
Abstract
Objectives:
To clarify the natural history of asymptomatic renal stones ≤5 mm in comparison with stones ≥5 mm. Calculi ≤5 mm are considered insignificant stones, but to what extent stone-related events can occur is unclear.
Patients and Methods:
In this retrospective study, 207 patients with asymptomatic renal stones confirmed by both CT and ultrasonography performed on the same day were enrolled. A follow-up ultrasound was performed every 6 months. The active indications for surgical intervention included stone relocations into the ureter and stone-related symptoms. The primary endpoint was the rate of surgical intervention.
Results:
A total of 207 patients (71 cases with stones ≤5 mm and 136 cases with stones >5 mm) were included in this study. At a median follow-up of 3.3 years, 14 patients (20%) from the ≤5-mm group and 52 (38%) from the >5-mm group underwent surgical treatment (p = 0.0067). Moreover, 11 patients (16%) from the ≤5-mm group and 27 (20%) from the >5-mm group received surgical intervention as they manifested active indications, showing no significant difference (p = 0.44). As regards stone events, there were no significant differences in spontaneous stone passage, pain, hematuria, and stone growth. Multivariate analysis revealed that age ≤50 years and a history of stone surgery were significant factors, but stone size was not.
Conclusion:
About 20% of asymptomatic renal stones ≤5 mm require surgical treatment within 5 years.
Introduction
Urolithiasis is one of the most prevalent and recurrent urologic diseases of the modern era. 1,2 The prevalence of urolithiasis has been estimated to be at 3%–7.1% in females and 8%–19% in males. 3,4 Hence, the economical and clinical burden of urolithiasis on the health care system are of great concern.
With advances in imaging technology, the possibility of detecting asymptomatic renal stone has been increasing. 5,6 Treatment options for renal stones include active surveillance, extracorporeal shockwave lithotripsy (SWL), ureteroscopy, and percutaneous nephrolithotomy (PCNL). However, the treatment strategy for asymptomatic renal stones remains to be established. There was little evidence on the clinical course of asymptomatic renal stones, but several recent studies have reported the natural history of asymptomatic renal stone patients who had undergone active surveillance. 5,7 However, these studies had limitations, including small sample size, short follow-up period, and inconsistency of imaging modalities. In particular, the data about the natural history of calculi ≤5 mm are very limited.
In several guidelines, calculi ≤5 mm have been considered as insignificant stones, but it was not clear as to what extent stone-related events can occur and surgical intervention be performed in these small stones. 8,9 From a technical viewpoint, the detection of renal stone ≤5 mm is often difficult without the use of noncontrast CT (NCCT). 2,9,10 In this regard, imaging modalities used in analyzing the natural history of asymptomatic renal stones in previous studies were inadequate for the detection and follow-up of renal stones ≤5 mm.
To clarify the natural history of asymptomatic renal stones ≤5 mm, this study investigated the natural history of cases in which asymptomatic renal stones were confirmed by both NCCT and ultrasound (US) and followed up continuously by US.
Patients and Methods
This study was approved by the Institutional Review Board of Ijinkai Takeda General Hospital. The inclusion criteria for this study were patients with renal stones detected by both NCCT and US imaging performed on the same day who had undergone active surveillance for asymptomatic renal stones from January 2010 to September 2014. 10,11 Although new patients routinely received US for the screening of urinary tract at our institution, we also performed NCCT for patients with acute flank pain and suspected urolithiasis to get information such as mean stone density and skin-to-stone distance. As a result, the majority of patients with suspected urolithiasis received both NCCT and US on the same day. 10,11 As previously described, all US examinations at our institution were performed by 7 experienced sonographers who are specialized in handling urologic US. 10,11 When a stone depicted by both US and NCCT was in the same kidney, the patients were enrolled in this study. Data of patients who were not treated for urolithiasis within 3 months after diagnosis and were followed up for more than 3 months were retrospectively extracted. The exclusion criteria were concurrent ureteral stones, solitary kidney, staghorn calculi, and urinary diversion. This study included patients with a new diagnosis of asymptomatic renal stones and patients who were already on active surveillance and on follow-up where data were collected only for the set study period.
Follow-up US was conducted on the patients every 6 months in an outpatient clinic. Indications for aggressive treatment included stone relocation into the ureter with or without pain, urinary tract infection with emergency drainage, and stone-related pain with no evidence of stone relocation (active treatment indication). However, surgical intervention was performed for calculi that increased in size by more than or <50% or at the patient's request (nonactive treatment indication). The surgical intervention was considered an event, at which point data were censored.
