
Abstract
Purpose:
To investigate the safety of microwave ablation (MWA) as an emerging technology for treating small renal masses.
Materials and Methods:
Patients with renal masses treated at a high-volume center with MWA between March 2015 and June 2019 were retrospectively identified. Safety, changes in renal function, primary treatment efficacy, and the natural history of imaging characteristics of masses postablation were examined.
Results:
Forty-five patients underwent MWA during the study period. Median age was 71 years (range 31–87). Median RENAL nephrometry score was 6 (range 4–9) with mean tumor size 2.6 ± 0.7 cm. Thirty-three percent of tumors were within 4 mm of the collecting system. Median total microwave energy applied was 400 W (range 105–2600 W). There was no significant change in creatinine (p = 0.21) or glomerular filtration rate (GFR) (p = 0.09) from preoperative to postoperative day 1 (POD#1) levels. There was a statistically but not clinically significant decrease in hemoglobin from preoperative to POD#1 levels (estimated −0.06 from 7 days before procedure to POD#1, p = 0.02). There was no durable change in creatinine (p = 0.16) or GFR (p = 0.72) at median follow-up of 7.5 months. There were 4 (9%) complications: three Clavien grade 1 and one Clavien grade 3 that led to loss of the kidney. Tumor size decreased postoperatively by an estimated −0.03 cm/month (range 0–1.9 cm, p < 0.01). Initial technical success was 100%. Primary treatment efficacy was 94%.
Conclusion:
MWA shows promise as an alternative thermal ablative technique with excellent short-term outcomes.
Introduction
Radiofrequency ablation (RFA) and cryoablation (CA) are accepted treatment alternatives to extirpative surgery for the treatment of cT1a renal masses. 1 More recently, microwave ablation (MWA) has shown promise as an alternative thermal ablative technique that may offer theoretical advantages due to a more rapid heating action, which may limit thermal heat sink. 2 First described in 2007, subsequent clinical studies have shown reduced procedure time and dose of sedative medication during MWA compared with RFA and CA with similar oncologic and renal functional outcomes. 3 –5 However, the safety of MWA remains less well studied than either RFA or CA with mixed results within the literature. 6,7
This study describes a single center experience with MWA over 4 years at a high-volume center with significant prior experience with percutaneous ablation. Specifically, renal functional outcomes and perioperative complications as well as the natural history of the imaging characteristics of microwave-ablated tumors were examined. Short-term oncologic outcomes, including local recurrence-free survival (LRFS), cancer-specific survival (CSS), and overall survival (OS), after MWA were secondarily evaluated.
Patients and Methods
Patients treated with MWA at our institution between March 2015 and June 2019 were retrospectively reviewed under Institutional Review Board approval. Data were gathered on patient demographics, oncologic history and outcomes, tumor characteristics, including pathology and RENAL nephrometry score, pre- and postoperative hemoglobin, creatinine, and glomerular filtration rate (GFR), and postoperative complications. Both the standard RENAL nephrometry score and a modified RENAL nephrometry score were used to better categorize small renal masses. 8 Renal functional outcomes, complications, and imaging characteristics of masses postablation were assessed. Short-term oncologic outcomes were also evaluated.
Tumor ablation was carried out under CT guidance using either a Siemens Somation AS Plus or Seimens Somatom Definition AS scanner (Siemens Corporation, Munich, Germany) with a technique similar to that previously described in our institutional algorithm for RFA. 9 In brief, patients were placed prone in the CT gantry, and an initial helical scan was performed to identify tumor location. The patient was marked using an external grid, and the ablative probe was passed into the tumor using repeated 3-slice procedural CT images. Once the probe was correctly placed, intravenous contrast (1 cc/kg) was injected to confirm appropriate needle placement within the center of the tumor before subsequent ablation. For entirely endophytic tumors, intraoperative ultrasound and early contrast administration were used to plan needle placement. Ablation parameters were based on lesion size, and treatment algorithms were determined by the manufacturer's suggested settings with a planned margin of ∼5 mm. MWA was performed using the Solaro microwave tissue ablation system (Angiodynamics, Latham, NY), and either a 14 or 19 cm 15 Ga probe based on skin to tumor distance. A contrasted postablation CT scan was obtained at 5 minutes after the ablation to ensure complete ablation of the lesion, as indicated by no residual enhancement within the lesion, and evaluate for immediate postoperative complications. Procedures were performed by a team of a single urologist and two interventional radiologists, all of whom had performed >100 prior renal ablations (CA and RFA). According to institutional protocol, all patients were admitted postoperatively for overnight observation. Serum complete blood counts and electrolytes were obtained on postoperative day 1 (POD#1) before discharge. Patients underwent either CT or MRI at 6 weeks, depending on renal function and allergies to contrast agents, then every 6 months for 2 years, then annually thereafter.
