
Abstract
Introduction:
Bladder outflow obstruction (BOO) surgery is among the most commonly performed urologic procedures. Postoperative assessment consists of physical measurement of uroflowmetry and post-void residual volume, but health systems worldwide have experienced pressures in demand, leading to exploration of greater efficiency in organizing clinic protocols. International Prostate Symptom Score (IPSS) questionnaire measurement has been identified as a tool to predict change in postoperative management. Our institution established a nurse-led follow-up virtual clinic (VC) for patients undergoing BOO surgery based on IPSS measurement. We present the clinical and economic outcomes of this new service.
Materials and Methods:
Patients with a successful postoperative trial without catheter were contacted by telephone via VC and discharged by a Urology Clinical Nurse Specialist (UCNS) if IPSS was <8. Data were analyzed for IPSS, arrangement of subsequent clinic visits, and numbers discharged. Primary outcome was the proportion of patients discharged after VC consultation. Secondary outcomes were overall discharge rate following subsequent face-to-face (FTF) appointment; and the proportion of patients re-referred from Primary Care within 3 months of discharge from VC. Cost savings were calculated based on tariffs of £135 for first attendance with UCNS, £199 for uroflowmetry, and £47.84 for VC appointment.
Results:
The first 50 patients to be recipients of the new VC were included. The median IPSS and quality-of-life score were 13 (interquartile range [IQR] 5) and 3 (IQR 1), respectively. Thirty-nine (78%) patients were discharged from VC; 36 (72%) had IPSS <8. Overall discharge rate following subsequent FTF appointment was 88%. Two patients discharged from VC (5.1%) were subsequently re-referred, neither of whom required additional treatment. Total cost savings with VC amounted to £10,634.
Conclusion:
Telephone follow-up for BOO surgery based on IPSS is clinically safe and cost-effective, providing greater efficiency for clinic protocols.
Introduction
Surgery for male bladder outflow obstruction (BOO), often secondary to benign prostatic enlargement (BPE), is one of the most common indications for urologic surgery, with more than 84,000 such procedures carried out in the National Health Service (NHS) in England during 2018 to 2019. 1 Such operative measures are considered for men with lower urinary tract symptoms (LUTS) causing significant bother or impact on quality of life (QoL), or which are refractory to medical treatment, or who may have gone into urinary retention requiring catheterization and desire to be catheter-free.
Current European Association of Urology (EAU) guidelines on postoperative assessment of patients who have undergone BOO surgery recommend review at 4 to 6 weeks after trial without catheter (TWOC) to evaluate treatment response and adverse events, with measurement of International Prostate Symptom Score (IPSS), uroflowmetry, and post-void residual (PVR) bladder volume. 2 However, health care systems worldwide are experiencing pressures in demand, leading to exploration of streamlined follow-up protocols and establishment of virtual services. Such uses of telemedicine have already been implemented in Urology, for example, with prisoner populations, 3 although its use within the specialty globally has been sparing. 4
Our institution, in looking to introduce greater efficiency into our own clinic protocols, identified IPSS measurement as a tool to predict change in management at postoperative assessment of BOO surgery patients, 5 and in response, we set up a new virtual service for more resourceful assessment of such patients. The aims of this study were to calculate the cost savings made from this new provision and to assess its clinical safety based on clinical outcomes determined by IPSS, discharge rates, and re-referral rates.
Materials and Methods
This was a single-site multiple surgeon study, which was registered locally with the Trust Clinical Audit Department (reference number UHDB239a, Queen's Hospital Burton site). This study was conducted as part of a Service Evaluation project and therefore did not require Research Ethics Committee approval as per the guidance outlined by the NHS Health Research Authority. The BOO surgery procedures offered by our department are transurethral resection of the prostate (TURP) and bladder neck incision (BNI). We established a nurse-led follow-up virtual clinic (VC) based on IPSS measurement for patients who had undergone BOO surgery, whereas before the service had consisted of a face-to-face (FTF) appointment with a Urology Clinical Nurse Specialist (UCNS) measuring uroflowmetry and PVR. Patients were allocated an appointment date and time ∼3 months after their surgery as specified in operation notes forwarded to the administrative team and were contacted by a UCNS (members of our existing staff) via telephone provided they had a successful postoperative TWOC (patients who had an unsuccessful second postoperative TWOC were automatically scheduled an FTF appointment with a Urology doctor and therefore excluded from any final analysis). IPSS questionnaire was read out to them over the telephone, with the IPSS and QoL score calculated from patients' responses. Patients were discharged back to Primary Care by the UCNS if their IPSS was <8 (mildly symptomatic according to the questionnaire). Subsequent FTF outpatient consultation with a Urology doctor was arranged by the UCNS if the IPSS was 8 or greater, or at patients' own requests regardless of IPSS.
