systems, mainly in tasks that were more demanding and required greater depth perception (suture and needle guidance). 17 Experienced surgeons showed no differences in errors with either imaging system. 14,21 This demonstrates that the use of 3D vision may not be a critical factor in performing standardized urological training tasks for surgeons with previous laparoscopic backgrounds.
All analyzed studies conducted in a clinical setting or with an experimental animal model were performed by experienced laparoscopic surgeons. One study in a porcine model also included 18 surgeons without any previous laparoscopic experience who had attended a training course in urological surgery. 19 The use of 3D vision was shown to allow surgeons to reduce the surgery time of adrenalectomy, nephron-sparing nephrectomy, simple and radical nephrectomy, pyeloplasty, and ureterolithotomy. 13,23 In particular, the time spent performing critical steps, such as dissection of the renal pedicle, needle position and driving, suture placement and tissue edge holding, was reduced compared with the use of conventional laparoscopic vision. 13,19,23 It seems that the use of 3D imaging systems leads to improvements in surgery time mainly in surgical procedures involving intracorporeal ligatures and sutures. This imaging technology enables surgeons to perform complicated and crucial surgical maneuvers more quickly and safely. 15,19,44
The present review included one study with radical prostatectomies, 27 but no information on surgery time was reported. Nevertheless, other studies have shown a significant reduction in operating time in this procedure using 3D imaging systems. 41,42 Unlike the present study, Dire et al. reported no significant difference in surgery time for pyeloplasty using 3D and 2D vision. 42 One of the three studies included was a retrospective study in children and another was a study in Chinese, which were not included in the current systematic review.
Some studies reported a reduction in blood loss for adrenalectomy, simple nephrectomy, pyeloplasty, and nephron-sparing nephrectomy procedures with 3D imaging systems. 13,23 According to a number of studies, this type of imaging technology makes it possible to better identify vascular structures, which allows for enhanced dissections and therefore less blood loss and improved bleeding control. 13,23 As previously mentioned, 3D vision improves eye/hand coordination and depth perception, which implies an amelioration in the identification of the different anatomical structures and thus in the precision of the execution of the different surgical steps. 23
Studies have shown that 3D vision improves the efficiency of novice surgeons, including surgical assistants, during radical prostatectomy, pyeloplasty, and partial nephrectomy. 19,27 This group of surgeons appeared to experience improvements in accuracy and efficiency during laparoscopic urologic surgery using these types of vision systems. 45
Ergonomics has been mainly assessed by means of subjective assessment methods such as NASA task load index (NASA-TLX), State-Trait Anxiety Inventory for Adults (STAI-6), and personalized questionnaires. Only the study of Aykan et al. 22 included an objective measurement to analyze handgrip strength after the completion of tasks using 2D and 3D imaging systems. It would have been desirable to have carried out these measures during the development of the activities instead. Performing an objective assessment with regard to the effect that novel medical equipment has on the surgical working environment is a crucial aspect for assessing its adequate adaptation to the clinical requirements and its benefits and limitations during its use.
The application of ergonomic principles in surgery is fundamental for the implantation of new medical technology, mainly due to frequent complaints from laparoscopic surgeons. However, an adequate and comprehensive objective methodology has yet to be standardized. Some groups are working on defining a standard framework and objective assessment method for ergonomic analysis in laparoscopic surgery. 46 –48
Taking into account the subjective evaluation regarding the use of 3D imaging systems in urological laparoscopy, improvements in surgical performance and greater comfort for the surgeons have been reported, 23 indicating the suitability of this technology for its use in advanced surgical conditions, in reduced spaces and in complex surgeries. 15 Image quality and depth perception were also positively evaluated with 3D vision systems. 13
During laparoscopic training, novice surgeons reported a significant reduction in general workload when using 3D vision compared with 2D vision. 17,18 However, their satisfaction with surgical performance was more favorable using 2D vision. 17 This result is somewhat contradictory, as the participants obtained a remarkable reduction in execution time with the use of the 3D vision system. 17 This surgeon's perception of surgical performance could probably improve after a period of comprehensive training with this new technology. Arezzo et al. also stated that 3D laparoscopy may result in decreased experienced cognitive workload provided that the viewing setup is optimal. 41
In terms of the stress experienced by surgeons during laparoscopic urological procedures, the use of 3D systems has resulted in less stress than traditional laparoscopy. 13,23 This may be because 3D imaging addresses the lack of depth perception in conventional laparoscopic surgery, which may have led to a decrease in the stress caused during surgery.