Initial technical success was defined as no residual enhancement within the entire tumor on immediate postprocedure contrasted CT scan. Based on the recommended standardization of reporting outcomes in image-guided tumor ablation by Ahmed and colleagues, primary treatment efficacy was defined as lack of nodular enhancement or growth on first follow-up CT scan, with enhancement being defined as a change of >10 HU and growth defined as any increase in size compared with preoperative imaging. 10 Disease recurrence was defined as development of new nodular enhancement or growth after an initially negative follow-up CT scan.
Statistical analysis
Changes in laboratory values and tumor size over time were assessed using mixed-effects regression models assuming a compound symmetry covariance structure. Survival probabilities were estimated and plotted using the Kaplan–Meier method. Estimates along with 95% pointwise confidence intervals were reported. For LRFS, time was calculated from ablation to recurrence. Patients without recurrence were censored on date of last surveillance. For CSS and OS, time was calculated from ablation to death due to renal cell carcinoma (RCC) or death due to any cause, respectively. Patients still alive were censored on date of last follow-up. All statistical testing was two sided and assessed for significance at the 5% level using SAS v9.4 (SAS Institute, Cary, NC).
Results
Demographics
Forty-five patients (71% male) underwent MWA during the study period (Table 1). The median age was 71 years (range 31–87 years). Mean preoperative body mass index was 32.3 ± 8.0. All patients had an American Society of Anesthesiologists (ASA) score of ≥2, and 62% of patients had an ASA of ≥3. There were 10 (22%) patients who had a history of RCC treated with either radical nephrectomy (3/10), partial nephrectomy (4/10), or both partial and radical nephrectomy (1/10), and 4 (9%) patients had solitary kidneys. One patient had undergone prior RFA for a separate RCC, and one patient had undergone both partial nephrectomy and RFA for two separate RCCs. No patient had a history of metastatic RCC.
Demographics
ASA = American Society of Anesthesiologists; BMI = body mass index; RCC = renal cell carcinoma.
The mean tumor size was 2.6 ± 0.7 cm, while median RENAL nephrometry score and modified RENAL nephrometry score were both 6 (both range 4–9). The mean distance of the tumor from the collecting system was 8.9 ± 5.0 mm, with 33% of masses within 4 mm of the collecting system. The mean skin to lesion distance was 9.2 ± 3.5 cm, and the median total microwave energy applied was 400 W (range 105–2600 W).
Thirty-four patients (76%) had either a biopsy-proven RCC or a history of contralateral or ipsilateral RCC. For many of these patients, biopsy was not obtained before ablation, as there is a known high pathologic concordance between initial pathology and recurrent masses, even contralaterally. 11 Two other patients had an intraoperative biopsy showing either oncocytoma (1) or normal renal parenchyma (1), the latter of which was deemed to be an inaccurate biopsy. Eleven patients without a history of RCC chose not to undergo biopsy following informed consent. Nine of these patients were treated due to progression on active surveillance with a median growth rate of 8 mm/year (range 1.5–18 mm/year).