Data were collected prospectively on preoperative (patient age; indication for surgery; flexible cystoscopy and findings; urodynamic studies and findings; presence of indwelling urinary catheters or performance of intermittent self-catheterization); intraoperative (primary BOO procedure performed, along with additional procedures carried out at the same time; estimated prostate size; grade of primary surgeon; duration of surgery); and postoperative variables (timing of successful postoperative TWOC). Further data were then collected from VC appointments, including IPSS and QoL scores with median scores and interquartile range (IQR) calculated, outcome from VC, subsequent management if not discharged from VC, and re-referral from Primary Care within 3 months of discharge from VC. Cost savings were calculated based on the NHS tariffs provided by the local Finance Department of £135 for FTF appointment with UCNS or doctor, £199 for uroflowmetry and PVR measurement, and £47.84 for VC appointment. 6
Primary outcome was the proportion of patients discharged after VC consultation. Secondary outcomes were the overall discharge rate of all patients following subsequent FTF outpatient visit arranged from VC; and the proportion of patients re-referred to our department from Primary Care within 3 months of discharge from VC.
Results
The first 50 patients to be recipients of the new VC were included, over a period of 10 months from September 2018 to August 2019; their preoperative demographics are shown in Table 1, including preoperative investigations and findings. Urinary retention (both acute and chronic; all patients had an indwelling urinary catheter) and LUTS with failed medical therapy (patients had been managed with both an alpha-blocker and 5-alpha-reductase inhibitor, or either one of these but unwilling to continue further medical therapy and instead expressing an active choice to pursue surgery, with the decision to operate made after thorough counseling) were the most common indications for surgery. Table 2 demonstrates the intraoperative and postoperative characteristics. Forty-nine patients underwent TURP and 1 had BNI. Forty-five (90%) patients operated on had either a medium or a large prostate. Six patients had an additional procedure performed at the same time as their BOO surgery. The primary surgeon in 26 (52%) cases was a consultant, but all procedures with a registrar or resident-level doctor as the operating surgeon were supervised by a consultant present in the operating theater. The greatest distribution of operative time was between 30 and 90 minutes (40 patients, 80%). Thirty-three (66%) patients had a successful first postoperative TWOC.
Patient Demographics and Preoperative Characteristics
BOO = bladder outflow obstruction; IQR = interquartile range; LUTS = lower urinary tract symptoms.
Intraoperative and Postoperative Characteristics
TWOC = trial without catheter.
The median IPSS from VC was 13 (IQR 5) and QoL score was 3 (IQR 1). Figure 1 demonstrates the outcomes from VC. All patients had their VC appointments arranged within 4 months of their surgery; 36 (72%) patients were discharged to Primary Care immediately after VC consultation based on IPSS of <8; 3 patients scored IPSS >8 but desired no further follow-up, with their QoL scores no >3. The remainder had a further FTF outpatient appointment arranged; five of these were subsequently discharged after this review, leading to an overall discharge rate of 88%. Two patients were kept under active surveillance for incidentally discovered prostate cancer from the TURP histology (both had IPSS of <8 at VC), and only one patient required further surgery in the form of optical urethrotomy for iatrogenic urethral stricture. Interestingly, there was a greater rate of discharge from VC in the group of patients who had a successful second TWOC (15/17, 88.2%) compared with those whose first TWOC was successful (24/33, 72.7%) this is demonstrated in Figure 2. We hypothesize that this may have been due to the prolonged catheterization time allowing longer healing time of the prostatic bed, although the exact reason is unknown.

Outcomes of VC and FTF appointments (percentages refer to proportion within the entire cohort of 50 patients). FTF = face-to-face; VC = virtual clinic.