Overall, no differences in side effects (headache, nausea, eye strain) were observed using both 3D and 2D vision systems during surgery. 13,15,22,23,26 However, some studies reported an increase in headache and visual discomfort with the use of 3D imaging systems. 17,19 These side effects may be due to the need to wear special glasses to perceive the 3D effect. Some studies also pointed out that the weight of the 3D vision glasses is a problem that should be addressed, although this problem currently seems to have been solved. 12,27
There are clear differences in the cost of 2D and 3D laparoscopy equipment. In general, 3D vision equipment is more expensive than 2D. 49 Although the purchase of a 3D imaging system can be up to 66% more expensive than a conventional 2D laparoscopic system, 50 eventually 3D imaging systems have shown a considerable benefit in terms of blood loss, operative time, and hospital stay, resulting in a reduction of the costs associated with the intervention. 50,51 In addition, improved depth perception, surgical precision and hand/eye coordination with 3D laparoscopic systems allow for reduced surgery time, thus reducing cost, exposure time to anesthesia and morbidity. 51,52 This means better patient safety and therefore shorter hospitalization time and lower costs related to postoperative hospital stay. 51 However, further studies and progress are needed to make the 3D imaging systems more cost effective.
Imaging and display technology are paramount in robot-assisted systems providing the primary method of feedback to the surgeon. In certain cases, the implementation of 3D vision in surgical robotic systems differs from the one used in a conventional laparoscopic approach. The da Vinci System is the most widespread surgical robotic platform, which uses a stereoscopic vision system with dual independent displays, one for each eye. This robotic platform has no force feedback, so visual feedback is vital for the surgeon. Ques such as shadows, motion parallax, and binocular cues are used to estimate location in 3D space of the end effectors, while tissue deformation is used to estimate gripping and prodding force being applied. 53,54 Currently, there are other robotic systems such as Hugo (Medtronic, Dublin, Ireland), Senhance™ (TransEnterix, Morrisville, NC), and Versius™ (CMR Surgical, Cambridge, UK), among others that use flat panel polarized 3D display technology for visualization of the intervention workspace. 53,55,56 Several studies have reported the added value of 3D vision in robotic surgery compared with conventional 2D vision. They showed that the use of 3D visualization improves the efficiency of surgical skills and reduce performance time, 34 improving surgical performance during anastomosis. 35,57
The benefits of 3D vision in surgical performance during standardized urological training tasks were more evident in the group of surgeons without a background in laparoscopic surgery. The results showed that the use of 3D imaging systems leads to improvements in surgery time, mainly in surgical procedures involving intracorporeal ligatures and sutures. Similarly, this type of imaging technology facilitates the identification of anatomical structures, enhancing the precision of maneuvers and the control of blood loss during urological procedures. With respect to surgeons' ergonomics, 3D vision systems provide better depth perception and reduce stress and general workload during surgery compared with traditional vision systems with no differences in potential side effects. Studies in urological surgery with this type of technology are still scarce. Further research is needed to draw more robust evidence-based findings regarding the implications of the use of 3D vision in laparoscopic urological surgery.
This review has some limitations. The number of studies included in the systematic review is limited, especially the number of randomized controlled trials in laparoscopic urological procedures. Although 3D vision has been widely implemented in surgical robotics, only three studies in this review involved robotic surgery, two of which investigated the use of the 3D technology for the bedside assistant. In addition, there is a lack of studies that apply objective assessment methods to the surgeon's ergonomics. Most studies used subjective questionnaires regarding experience in the use of this vision technology.
Conclusions
The benefits of 3D vision in improving surgical performance in standardized urological training tasks are more evident in the group of surgeons without a background in laparoscopic surgery. The results showed that the use of 3D imaging systems leads to improvements in surgery time, mainly in surgical procedures involving intracorporeal ligatures and sutures. With respect to surgeons' ergonomics, 3D vision provides better depth perception and reduces stress and workloads during surgery compared with traditional vision systems with no differences in potential side effects.
Footnotes
Acknowledgment
The authors specially thank Eva Sequeira for her technical support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work has been funded by the Government of Extremadura (Spain) (GR18199, TA18023) (cofunded by European Regional Development Fund). The funders had no role in study design, data collection, interpretation and analysis, decision to publish, or preparation of the article.