
Abstract
Objectives:
To compare the efficacy, complications, and costs of percutaneous nephrolithotomy (PNL) and extracorporeal shock wave lithotripsy (SWL) in the treatment of a 20 to 30 mm single renal pelvic stone with a density ≤1000 HU.
Patients and Methods:
Eighty patients were prospectively randomized to receive either PNL or SWL during May 2017 to April 2019. The relevant demographic and clinical characteristics were compared.
Results:
The mean age in the PNL and SWL groups was 43.25 ± 15.16 and 44.18 ± 12.08 years, respectively. The mean stone sizes were 25.2 ± 3.9 and 24.6 ± 2.3 mm, respectively. The stone-free rate (SFR) was significantly different after the primary procedures (92.5% vs 37.5%, respectively; p < 0.04), but it was comparable after 3 months (97.5% vs 90%, respectively; p = 0.723), with a higher rate of auxiliary procedures after SWL (p = 0.017). On multivariate analysis, stone density was the only significant variable for the SFR in the SWL group (p = 0.004). Complications occurred in 27.5% and 22.5% of cases, respectively (p = 0.796). The mean costs of SWL (650.23 ± 424.74 United States Dollars [US$]) were significantly lower than those of PNL (1137.65 ± 224.43 US$; p < 0.0001).
Conclusions:
The SFRs for PNL and SWL were not significantly different after 3 months in the treatment of a 20 to 30 mm single renal pelvic stone with ≤1000 HU, although PNL provided a significantly higher rate after its primary procedure. SWL was significantly less costly, but it mandated a significantly higher number of auxiliary procedures than PNL.
Introduction
There are different approaches to the treatment of kidney stones, after significant advances in minimally invasive techniques. 1 –3 They include extracorporeal shockwave lithotripsy (SWL), percutaneous nephrolithotomy (PNL), retrograde intrarenal surgery, and laparoscopic pyelolithotomy. These are currently the favorite methods. 1,3 To provide the optimal treatment, however, there are variable predictors that should be considered, including factors related to the stone such as the size, number, density, and location; the kidney such as the pelvicalyceal spatial anatomy; the patient such as obesity; and the technique such as mechanism of disintegration. 3 Efficacy and safety of each individual modality are potentially prone to the effect of these predictors rendering the selection of the optimal treatment a clinical challenge. 4,5 This challenge revealed a progressively accumulating literature of comparative researches with variable combinations of SWL, PNL, and retrograde intrarenal surgery. 5,6 Despite the verified recommendations of the current guidelines in assignment of PNL and SWL for treatment of certain stone sizes, 1 the optimal approach to the treatment of intermediate-sized kidney stones is still controversial. 7 The optimal treatment should provide the highest stone-free rate (SFR) with the lowest rates of interventions and complications. 5,8 In this study, we prospectively compared the outcomes of PNL and SWL in the treatment of a 20 to 30 mm single renal pelvic stone with ≤1000 HU. This stone size was defined because it is the most controversial one in the current literature of the intermediate-sized kidney stones, despite the recommendations of the guidelines of treatment of kidney stones. 1 –8
Patients and Methods
In a prospective randomized clinical study, adult patients who presented to our hospital between May 2017 and April 2019 with a single renal pelvic stone were randomly assigned and treated by PNL or SWL. The sample size of 78 patients was calculated to provide a study power 80% (type II error 0.2), confidence level 95% (type I error 0.05), and threshold of significance of 0.05 using Epi Info™, version 3.5 software. Patients were assigned to the potential modality using a computer-generated randomization method (JMP, version 12.0.1; SAS Institute, Cary, NC). Two authors (R.A.G. and M.A.I.) were responsible to patient's assignment and its revealing to the operator at the day of operation.
The inclusion criteria included the adult patients who had a 20 to 30 mm single renal pelvic stone with a density of ≤1000 HU in noncontrast computed tomography (NCCT) scan. However, the exclusion criteria were refusal of the procedure, factors precluding candidacy for anesthesia or surgery including morbid obesity, skeletal malformations, uncontrolled urinary tract infections, poor ipsilateral or total renal functions, distal and/or contralateral ureteral obstructions, atypical bowel position relative to the kidney, and nonpelvic renal stone locations.