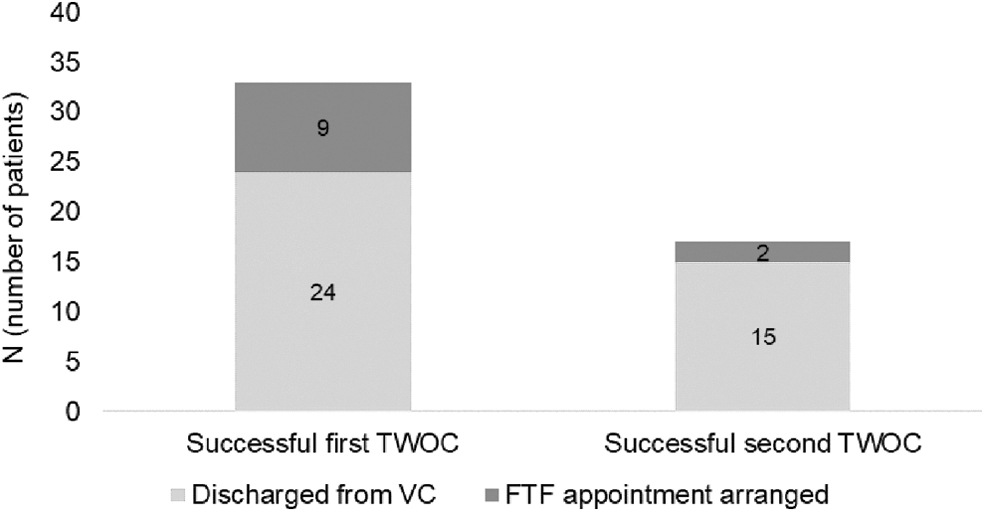
VC outcomes according to the timing of successful TWOC. TWOC = trial without catheter.
Of the 39 patients discharged straight from VC, 2 (5.1%) patients were re-referred from Primary Care within 3 months of discharge, but with probable Clavien–Dindo grade I complications in the form of hematuria and urinary tract infection rather than LUTS. One further patient with a history of dementia was “self-referred” by their carer to the department for LUTS.
Under the previous system of follow-up through FTF appointments, the total cost incurred for all 50 patients would have been £16,700. With VC, the total tariff for all 50 telephone consultations was £2392. Additional costs for uroflowmetry and FTF appointment were incurred through the 11 patients not immediately discharged, amounting to £3674, and a total of £6066 for the new service. Total cost savings to the health economy via VC were therefore calculated at £10,634 for the 10-month period.
Discussion
The use of VCs has become topical in light of the global coronavirus disease 2019 (COVID-19) pandemic, 7 necessitating many hospital Trusts within the NHS to undergo significant logistical reorganization. 8 One such measure to reduce FTF contact between clinicians and patients to reduce the risk of disease transmission has been to convert traditional outpatient appointments into telephone consultations, 9 particularly for maintaining movement within important patient pathways such as cancer, 10 and this has been seen by some authors as an opportunity to implement virtual consultations more widely, given the moves taken by many Trusts. 11 The initial results and longer term outcomes of these altered services across all hospital specialties have yet to be fully evaluated, but many new and follow-up clinics in the United Kingdom have switched to the virtual form, initially consisting of telephone consultations due to availability of technology.
VCs in Urology have been established in a wide variety of its subspecialties, including stones, 12 pediatrics, and even hematuria referrals. 13,14 Its use in LUTS has been limited to new referrals for urinary incontinence, where cost-effectiveness was not present due to re-attendances. 15 However, good patient satisfaction scores have been demonstrated elsewhere, 16 and the financial benefit has been proven by other Urology service providers. 17 Even a positive environmental impact has been calculated with such clinics through the saving of patient journeys to appointments, thus reducing both the individual and collective carbon footprint. 12,16 For our cohort, whose median age was 71.5 years, the absence of a journey to hospital saved them money they would otherwise have paid for public transport or car parking charges, and such an individual patient benefit cannot be overlooked especially in a more elderly population. It is also worth examining how VC adheres to the NHS “Getting It Right First Time” (GIRFT) recommendations, 18 specifically on “optimising urology outpatient services”: it makes smart use of the available services, provides quick answers, and agrees next steps including closure of the care episode. It is hoped VC will take a more prominent role in the next iteration of the GIRFT report, especially once the consequences of those regularly run during the COVID-19 pandemic are known.
