
Abstract
Introduction:
Simulation-based training in laparoscopic urology is essential, as these surgeries require a skill set different from routine urologic procedures. We aim to describe and validate the chicken and porcine intestine model for laparoscopic neobladder reconstruction.
Materials and Methods:
Prospective observational study was conducted at our institute. Twenty novice and 20 trained laparoscopic surgeons were included in the study. The relevant chicken anatomy and surgical steps were described to all the surgeons. The surgeons were asked to fill a nine-point questionnaire after completing the exercise comprising bowel organization, ability to do urethroneovesical anastomosis, suturing time, suturing similarity, quality of suturing, tissue feel, integrity of anastomosis, realism, and usefulness of model after finishing the procedure, and score it on a scale of 1–5. Time taken to perform the entire exercise was noted in addition. An independent expert observer retrospectively rated the urethroneovesical anastomosis on a scale of 1–5.
Results:
All the participants in the study gave a mean score of 3.5 or more to all the questions asked in the questionnaire. Both the groups rated the usefulness of the model highly with a mean score of 4.6 and 4.45, respectively. The mean score of the questionnaire was 35.9 and 36, respectively, for both the groups. The quality of urethroneovesical anastomosis as observed by an expert was better in the expert group (p = 0.001).
Conclusion:
The chicken and porcine model for laparoscopic neobladder reconstruction is a useful and effective training tool. This model has face, content, and construct validity to be used as a teaching and training tool in laparoscopic urology.
Introduction
Simulation-based training in laparoscopic urology is essential, as these surgeries require a three-dimensional imagination of two-dimensional vision, and there is loss of haptic feedback. 1 Simulation in minimally invasive surgery (MIS) allows the learner to practice new motor skills in a safe and stress-free environment outside the operating room, thereby decreasing the learning curve.
There is a large body of evidence supporting the use of simulators in MIS; also, there have been many attempts to validate these simulators in different studies. 2,3 Various types of endotrainers, both inanimate and animal models, have been described with variable degree of validity. 1,4,5 Reconstructive laparoscopic surgeries in urology are progressively becoming more complex and these simulators are hence providing valuable practice for surgeons before performing these surgeries on patients. We described a chicken and porcine model for laparoscopic neobladder reconstruction after cystectomy and aimed to validate this model with face, content, and construct validity.
Materials and Methods
It was a prospective observational study conducted at Muljibhai Patel Urological Hospital, Nadiad, Gujarat, India. Twenty novice surgeons and 20 trained laparoscopic surgeons were included in the study. Trained laparoscopic surgeons were either fellowship trained or had an experience of doing 20 or more cases. Novice surgeons were surgeons who had experience of doing <5 cases or no experience of intracorporeal suturing or were routinely not assisting laparoscopic procedures. The relevant chicken anatomy and surgical steps were explained to all the surgeons. Surgeons were shown a prerecorded video of the simulation and were asked to do steps of the simulation. The surgeons were then asked to fill a nine-point questionnaire comprising bowel organization, ability to do urethroneovesical anastomosis, suturing time, suturing similarity, quality of suturing, tissue feel, integrity of anastomosis, realism and usefulness of model after finishing the procedure, and score it on a subjective scale of 1–5 (Table 1). Time taken to perform the entire exercise was noted in addition. An independent expert observer retrospectively rated the urethroneovesical anastomosis on a scale of 1–5. Six months after the completion of the study the participants were asked to grade the improvement in their skill and utility of the model in surgical training on a scale of 1–5.
Surgeons Assessment Proforma
The study was conducted as per the institutional animal ethics committee guidelines. A waiver was obtained from the ethics committee in view of small animal cadaver use.
The sample size was calculated using Minitab software, with the aim of comparing the total score of both the groups based on various parameters under study (α = 0.05, power = 0.80). Statistical analysis was done and the difference between both the groups was compared using SPSS software version 25.0. The level of significance was set 0.05 and independent t-test was used to test the significance between the total scores obtained by the two groups.