A full history of illness, physical examination, and surgical fitness work-ups were obtained. Laboratory investigations included urinalysis, renal function tests, bleeding profile, complete blood count, and random blood sugar level. All the patients had abdominal ultrasonography (US), kidney, ureter, and bladder radiograph (KUB), and NCCT. HU was measured in magnified bone windows and the mean of multiple small regions of interest using the largest two dimensions. The measurements were repeated for confirmation.
Surgical techniques, steps, and armamentarium of PNL and SWL procedures are outlined in Table 1. In PNL, if the day 1 postoperative KUB and US were free, nephrostomy tube and ureteral catheter were removed in the first and second postoperative days, respectively. If there was no fever, pain, or urine leakage, the patient was discharged in the third postoperative day. If there were residual fragments >4 mm, a second look PNL was performed at the same admission. In SWL, if there were residual stones >4 mm after 2 weeks, an auxiliary SWL session was performed, 2 to 3 weeks apart. NCCT was carried out after 3 months to confirm the stone-free status in all patients. In the cases of persistent renal colic, urinary leakage, and fever, it was also carried out at presentation. The auxiliary procedure was defined as any extra intervention of the same primary treatment modality or of a different modality, including ureteroscopy and Double-J ureteral stents for treatment of residual stones >4 mm or complications.
Summary of Percutaneous Nephrolithotomy and Extracorporeal Shockwave Lithotripsy Surgical Techniques and Armamentarium
NCCT was carried out before the duration of 3 months in some cases, due to arrangements of patients traveling or consultations to other irrelevant presentations.
KUB = kidney, ureter, and bladder radiograph; NCCT = noncontrast computed tomography; PNL = percutaneous nephrolithotomy; SWL = extracorporeal shockwave lithotripsy; US = ultrasonography.
The primary outcome measure was a stone-free status, defined as the absence of any detectable stone fragments at the end of the procedure by both US and fluoroscopy or detectable single or multiple residual fragments ≤4 mm (the most common value in the literature 1,2 ) by US or KUB during the direct postoperative day, before removal of the nephrostomy tube. Follow-up visits and imaging were scheduled to diagnose the stone-free status (Table 1).
Due to economic factors and uncertain benefit for treatment of the current stones, postoperative stone analysis was not a variable in the current study, but it was performed only in seven and three patients on their demand in the PNL and SWL groups, respectively.
The summation of costs included all the surgical procedures, medications, follow-up work-ups, fees of medical personnel, and the additional services and subsidiary costs such as traveling and emergency calls (Table 2). The values were converted from the Egyptian currency into a standard currency (Dollars of the United States [US$]). These values were calculated according to the current local prices and payment policies of health care services during the time of the study at our hospital, which is a governmental center.
Distribution and Summation of the Costs per Service in the Percutaneous Nephrolithotomy and Extracorporeal Shockwave Lithotripsy Groups
Costs of the primary and secondary procedures are provided as total packages, including the costs of the procedure and the perioperative services. For example, primary PNL costs (882 US$) could be empirically distributed into: operative room (220 US$), anesthesia (100 US$), disposables (220 US$), medical personnel fees (140 US$), hospital stay (80 US$), medications (100 US$), and admission and discharge files (22 US$). The other items of services are done outside these packages and are distributed as mentioned above considering the average costs. Considering that the main treatment could be achieved by the primary procedures and owing to the governmental health care policies, costs of primary PNL and SWL procedures are higher than the auxiliary ones.
Frequency of the service is not usually similar to the number of patients who received this service due to repeating of the service for auxiliary treatment, follow-up of stone clearance, or other nonscheduled medical, imaging, or laboratory tests such as hemoglobin levels. Also, the final summation of costs may be different from the outcome of frequency × patients' number due to differences such considering the auxiliary treatment by a different modality (PNL after SWL and vice versa) as a primary one in price.
CBC = complete blood count; NA = not applicable data; SD = standard deviation; URS = ureteroscopy; US$ = United States Dollars.
An informed written consent was taken from each patient. At the start, clinical trials registration was not a requirement to be approved by the Ethical Committee of Faculty of Medicine, Assiut University. Institutional review board number: IRB 17200414, 2016.