Clinical data such as age, sex, stone location (upper calix, middle calix, including renal pelvis, or lower calix), laterality of the stones, multiple stones or simple stone, history of intervention for urolithiasis, and stone size by NCCT and US were retrospectively collected from medical records. Stone size was defined as the longest axis on US and NCCT. The classification of stone size between ≤5 and >5 mm was based on the size measured by NCCT. If renal stones are multiple, stone size was defined as the longest axis of the largest stones, not as the sums up of the longest axis of each stones. We classified stone sizes into three subgroups (0–5.0, 5.1–10.0, and ≥10.0 mm), and examined whether stone size measured separately by US and NCCT at first entry would fit in the same subgroup. Stone growth was defined as >50% from stone size at first entry in this study determined through US. The primary study endpoint was the rate of surgical intervention. Secondary endpoints included stone-related events, such as spontaneous stone passage, fever, hematuria, pain, and stone growth.
Statistical analyses
Statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). 12 Propensity score matching was performed between patients with renal stones ≤5 mm and those with renal stones >5 mm. The patients were matched in one-to-one fashion according to age, sex, history of stone treatment, single stone or multiple stones, and stone location. A caliper width of 0.2 for the standard deviation was applied. The chi-square test or Fisher's exact test was used to determine any significant differences in normal data. A two-tailed Student's t-test or Mann–Whitney U test was used to analyze differences in continuous variables. Moreover, univariable and multivariable Cox regression was used to estimate hazard ratios for potential predictors of all surgical interventions and surgical intervention for active indication. The Kaplan–Meier curves were utilized to describe surgical intervention and stone-related event. A p-value <0.05 was considered significant.
Results
Patient characteristics
At final analysis, this retrospective study included 207 patients (71 cases with renal stones ≤5 mm on NCCT and 136 cases with renal stones >5 mm on NCCT). Table 1 shows the patients' characteristics. Among the patients, about two-thirds were men, and the median age was about 60 years of age, and approximately half of the patients had a history of surgical intervention for urinary stones. The incidence of multiple renal stones and history of intervention for urolithiasis was lower in the group with ≤5 mm stones compared with the group with >5 mm renal stones. As for stone size measurement by NCCT and US at first entry, we classified stone sizes into three subgroups (0–5.0, 5.1–10.0, and ≥10.0 mm). Similarity in stone group size was 159 of 207 (76.8%), indicating that that US are reliable to some extent in stone size measurement (Supplementary Table S1).
Patients' Characteristics Before Matching
IQR = interquartile range.
To evaluate the patients' background, propensity score matching was performed to compare the rate of surgical intervention and stone-related events between the ≤5 and >5-mm groups (Supplementary Table S2). A total of 50 matched pairs were available for the final analysis. There was no significant difference observed as regards the incidence of multiple renal stones and history of intervention for urolithiasis as well as age, sex, history of stone treatment, single stone or multiple stones, and stone location between both groups after matching.
Surgical intervention
Table 2 presents the details of stone-related surgical intervention. A total of 66 patients (31.9%) received surgical intervention (SWL in 57 cases and ureteroscopy in 9 cases) at a median follow-up of 3.3 years. Moreover, 14 patients (20%) in the ≤5-mm group and 52 (38%) in the >5-mm group underwent surgical treatment, and a statistically significant difference was noted between the two groups (p = 0.0067). The Kaplan–Meier estimate revealed that the 5-year estimate intervention rates of the ≤5 and >5-mm groups were 23.7% and 36.9% (p = 0.0238), respectively (Fig. 1A). Limited to active treatment indications (descending stones into the ureter and stone-related symptoms such as pain hematuria, fever), 11 patients (16%) from the ≤5-mm group and 27 (20%) from the >5-mm group underwent surgical treatment, showing no significant difference (p = 0.44). The Kaplan–Meier estimate also revealed that there was no significant difference in the estimated surgical intervention rates for active indication between the ≤5 and >5-mm groups (p = 0.400) (Fig. 1B). In contrast, nonactive treatment indications (stone growth and patient's choice) were more common in the >5-mm group (p = 0.0047). After propensity score matching, 12 patients (24%) from the ≤5-mm group and 20 (40%) from the >5-mm group underwent surgical treatment, showing no significant difference (p = 0.086) (Supplementary Table S3). Again, 9 patients (18%) in the ≤5-mm group and 12 (24%) in the >5-mm group underwent surgical treatment for active treatment indication, showing no significant difference (p = 0.46). The Kaplan–Meier estimate also revealed that there was no significant difference after propensity score matching (Fig. 1C, D).

Kaplan–Meier curve of intervention rate in the ≤5 and >5-mm groups for all surgical interventions
The Details of Surgical Intervention and Stone-Related Event Before Matching
SWL = extracorporeal shockwave lithotripsy.