Model Construct
Relevant chicken anatomy explained to the participants
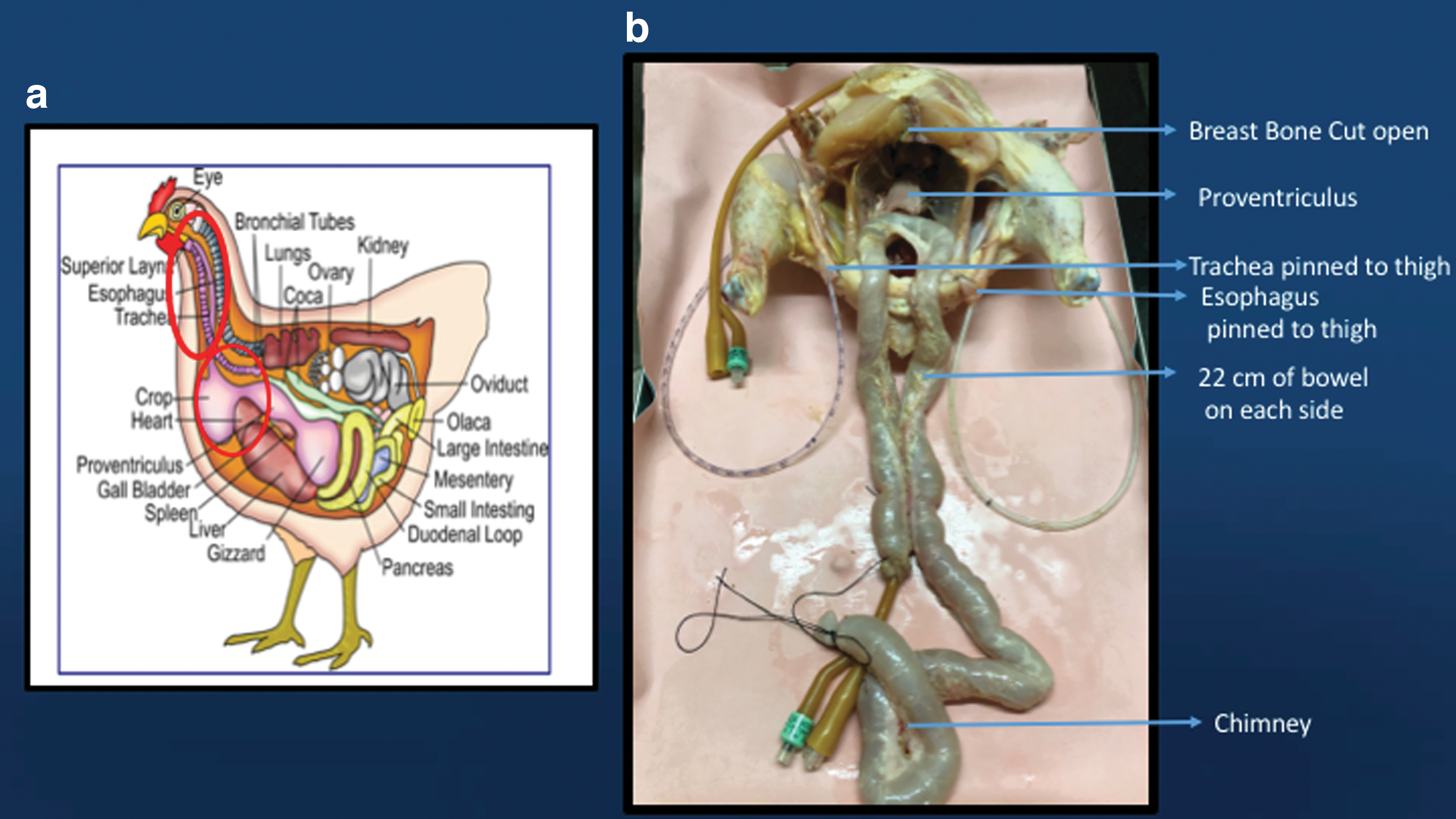
The chicken neck houses the esophagus and the trachea that lie on the vertebral column. The esophagus continues as crop, also known as the ingluvies, followed by proventriculus and gizzard (Fig. 1a). The crop, proventriculus, and the gizzard actually form the chicken stomach. The proventriculus is thick and muscular and can mimic the human urethra.