Renal functional outcomes and postoperative complications
On POD#1, there was a statistically significant but not clinically significant decline in hemoglobin from preoperative levels (p = 0.02, estimated −0.06 from 7 days preoperatively to POD#1, Fig. 1), which is likely explained by intraoperative intravenous fluid administration as there were no hemorrhagic complications. There was neither a significant decline in POD#1 creatinine (estimated 0.03 mg/dL/month, p = 0.21, Fig. 1) nor GFR (estimated −1.53 mL/minute/1.73-m2/month, p = 0.09, Fig. 1), or any further decline in either creatinine (estimated 0.004 mg/dL/month, p = 0.16) or GFR (estimated −0.05 mL/minute/1.73-m2/month, p = 0.72, Fig. 1) at last laboratory evaluation (median 7.5 months). There were four complications (9%): three were Clavien grade 1 complications, all of which resolved conservatively, including hyperkalemia and postoperative pain requiring readmission, delayed urine leak, and perinephric fluid collection. There was one Clavien grade 3 complication, an intrarenal stricture caused by fibrosis presenting 8 months postprocedurally, which eventually led to loss of function of the kidney on nuclear renal scan. There was no association between tumor distance to the collecting system or RENAL nephrometry and complications, although the small number of complications limited analysis.
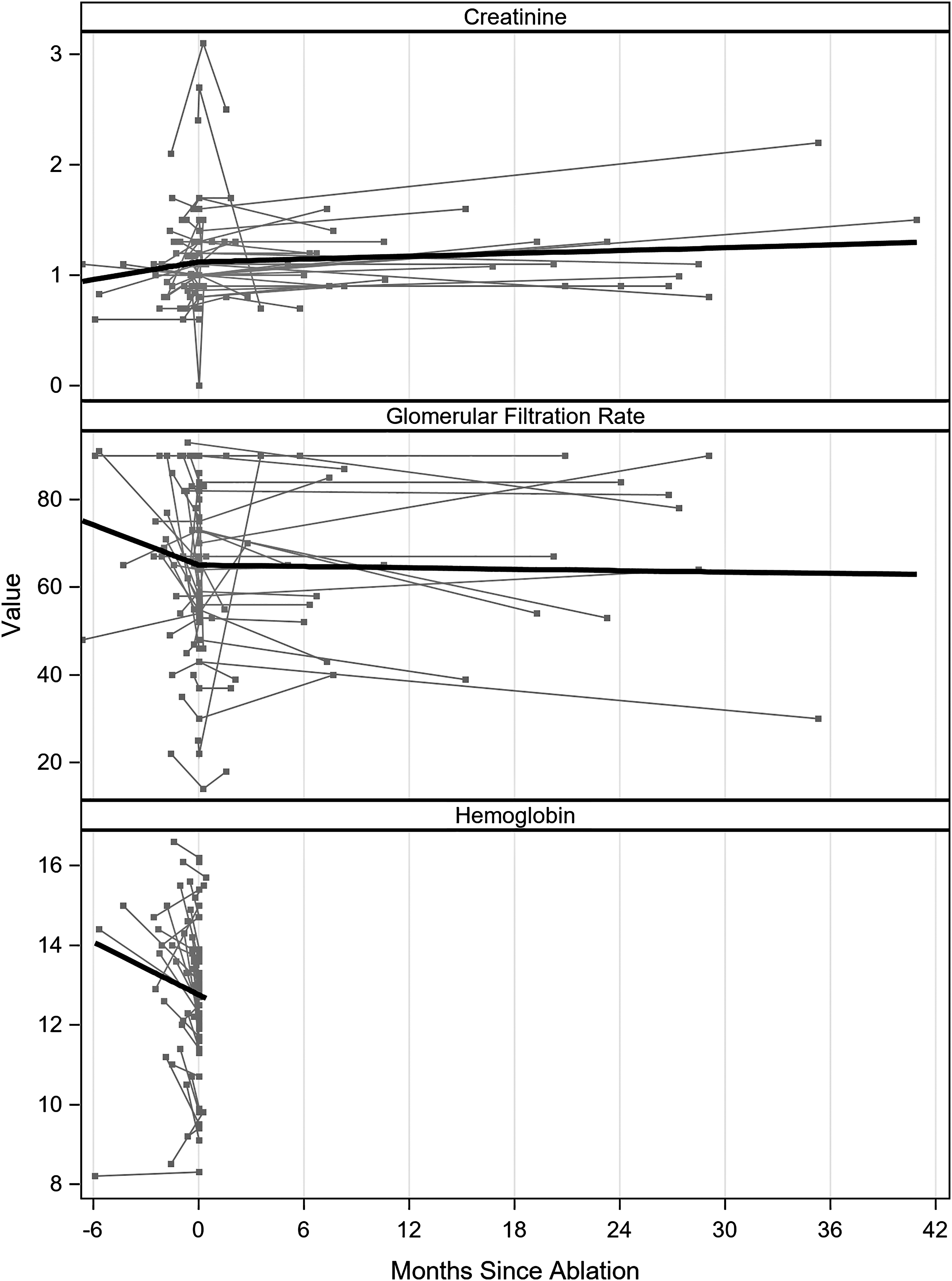
Change in creatinine, GFR, and hemoglobin after MWA over time. While there was a slight statistically significant decline in hemoglobin on POD#1 (estimated −0.06 from 7 days before surgery to POD#1; p = 0.02), there was no change in postoperative creatinine (p = 0.21) or GFR (p = 0.09). There was also no long-term decline in creatinine (p = 0.16) or GFR (p = 0.72) with median follow-up 7.5 months. GFR = glomerular filtration rate; MWA = microwave ablation; POD#1 = postoperative day #1.
Short-term oncologic outcomes
Initial technical success was 100%, with all (45/45) patients having an initially effective ablation on immediate postablation imaging. Of the 45 patients in the study, 36 patients had at least one follow-up, contrast-enhanced scan, and were included for subsequent analysis of treatment effect. Two patients had persistent disease at their initial 6 week follow-up based on a nodular