The results from our new VC provide a good example of how patient-reported outcome measures (PROMs) can be used to have a direct impact on patient management. 19 IPSS has been long used as a PROM in the assessment of LUTS to determine symptom severity, and such stratification is recommended in the National Institute for Health and Care Excellence (NICE) guidelines not only to determine whether patients should be offered medical or surgical treatment but also response to treatment. 20 The latter use has been particularly true of IPSS in many well-known urologic trials, for example, Combination of Avodart and Tamsulosin (CombAT) in assessing combination medical therapy, 21 and MedLift in assessing surgical treatment for BPE. 22 PROMs are also used widely in other urologic subspecialties to evaluate erectile function and incontinence, 23,24 which are urologic symptoms that relate to QoL. However, it seems globally in medicine that PROMs have had a lack of impact on clinical decision-making due to both patient and clinician factors. 25 The discharge criteria for our VC are based entirely on the values received from the PROM used, and patients were discharged not only because of their IPSS but also because of the QoL score. The use of the latter is a greater vindication of the influence this PROM had on the final clinical decision-making, particularly because in our cohort, three patients were discharged directly from VC where their IPSS was >8, yet QoL score demonstrated no clear dissatisfaction with the way their urinary symptoms were.
There were limitations in the evaluation of this new service. We did not quantify patient satisfaction with the service itself, given the time-limited nature of the VC appointments, but did not receive any patient complaints about its virtual nature. Using only IPSS to determine future management focused purely on outcomes related to LUTS and did not take into account non-LUTS adverse events; the inclusion of other validated questionnaires such as the International Index of Erectile Function, 23 and one assessing continence, 26 would have identified further QoL outcomes, and this is an aspect we will look to incorporate in future VCs. We did not exclude patients with dementia from the VC (only one patient in the cohort had a background of this), with the intention that their carers would answer the IPSS on their behalf over the phone. However, this patient was referred back to our service by their carer and in hindsight, given the inability to answer the IPSS, this group of patients probably should have been excluded from the start. This cohort of patients was not compared with a previous cohort who would have been followed up under the prior system; this may have provided useful information regarding follow-up ratios, but the aim of this study was achieved in terms of assessing clinical safety and cost-effectiveness of the new VC.
To the best of our knowledge, this is the first reported example in the literature of VC being used to follow up BOO surgery, and other urologists may question the absence of uroflowmetry and PVR in assessing postoperative success of BOO surgery and the need for a change in management; EAU guidelines, however, acknowledge that its recommendations on BOO surgery follow-up are based on level 4 evidence. Furthermore, our department established the VC as we identified IPSS as a strong predictor of changes in patient management and, potentially, providing greater promise to deliver a more efficient service. 5 IPSS takes 15 minutes to complete, with clear discharge criteria set. Logistically, it removes the potentially long wait for the patient to void urine to measure uroflowmetry and PVR, the former investigation in itself then possibly providing inadequate results as patients may neither attend with a full bladder nor void a sufficient volume that can be accurately interpreted. We do realize that it is unlikely this approach will be utilized for more recent means of BOO surgery developed as an alternative to TURP, such as holmium laser enucleation of the prostate (HoLEP), prostatic urethral lift (UroLift®), and transurethral water vapor therapy (Rezum), as these newer technologies still require rigorous objective follow-up data to prove their long-term efficacy. However, once the outcomes of these are established, we recommend that VC follow-up become the model to adopt.
Our results also add further evidence in favor of the operative success of TURP, still considered as the historical “gold standard” operation for BOO surgery, with more than 11,000 carried out in England from 2018 to 2019. 1 HoLEP, for example, has been demonstrated to have a lower transfusion rate, reduced length of stay, and better postoperative IPSS and maximum flow rate compared with TURP. 27,28 Newer technologies such as UroLift and Rezum have been widely taken up because they are seen as even more minimally invasive procedures, again offering good outcomes in terms of complications. 29,30 However, we were satisfied with the proportion of patients who were immediately discharged following VC consultation; there are still many Urology departments offering only TURP as surgery for BOO, and until the newer procedures are incorporated into these departments' services, they should still feel confident in the outcomes TURP will offer.
Conclusions
VC follow-up for BOO surgery is clinically safe and cost-effective. It streamlines clinic protocols, adds greater efficiency, and adds further evidence to widened use of VC in Urology, especially at a time when significant pressures on health care systems are being felt worldwide.
Footnotes
Acknowledgments
We wish to acknowledge Kayleigh Ablewhite and Ceinwen Simpson, Urology Clinical Nurse Specialists in our institution, who ran the new virtual clinic and without whose hard work it would not have succeeded. We have adhered to the principles outlined in the Declaration of Helsinki.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.