(
Setup
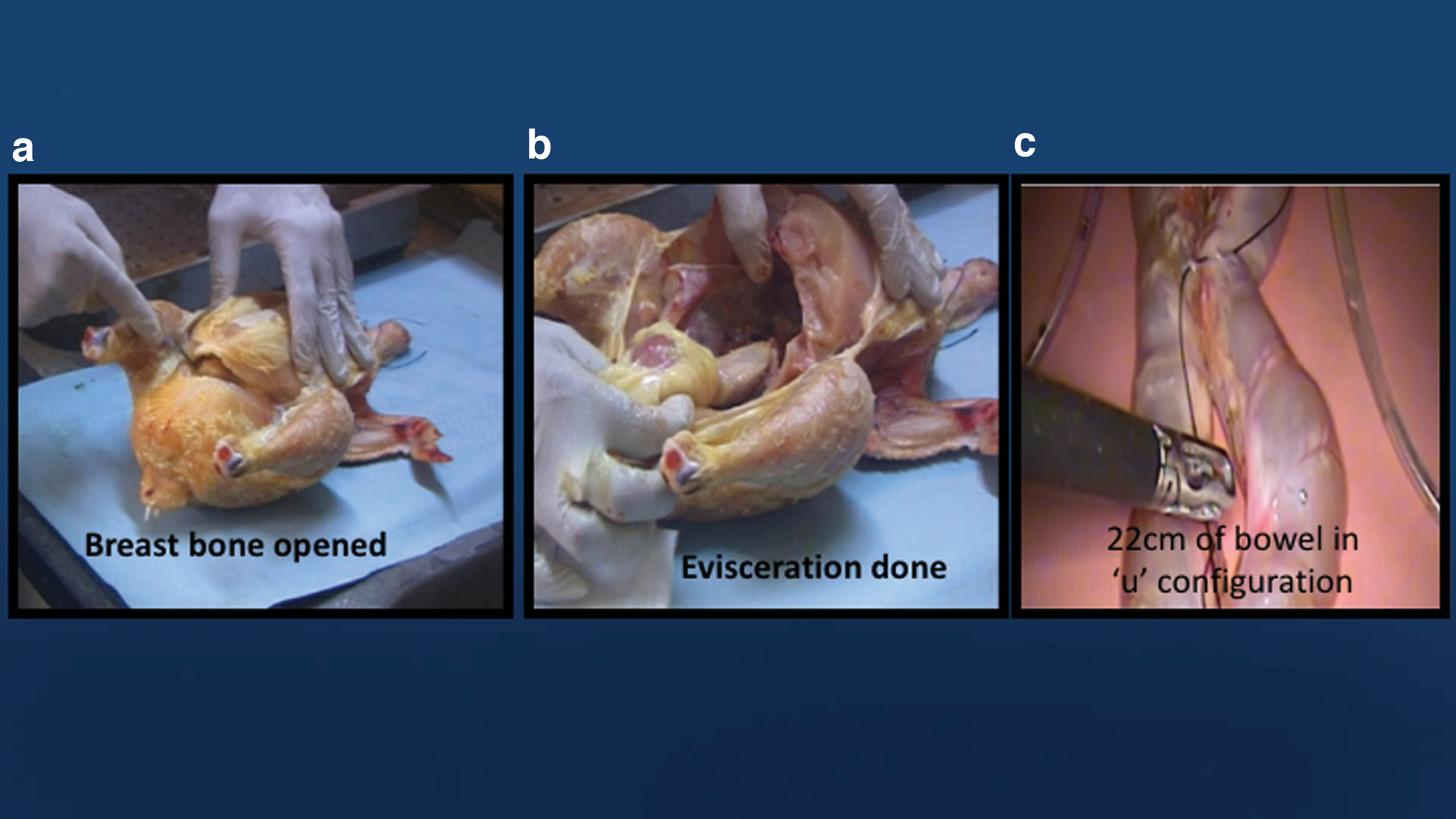
The chicken is culled, fur extracted, and beheaded. The esophagus and trachea are dissected and excised from the neck. The chicken is placed on its back with the leg end facing the operator and head end away from the operator (Fig. 1b). The chicken breast is open transversely (Fig. 2a) and chunk of chicken breast is excised to expose the viscera. The chicken is eviscerated leaving the proventriculus and gizzard intact (Fig. 2b). The junction of proventriculus and gizzard is transected. The cut end of proventriculus will mimic the urethra. The previously dissected and disconnected trachea and esophagus is mounted on the thighs of the chicken to mimic the right and left ureter (Fig. 1b). A 60 cm porcine intestine is used for reconstruction of the neobladder. The intestine is washed and tied at both the ends.