area of enhancement on cross-sectional imaging, equivalent to a primary treatment efficacy rate of 94% (34/36). One of these patients underwent repeat ablation secondary to a thick rim of enhancing nodular tissue along the parenchymal edge, while the other patient was observed for a 4 mm island of enhancement within the center of the tumor on delayed imaging. In the second patient, subsequent imaging at 6 months and out to last follow-up at 24 months showed complete resolution of this area without further contrast enhancement, such that this patient was considered as an initial treatment failure but reclassified thereafter as having no local recurrence. Median surveillance follow-up was 8.0 months (range 0.8–44.6 months) for patients with at least one follow-up scan. Tumor size decreased postoperatively by an estimated −0.03 cm/month (range 0–1.9 cm, p < 0.01, Fig. 2). One patient of the 36 with follow-up contrast-enhanced imaging developed new enhancement within a previously treated lesion at 9 months and underwent laparoscopic nephrectomy with final pathology demonstrating pT3a WHO/ISUP grade 3/4 RCC. One-year LRFS, CSS, and OS were, therefore, 94%, 100%, and 92%, respectively (Fig. 3A, B).

Change in tumor size after MWA over time. There was a statistically significant decrease in tumor size over time of approximately −0.03 cm/month (p < 0.01). Black line represents best model fit.

The Kaplan–Meier curves showing recurrence-free and OS.
Discussion
MWA is an emerging ablation technology for renal masses with potential benefits over RFA. 12 –14 Prior studies have shown shorter procedure times and reduced sedative requirements with MWA compared with RFA, as well as superior delivery of heat into renal tissue due to the inherent physical properties of microwave energy. 3,4,15 Despite these promising results, the literature is still in its infancy with wide variability in outcomes data and complication rates. 6,7 Results of this study show that in a center with extensive experience in percutaneous ablation, transitioning to MWA allows for similar complication rates compared with previously established thermal ablation. 16,17 This study also describes the natural history of the imaging characteristics of these masses postablation and secondarily examines short-term oncologic outcomes.