Stone-related events
As regards stone-related events, the incidence of fever was significantly higher in the >5-mm group than in the ≤5-mm group (22.8% vs 11.3%, respectively; p = 0.044), but there were no significant differences noted in the rates of spontaneous stone passage, hematuria, pain, or stone growth (Table 2). Kaplan–Meier estimate revealed that 5-year estimated rates for each stone-related event, except for fever between the ≤5 and >5-mm groups were not significantly different (Fig. 2). After propensity score matching, the comparison of each stone-related event and Kaplan–Meier estimation between the ≤5 and >5-mm groups showed similar results (Supplementary Table S3 and Supplementary Fig. S1).
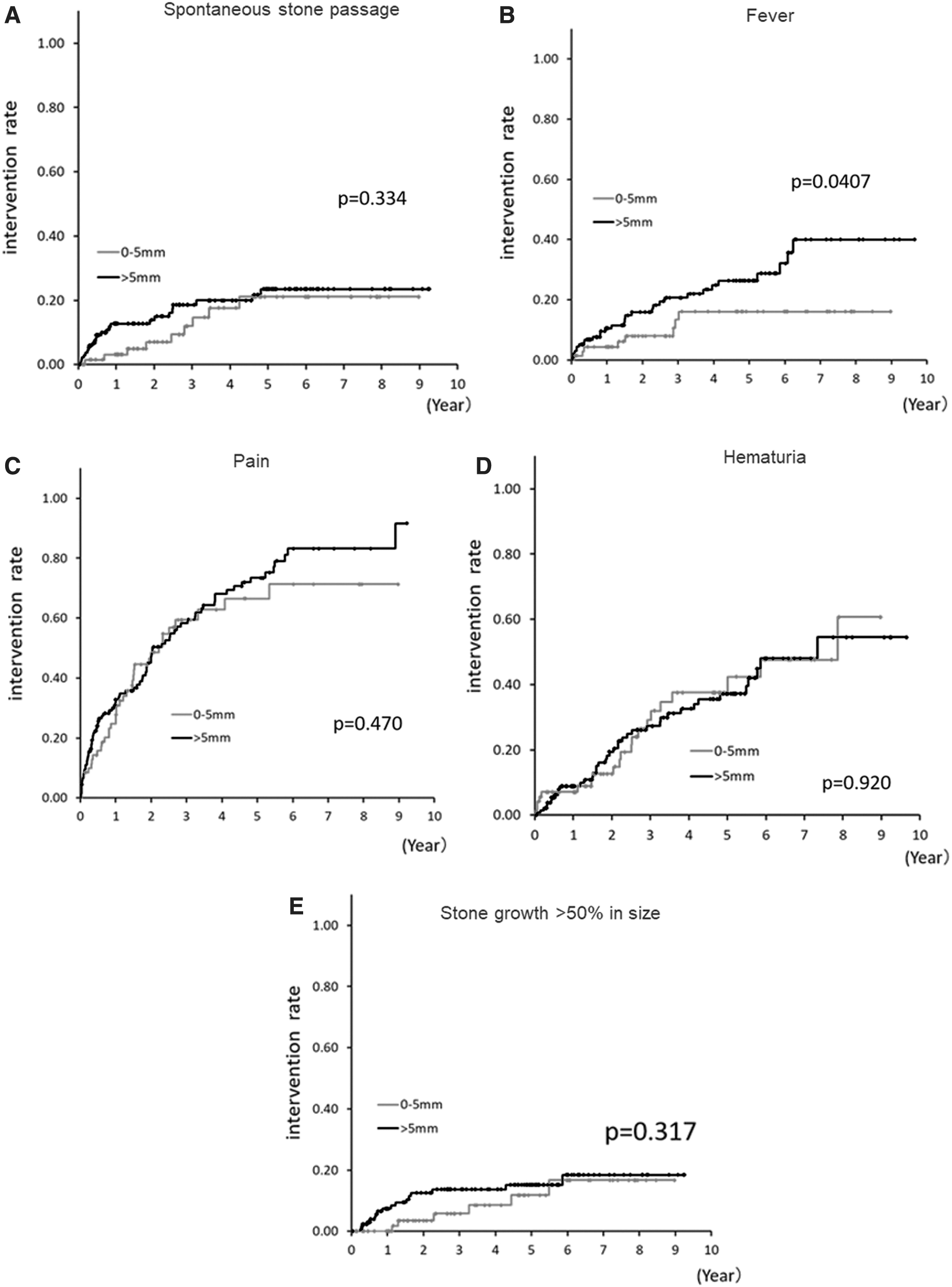
Kaplan–Meier curves of stone-related events. Spontaneous stone passage
The risk factor for surgical intervention
Finally, factors associated with all surgical interventions (n = 66) and surgical intervention (n = 38) for active treatment indication were analyzed using univariate and multivariate Cox proportional-hazards models (Table 3). In univariate analysis, stone size was a significant factor for all surgical interventions in addition to laterality of stones and history of stone treatment. Contrarily, in multivariate analysis, age ≤50 years and history of intervention for urinary stones were significant factors, but stone size was not.