(
The neobladder was made out of 44 cm bowel, two limbs each of 22 cm were arranged in inverted “U”-shaped configuration (Fig. 2c). These limbs were detubularized and then cross folded to form a reservoir and 14 cm of chimney was used for ureteral anastomosis. The whole assembly was placed in the self-designed endotrainer.
Instruments used
Self-designed endotrainer
30° laparoscopes
Camera Single Chip Karl Storz™
Maryland forceps
Bowel holding forceps
Needle driver
3-0, 2-0 silk and Vicryl.
Self-designed endotrainer
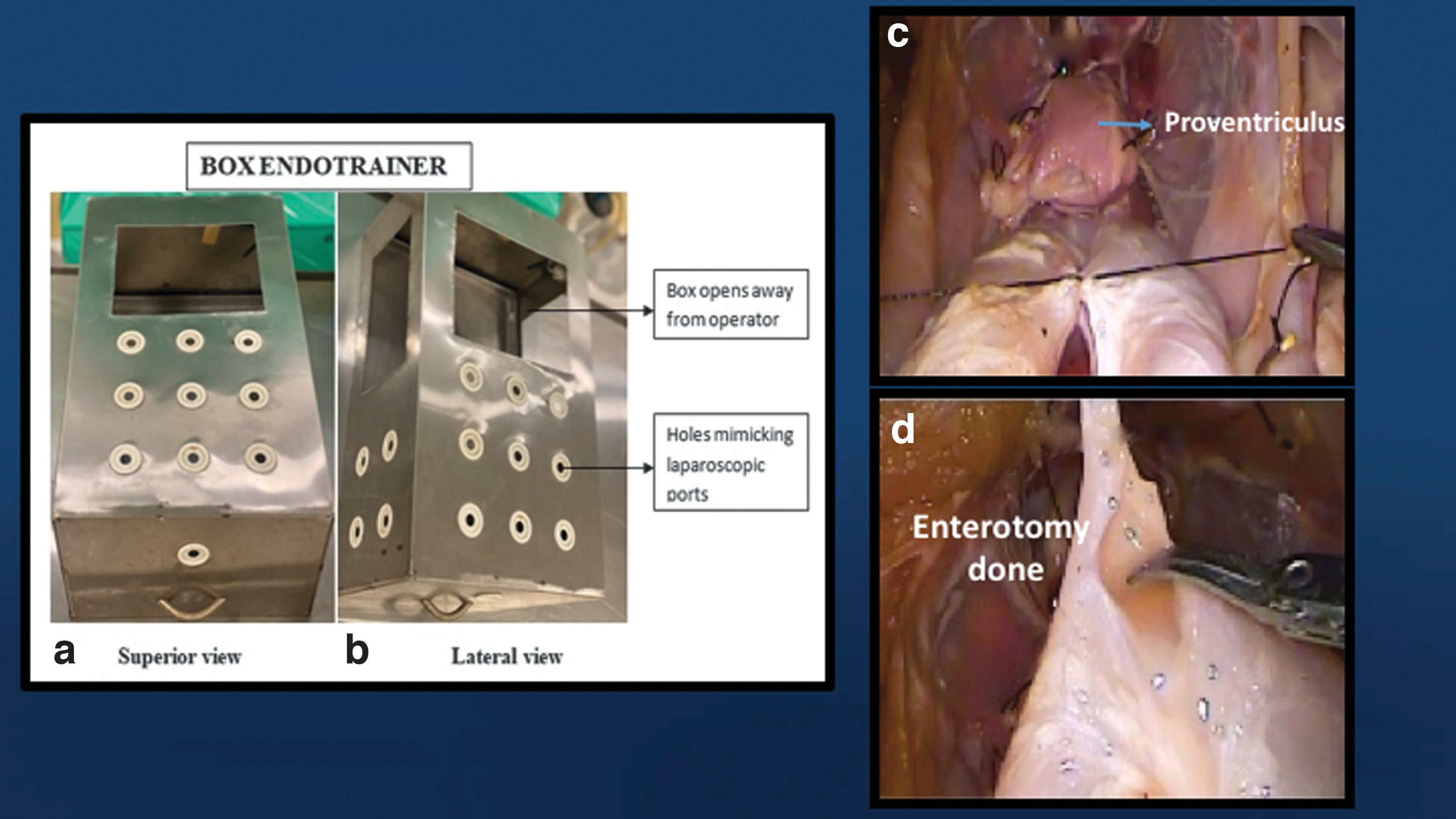
Cuboid-shaped container made out of steel sheets closed from all the sides apart from the base, the cuboid is kept on the steel tray on which the assembly is kept. Dimension of the box are 0.5 × 0.3 × 0.2 meters. Multiple holes are symmetrically carved out on the superior and the lateral surfaces as well as the surface that is facing the surgeon. The surface facing the operator has a central aperture for the laparoscopic telescope to be passed. All the holes are covered with caps of the ionic contrast bottle that are cut out in the center so that instruments can pass through it (Fig. 3a, b).