The rate of complications after MWA in our study is similar to the 10%–17% complication rate of RFA reported in the literature, with the majority of complications in this study (3/4) being Clavien grade 1. 3,18 Importantly, the low rate of urine leak in our study (3%), despite treatment of tumors adjacent to the collecting system, is comparable with RFA. 19,20 Our results also contradict those of a recent study by Thompson and colleagues, which described a relatively high (11.5%) rate of postoperative bleeding and urinary complications with MWA, as there were no bleeding complications or clinically significant changes in postprocedural hemoglobin and only a single Clavien grade 3 urinary complication (3%) despite treating multiple tumors in proximity to the collecting system. 6 Our results also contrast with the initial experience described in a case series by Castle and colleagues in 2010, who reported a high rate of major complications in a mixed group of 10 percutaneous and laparoscopic cases as well as a recurrence rate of 38%. 21 In addition to the difference in technique, patients in that study were far more likely to have pT1b tumors and tumors involving the collecting system, both of which are factors likely to decrease success rates and increase complications. With appropriate patient selection, our results show that percutaneous MWA can be safe, efficacious, and equally as nephron sparing as other thermal ablation technologies with no change in postoperative creatinine or GFR. 3,18
Changes in imaging characteristics after RFA and CA have been well described, with CA typically showing faster involution than RFA. 22 However, the rate of decline in the size of renal masses after MWA has not previously been reported. Our findings show that lesions treated with MWA will generally decrease in size by −0.03 cm/month without an initial increase in size as seen with RFA, but the magnitude of the decrease is not as pronounced as that reported for CA. 23,24 Our results show the relatively short-term changes seen in the size of renal masses treated with MWA with a median follow-up of 8 months. Additional studies are needed to fully evaluate long-term changes in imaging characteristics on surveillance of these renal masses postablation.
One patient in our cohort had an area of focal enhancement (5 mm) within the center of the ablated lesion noted on first follow-up scan, but this area was noted to resolve on 6 month follow-up imaging. Reasons for early persistent enhancement are unclear, though they are likely related to postoperative hyperemia and inflammation, as seen following other ablation technologies. 25 Similar to other ablative techniques, larger areas of nodular enhancement or irregular peripheral enhancement within the ablation zone should be considered an incomplete ablation, whereas small areas of focal enhancement within the ablated zone should be interpreted with caution on the initial scan and may be safely observed with short-term follow-up.
With regard to oncologic outcomes, even with short-term follow-up, our overall technical success and our 1-year RFS, CSS, and OS rates are similar to those reported in the literature for MWA as well as RFA and CA. Contemporary short-term results for MWA have shown initial technical success between 94% and 100%. 4,5,14,26 Six month to 1 year follow-up in the literature after MWA has shown RFS between 85% and 100%, CSS ∼96%–97%, and OS from 81% to 93%. 4,14,26 Short-term results for RFA are similar, with 85%–97% initial technical success, 84% RFS, and 100% CSS at 3 years. 16,18 CA also yields similar short-term oncologic outcomes, with initial technical success reported at 93%–96% and 1-year disease-free and OS at 96% and 97%, respectively. 4,27 –29
Because of the limited number of complications in our study, we were unable to fully investigate individual risk factors for postoperative complications. Nevertheless, we were able to treat multiple central tumors, and despite a third of patients having tumors within 4 mm of the collecting system, urinary complications were rare. The single institutional nature of the study allowed for homogeneous follow-up and ablative technique but may limit the generalizability to less experienced or more heterogeneous practices. Many of these patients with significant comorbidities strongly preferred ablation over extirpative surgery. Since ablation efficacy is known to decrease with increasing tumor size, they opted for ablation without first undergoing biopsy based on rapid growth rate (average 8 mm/year) during active surveillance. 30,31 While the lack of pathologic data for these patients limits evaluation of long-term oncologic outcomes, their short-term outcomes are important with regard to measuring technical success, complications, and postoperative renal function. Indeed, these patients had similar outcomes to those with biopsy-proven disease, and no patient had any further growth of their tumor after MWA, despite the relatively rapid growth preprocedurally.
Conclusion
MWA shows promise as an alternative thermal ablative technique. In centers with experience in thermal ablation, MWA can safely be added to the treatment paradigm for treatment of both exophytic and endophytic tumors, including some tumors with proximity to the renal collecting system, with complication rates comparable with other percutaneous thermal ablative techniques.
Footnotes
Acknowledgment
The authors thank the Watts Family Fellowship in Urology for supporting this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Watts Family Fellowship in Urology at the University of Iowa.