Statistical analysis
Recorded data were analyzed using the statistical package for social sciences, version 20.0 (SPSS, Inc., Chicago, IL). Quantitative data are expressed as mean ± standard deviation. Qualitative data are expressed as frequency and percentage. Between the PNL and SWL groups, continuous variables were compared using the Mann–Whitney U test. Categorical variables were compared using the Pearson chi-square/Fisher exact test. Multivariate logistic regression analysis was used to predict the outcome of categorical variables based on one or more predictor variables. The p-value <0.05 was considered statistically significant.
Results
Considering a proportion of lost to follow-up patients, 80 patients were randomized and completed the current study after exclusion of the ineligible patients (Fig. 1). Three patients refused SWL and two patients refused PNL. Forty patients were allocated to PNL, and the other 40 patients were allocated to SWL. The demographic and clinical characteristics of the patients and the characteristics of stones are demonstrated in Table 3.
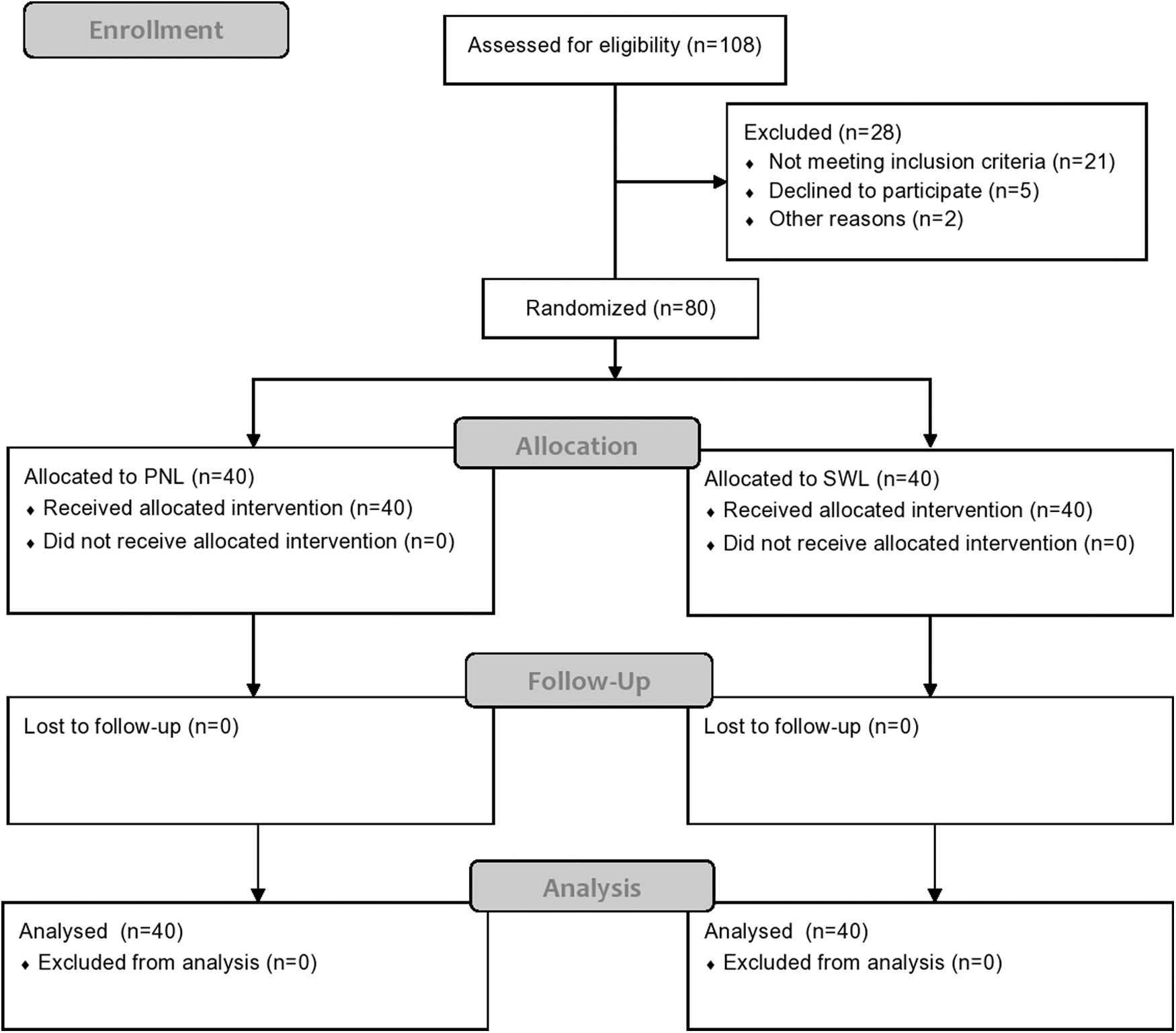
CONSORT flowchart of patients undergoing PNL or SWL. PNL = percutaneous nephrolithotomy; SWL = extracorporeal shockwave lithotripsy.