(
Steps of simulation procedure as explained to the participants
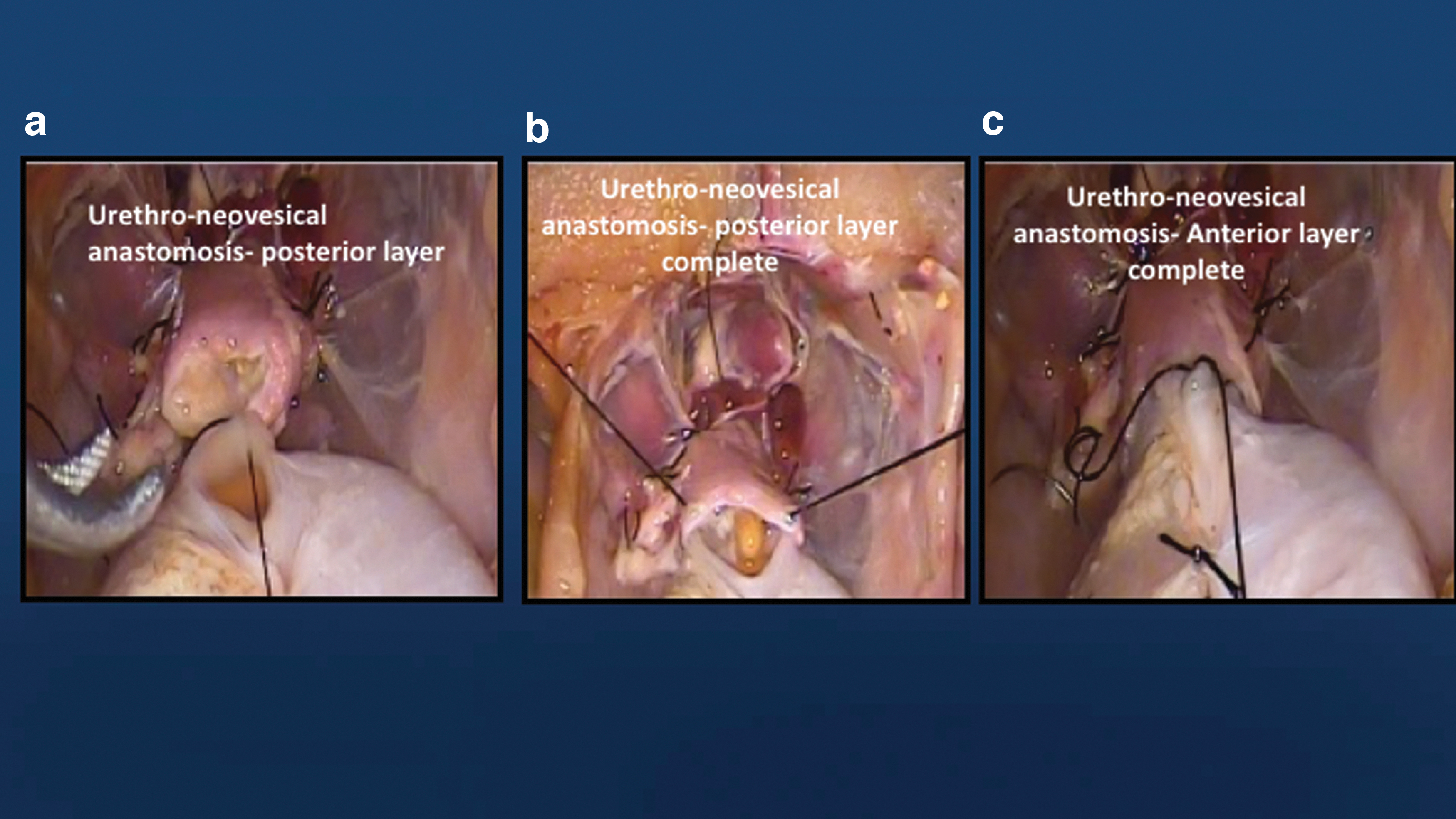
Surgical steps to be followed are explained as follows: Participants were asked to orient the porcine bowel in an inverted “U” configuration with the bend of the “U” facing the proventriculus. Each limb was measured 22 cm and kept adjacent to each other. Rest of the bowel was left as a chimney on one side of the operator (preferably left) (Fig. 2c). The two limbs of the inverted “U” were approximated to each other, by tacking interrupted stitches close to the mesentery, with silk 3-0 and without opening the bowel (Fig. 3c). A small button hole enterotomy was made at the most dependent part of the bend of the inverted “U” loop of bowel. This was the site for the urethroneovesical anastomosis (Fig. 3d). Button hole enterotomy of porcine bowel loop was anastomosed with cut end of proventriculus of chicken that mimics the urethra. This was to be done with a bidirectional suture, made by tying two 15 cm 3-0 silk threads with needle (Fig. 4a). ( The anastomosis was started in the center on the posterior wall at 6 O' clock position. After completion of the posterior wall, a Foley's catheter is passed across the anastomosis. The Foley's catheter is introduced through the crop of the chicken into the proventriculus and subsequently into the porcine bowel mimicking the urethroneovesical anastomosis. Posterior followed by anterior layer of anastomosis is done over the Foley catheter (Fig. 4b, c) The entire intestine that is in the inverted “U” configuration is tubularized and it is done close to the mesenteric border (Fig. 5a). ( Posterior wall of the tubularized bowel is sutured together to form the bladder plate. The bladder plate is now cross folded. The left distal end meets the right proximal end. Complete approximation of cut edges of bowel achieved (Fig. 5b–d) Folding of bowel on itself to create neobladder and approximation is