Univariable and Multivariable Cox Regression Analysis of Variables Associated with All Surgical Interventions or Surgical Intervention for Active Indication
CI = confidence interval; HR = hazard ratio.
For surgical intervention for active treatment indication, stone size (≤5 mm) was not a significant factor on both univariate and multivariate analysis; however, age ≤50 years and history of surgical intervention for urolithiasis were significant factors on multivariate analysis.
Based on the two prognostic factors (age ≤50 years and history of stone surgery), the patients with asymptomatic renal stones ≤5 mm were divided into two risk groups. The 5-year intervention rate in patients with one or two adverse factors was 35.0%, whereas in patients with zero adverse factors, it was only 4.4%, indicating a statistically significant difference between the two groups (p = 0.042) (Supplementary Fig. S2).
Discussion
In several guidelines, calculi smaller than 5 mm have been considered as insignificant stones, 8,9 but there are no data specific to the natural history of asymptomatic renal stones ≤5 mm. This study first clarified the natural history of small asymptomatic renal stones, specific to <5 mm in size. To evaluate the natural history of asymptomatic small renal stones, accurate diagnosis for small stones is required during the primary imaging procedure and at follow-up. NCCT is believed to be a better procedure for the detection of stones ≤5 mm than kidney, ureter, and bladder radiograph (KUB) or US; however, repeat NCCT should be avoided due to radiation exposure. We have previously reported that renal stones ≤5 mm were difficult to be visualized by KUB and the specificity by US was low. 10,11 In this regard, this study is unique in that renal stones confirmed by both NCCT and US at diagnosis were followed up by US, resulting in accurate diagnosis for stones ≤5 mm and follow-up without radiation exposure.
There is substantial variation in reported rates of surgical intervention from 7.1% to 40%, spontaneous stone passage from 3.1% to 29.1%, symptom development from 7.3% to 77.0%, and stone growth from 5.2% to 66.0% in patients with asymptomatic renal stones (Supplementary Table S4). 3,13 –18 This discrepancy is believed to be due to the difference in indications for surgical intervention, the difference in the definition for symptom development or stone growth, the length of follow-up, and the difference of the cohort in each study. The incidence of surgical intervention in our study is within the range of that from previous reports but is rather high. There are two possible reasons for this. First, in this study, surgical intervention was also performed for stone growth or at the patient's request as well as in patients with active treatment indications (stone relocation into the ureter; and stone-related symptoms such as pain, hematuria, and fever). Limited to active treatment indications, the incidence of surgical intervention was not relevantly high. Second, the number of patients in this study with previous history of surgical intervention for urolithiasis was high. The high incidence of surgical intervention especially for stones ≤5 mm may reflect the natural history of patients with residual stones after surgical intervention. 19 Recent studies have suggested that residual stones >4 mm after PCNL and ureteroscopy are associated with a higher likelihood for reintervention. 20 –22
Several studies have reported factors associated with surgical intervention during active surveillance, including male sex, age (≤50 years), the rate of stone growth, stone history, and stone size. 3,5,7,15,17 In this study, age ≤50 years and a history of surgical intervention were significant factors associated with surgical intervention, but not stone size <5 mm. Interestingly, in the present study, the incidence of surgical intervention was low in patients above 50 years of age with asymptomatic renal stones ≤5 mm and without a history of surgical intervention. Follow-up of these patients could safely be reduced.
This study had inherent limitations. First, this was a retrospective study and, as such, may be subject to confounding or bias. Second, analysis of patients who were already on surveillance at the start of study period was restricted to the study period dates and not the start date of surveillance. This protocol could underrepresent the efficacy of the surveillance group. Third, the study cohort underwent NCCT and US imaging on the same day, and the study may have included high-risk patients, such as those with a history of intervention for urolithiasis. Fourth, the sample size in this study is small and not enough, particularly the group with renal stones <5 mm.
Despite the limitations, to the best of our knowledge, this study is the first to evaluate the natural history of asymptomatic renal stones <5 mm in size using strict inclusion criteria. We believe that the question of whether asymptomatic renal stones ≤5 mm can cause stone-related events and require surgical intervention deserves attention in our daily clinical practice.
Conclusions
About 20% of asymptomatic renal stones ≤5 mm require surgical treatment within 5 years. These results are useful when urologists discuss whether to perform conservative management with active surveillance imaging or prophylactic surgical intervention with patients with small asymptomatic renal stones ≤5 mm.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.