The Demographic and Clinical Characteristics of the Patients in Both Groups
BMI = body mass index; HU = Hounsfield unit; G = grade; SFR-1st = stone-free rate after the first session; SFR-3m = stone-free rate after 3 months.
Regarding the PNL procedure, the upper calix was the favorable access in 21 (52.5%) patients. A single puncture was required in 38 (95%) patients. The mean operative time was 79.88 ± 16.35 minutes. In both groups, procedures were carried out by different urologists, and despite the common practice of inserting preoperative stents for patients with larger stones before SWL, no preoperative stents were placed.
The final SFRs for the PNL and SWL groups were insignificantly different at 3 months (p = 0.723), despite the significantly higher rate after the primary PNL procedure than that after primary SWL session (p < 0.01) (Table 3). Significantly different numbers of auxiliary procedures (7.5% vs 62.5%, respectively; p = 0.017) resulted in these outcomes. In the PNL group, 37 patients (92.5%) rendered stone free by a single procedure, but the remaining 3 patients (7.5%) needed two procedures for each. Only one of them was further treated by an auxiliary SWL session. In the SWL group, 15 patients (37.5%) were cleared with the first session, 12 patients (30%) with two sessions, 5 patients (12.5%) with three sessions, and 4 patients (10%) with four sessions. However, four patients (10%) needed PNL after four SWL sessions to become free of stones.
No statistically significant relationship could be detected between the SFR and the proposed affecting factors by the multivariate analysis using the logistic regression, except the stone density, which was represented by HU (Table 4).
Logistic Regression of Factors Affecting the Stone-Free Rate Calculated at 3 Months After the Primary Procedure in Both Groups
CI = confidence interval; OR = odds ratio.
All complications were graded according to the modified Clavien–Dindo system (Table 3). Although the levels of grades in the PNL group were lower than those of the SWL group, the total frequency was insignificantly higher (p = 0.796). In the SWL group, four patients had hematuria, which was managed conservatively. Also, five patients had Steinstrasse and renal colic without fever; three of them were treated conservatively, whereas two of them were cleared by ureteroscopy with placement of Double-J stents. All the five patients were prescribed analgesics, alpha blockers, and antibiotics. In the PNL group, three patients had urinary leakage and other five patients developed fever of 38.2°C to 39°C; all were managed conservatively by observation, antibiotics, and antipyretics. Also, three patients developed hematuria and clots within the first postoperative week, and the hemoglobin level was reduced to 7.5 to 8.5 g/dL. They were treated conservatively including blood transfusion to all the three patients. All these complicated cases were unplanned emergency presentations. Angiography and embolization interventions were not indicated at all.
Regarding the costs (Tables 2 and 3), costs of the primary procedures and the total costs of PNL were higher than those of SWL. The mean of the total costs of PNL was significantly higher than those of SWL (p < 0.0001).
Follow-up duration was 3 months at least for all the patients in both groups. No recurrence or increased sizes of residual gravels was detected among the patients of both groups.
Discussion
Kidney stones are prevalent worldwide, and their treatment has markedly been shifted from the traditional open surgery to the minimally invasive modalities due to the technological advancements of endourology. 1,2,5,9,10 The demographic characteristics in PNL and SWL studies are usually similar. 2,10 Body mass index (BMI) could be a significant factor in characterization of the patients to the suitable treatment. 8,11 In the current study, the relatively low skin-to-stone distance could be attributed to the lower BMIs of our population than those of the Western populations. 11 The insignificant difference in its comparative effect on the SFR may refer to a favorable effect in both groups of the current study.