achieved with silk 3-0 suture (Fig. 6a, b). ( Remaining 16 cm of the porcine intestine is identified. Trachea and esophagus of chicken that were anchored to chicken thigh were anastomosed with the porcine intestine in an end to side manner. An infant feeding tube is passed through the anastomosis. This completes the procedure (Fig. 6c).


Results
A total of 40 participants, 20 novice surgeons, and 20 trained surgeons (experts) participated in the study.
All the participants in the study gave a mean score of 3.5 or more to all the questions asked in the study. Both the groups in the study had comparable mean scores to all the questions asked in the study (p-value not significant). Both the groups rated the usefulness of the model highly with a mean score of 4.6 and 4.45, respectively (Table 2). The mean time taken by the novice and expert to complete the exercise was 140.15 ± 11.39 and 135.80 ± 12.23 minutes, respectively (p = 0.252). The mean rating given by expert observer to the quality of urethroneovesical anastomosis done by novice and expert was 3.3 ± 0.57 and 4.0 ± 0.64 (p = 0.001), respectively (Table 3).
Scores Given by Both the Groups to Each Parameter
Table highlights face and content validity of the model.
p-Values were seen to be insignificant.
SD = standard deviation.
Additional Values of Variables
p-Values were significant.
The face validity of the model was evaluated by the surgeons of the novice group and all the participants believed that the model had excellent usefulness as compared with real-life scenario. Also, 85% of the participants felt that the model was realistic and suturing was similar to the real situation.
The answers of the expert group showed that the model had content validity and agreed that it was useful in the training of laparoscopic neobladder surgery (Supplementary Fig. S1). The subjective suturing time score for the expert group was less than the novice but not statistically significant.
The novice and experts rated the mean improvement in skill and utility in surgical training as 4.0 ± 0.64 and 3.85 ± 0.74, respectively (p = 0.501) (Table 3).
Discussion
Surgical training consists of developing cognitive, clinical, and technical skills, the latter being traditionally acquired through mentoring. 6 Time and resources are essential components that restrict mentoring in current day and age, and trainees have to look at other options to acquire the necessary skills for performing the procedures independently. Simulation can be described as an exercise that reproduces or emulates, under artificial conditions, components of surgical procedures that are likely to occur under normal circumstances. 7 Simulators provide the trainees with both “Education” as well as “Training.” Education usually refers to the communication or acquisition of knowledge or information, whereas training refers to the acquisition of skills (cognitive or psychomotor). 8 Simulation provides the trainees with an opportunity to practice on inanimate objects in a stress-free environment, and later to be able to transfer these skills to the operating room on patients. This also reduces the financial burden along with the time taken up in training directly in the operating room. 9
MIS has now become a common place in most of the institutes and everything that could be done open surgically is now being replicated laparoscopically/robotically. As the complexity of the procedure increases, so does the learning curve. Because stakes are high in more complex procedures the learning curve further slows down.
At present, the mainstay of curative treatment for muscle invasive bladder cancer remains radical surgery with urinary diversion. Urinary diversion may either be in the form of ileal conduit or reconstruction in the form of neobladder. Urinary diversion is a complex part of the surgery and has traditionally been done through the open technique (extracorporeally in ileal conduit). However, with the advent of MIS, it was shown that this could also be done laparoscopically, first in porcine model 10 and then in humans. 11 With the introduction of robotic surgery into the fray, these complex surgeries have become replicable and can be done in lesser time with smaller incisions, thereby reducing the perioperative morbidity. Tyritzis and colleagues showed that the oncologic, functional, and complication outcomes of robot-assisted radical cystectomy with totally intracorporeal ileal neobladder were similar to open radical cystectomy series. 12 Desai and colleagues also found the surgery feasible with comparable complication rates in their series of 132 patients. 13
We intended to provide a novel model for simulation of laparoscopic neobladder construction after cystectomy. The model takes about 20 minutes to assemble and exercise takes about 2 hours to complete. This is a complex and advanced laparoscopic surgery and hence requires practice before performing it in a patient, to reduce the complications and perioperative morbidity. We used a mixed chicken and porcine model, which was oriented in such a way that it resembles the human pelvis. The cut end of the proventriculus of the chicken was anastomosed to the enterotomy made in the porcine bowel loop to resemble the urethroneovesical anastomosis done in neobladder construction. This was similar to the model for urethrovesical anastomosis proposed by Laguna and Mochtar where they anastomosed the esophagus and stomach. 2 The remaining part of the neobladder construction was done using porcine bowel loops.
This model can be replicated into a robotic milieu. However, we could not do it in our study for the want of the resources. This model is a novel model not described elsewhere in literature and is extremely useful for surgeons who want to start doing intracorporeal neobladder construction. Performing the steps as described will help to develop a greater understanding of the anatomy during the surgery and reduce the operative time of the actual procedure. The time taken to complete the simulation by novice in our study was more than the expert but not statistically significant (p = 0.252). The independent expert retrospectively observed the urethroneovesical anastomosis videos and rated the quality of anastomosis to be superior in the expert group (p = 0.001), hence proving the construct validity of the model. Both novice and expert reported an improvement of skill after using this model. In this study, we validated the face, content, and construct validity of the aforementioned model.
Limitations of the study
We could not prove concurrent validity or predictive validity in the model. However, usefulness of the model was proven by both the novices as well as experts. All the questions were self-reported. Questions such as suturing time and quality of suturing were not reported by a separate observer. Also, we could not demonstrate a statistically significant difference in suturing time of expert and novice.
Conclusion
The chicken and porcine model for laparoscopic neobladder reconstruction is a novel and useful model. It has face, content, and construct validity to be used as learning and teaching tool in advanced laparoscopic urologic surgeries.
Footnotes
Acknowledgment
We acknowledge contribution of Dr. Ankit Pal, chief veterinary surgeon at Jayramdas Patel Academic Center, Wet Lab, toward development of this model.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.