SWL and PNL are strongly recommended for kidney stones ≤10 mm and >20 mm, respectively. 1,2,12 Variable sizes of stones within the range of 10 to 30 mm have been studied under the terms of moderate-sized or intermediate-sized kidney stones including different stone locations. 5,8,13 –16 However, renal pelvic stones with a size of 20 to 30 mm have been targeted in a few comparative studies, which have not been confined to PNL and SWL. 4,6,8,17 –23 This stone size may represent a challenging zone between the moderate and large sizes, where the preference of SWL is inversely related to the stone burden. 2,12 Also, skin-to-stone distance and density are major factors affecting the outcomes of SWL. 3,12 In the current comparison of a 20 to 30 mm stone treatment, we had to compensate for the low favorability of SWL by limiting the stone density to ≤1000 HU.
US and KUB are inexpensive basic imaging that could be obtained for patients on their initial presentation and follow-up. While the former is a bedside complementary test to physical examination providing the basic descriptions including kidney site, size, and dimensions, the latter can only detect the radiopaque shadows. However, NCCT is the preferred modality for diagnosis and characterization of kidney stones to the suitable line of treatment and follow-up. It provides a confirmative description of the renal anatomy and stone characteristics. 24 HU measurement is currently the preferred NCCT-generated method to predict a stone composition and its response to treatment. 3,19 Despite the absent consensus, there is a common attitude that stones with <500 to 600 HU could be considered as radiolucent or friable stones. 20,25 However, stones with >1000 HU have been considered very hard and may not respond to SWL. Therefore, the HU value might crudely differentiate kidney stones into hard and not-hard ones when its value is >1000 and <1000 HU, respectively. 9,12,23 However, PNL is not significantly affected by stone composition. 5 In the current study, stone composition was unknown for all cases preoperatively. However, the predetermined ≤1000 HU as an inclusion criterion might provide a legitimation for enrollment of SWL in this comparison with PNL for treatment of this relatively large stone size. HU was the only variable that showed a significant correlation with the SFR in the SWL group. This finding was similar to the reported significant role of stone density as an independent predictor for the SFR after SWL in relation to the stone location. 26
The current SFR came in agreement with the previous studies that targeted similar renal pelvic stones. 8,13 The SFR after the primary procedures has variably been defined as either having no residual stone fragments at all or accepting residual fragments of 2 to 5 mm sizes. 5,18,27 Similarly, we employed the latter definition and considered only the residual fragments >4 mm for further treatment. However, SWL mandated a higher number of auxiliary procedures than PNL. Despite the inclusion of the extra sessions of SWL in the definition of the auxiliary procedures, the current results came in concordance with the literature. 2 However, it is still imperative to consider the issue of auxiliary treatment in patient's counseling to outweigh the risks and benefits of repeated sessions of SWL in many aspects, such as the disturbed work times with extra costs and frequent exposure to radiation. 20,28 The current SFR at 3 months was similar in both groups, despite its significantly higher value after the primary PNL. This outcome was similar to the results of Gadelmoula et al. who employed >1000 HU in treatment of similar moderate-sized stones. 13 It seemed that inclusion of stones with ≤1000 HU did not significantly affect the rate of auxiliary procedures after SWL.
Using the modified Clavien–Dindo classification, grades of complications of SWL were higher than those of PNL, but with insignificant lower total frequency. Inclusion of isolated fever after PNL in this classification could be concerned, but this issue could be alleviated by the high degree of fever similar to other studies. 29
SWL provides significantly lower costs than PNL. 8 This may be attributed to significantly lower proportion of inpatient admissions and visits of post-SWL emergencies compared with PNL. 30 Similarly, the current results showed higher costs of PNL than those of SWL. These relatively low costs could be partially attributed to the governmental support to the health care services.
Despite its similarity to other studies targeting 20 to 30 mm single renal pelvic stones, 8 the current study was prospective and randomized with a specified stone density ≤1000 HU. Its limitations may include a relatively small sample size and lack of generalizability of outcomes. Large multicenter studies are warranted to compensate for these limitations.
Conclusions
The SFRs for PNL and SWL were not significantly different after 3 months in the treatment of a 20 to 30 mm single renal pelvic stone with ≤1000 HU, although PNL provided a significantly higher rate after the primary procedures than that after SWL. However, SWL mandated a significantly higher number of auxiliary procedures (62.5%). Although PNL showed insignificantly higher frequency of complications than SWL, grades of complications after SWL were higher than those after PNL. However, SWL is a noninvasive outpatient procedure with significantly lower costs than PNL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.