
Abstract
Purpose:
Unplanned conversion from minimally invasive surgery (MIS) to open surgery is a significant challenge, although the frequency of conversion for robotic and laparoscopic kidney surgery is not well described. We aimed to compare rates of conversion for robotic versus laparoscopic kidney surgery.
Methods:
The National Cancer Database was used to identify patients who underwent robotic or laparoscopic partial nephrectomy (PN), radical nephrectomy (RN), or nephroureterectomy (NU) from 2010 to 2014. Multivariate logistic regression was used to identify factors associated with conversion to open. Length of stay and 30-day mortality rate were compared between groups using Kruskal–Wallis and Fisher's exact tests. Propensity score matching was performed to confirm study results.
Results:
A total of 61,191 patients underwent MIS PN, RN, or NU. Conversion rates were lower for robotics than for laparoscopy (PN: 2.1% vs 6.4%; RN: 4.9% vs 6.0%; NU: 3.8% vs 9.2%; P < 0.001). Median length of stay was longer for patients who underwent conversion than for those who did not (PN: 4.0 vs 2.0 days; RN: 4.0 vs 3.0; NU: 5.0 vs 4.0; P < 0.0001). Thirty-day mortality rate was higher for patients who underwent conversion (PN: 0.24% vs 1.42%; RN: 0.73% vs 2.71%; NU: 1.0% vs 3.0%, P < 0.001). Results were confirmed in propensity score-matched cohorts.
Conclusions:
Among patients undergoing minimally invasive kidney surgery, robotics is associated with a lower rate of unplanned open conversion than laparoscopy. This relative advantage has implications on length of stay and short-term mortality rate and should be considered when weighing the costs and benefits of robotic kidney surgery.
Introduction
The earliest reports of laparoscopic renal surgery emerged in the early 1990s. 1,2 As experience with this technology grew, institutional case series demonstrated that this approach was safe, technically feasible in experienced hands, and oncologically noninferior to open surgery. 3 –5 In the late 1990s and early 2000s, there was increasing adoption of laparoscopic kidney surgery in real-world clinical practice. 6,7 More than a decade after the introduction of laparoscopy, robotics emerged as the next major technologic advancement in minimally invasive kidney surgery. 8 –10 Indeed, in recent years there has been widespread adoption of robotic kidney surgery. 11
Retrospective studies have demonstrated a relative advantage of robotics over laparoscopy for select perioperative outcomes, such as operative duration, ischemia time, and blood loss. 12,13 However, with both laparoscopy and robotics, unplanned intraoperative conversion to open surgery remains a significant challenge. 14,15 Intraoperative conversion may increase morbidity and may offset the benefits of minimally invasive surgery (MIS).
The relative conversion rates to open surgery between robotic and laparoscopic surgery for renal and upper tract malignancies are not well characterized. A deeper understanding of unplanned intraoperative conversion during minimally invasive renal surgery has implications for surgical planning, preoperative patient counseling, and cost–benefit analyses of robotic technology. This study aims to compare rates of unplanned conversion between robotic and laparoscopic partial nephrectomy (PN), radical nephrectomy (RN), and nephroureterectomy (NU) using the National Cancer Database.
Methods
Study population
The National Cancer Database (NCDB) was used to identify patients undergoing laparoscopic or robotic PN, RN, or NU from 2010 to 2014. The NCDB is a national hospital-based all-payer cancer registry capturing all geographic regions in the United States. The NCDB encompasses >70% of all incident cancer cases, and includes >34 million patients.
Primary insurance coverage was categorized into private, public (including Medicare, Medicaid, or “Other Government” insurance), and uninsured. Facility type was based on Commission on Cancer accreditation categories that include Community (100–500 new cancer cases annually), Comprehensive Community (>500 new cases), Academic (>500 new cases and ≥4 residency training programs), and Integrated Network (provides integrated cancer care, no case requirement). Income and education quartiles were based on US Census data for the patient's residential zip code. Urban/rural classification was based on population density data from the United States Department of Agriculture Economic Research Service. Facility surgical volume and geographic distance from patient's residence to treatment facility were categorized into tertiles to facilitate analyses.
A total of 90,819 patients were initially identified. Patients with incomplete or missing data on income (n = 2740), education (n = 2746), urban/rural classification (n = 2175), insurance (n = 988), tumor size (n = 805), clinical T-stage (n = 17,195), clinical N-stage (n = 10,650), clinical M-stage (n = 7211), or facility type (n = 4536) were excluded from analyses. This yielded a final study cohort of 61,191 patients. The primary outcome was explored in the excluded cohort, and noted to be similar to that of the study cohort (Supplementary Table S1).
Outcomes
The primary study outcome was unplanned conversion from MIS to open surgery. This was defined as either “Robotic converted to open” or “Laparoscopic converted to open” in the NCDB “Surgical Approach” variable. Secondary outcomes included length of inpatient hospital stay as well as 30-day all cause mortality rate. Secondary outcomes were compared between study groups, as well as with an additional cohort of 42,860 patients undergoing a priori open surgery (n = 15,418 PN, n = 26,186 RN, n = 1256 NU).
Statistical analyses
Baseline clinical and sociodemographic patient characteristics and crude conversion rates for laparoscopy versus robotics were compared using chi-square test. Multivariate logistic regression assessed likelihood of unplanned conversion for robotics versus laparoscopy while adjusting for all relevant clinical and sociodemographic covariates. Inpatient length of stay was compared among patients who underwent successful MIS, MIS converted to open, and a priori open surgery using the Kruskal–Wallis test. Crude rates of 30-day mortality rate were compared across these groups using the Fisher's exact test. Adjusted 30-day mortality rate outcomes were examined using multivariate logistic regression, accounting for clinical and sociodemographic characteristics. All analyses were performed separately within the PN, RN, and NU cohorts.
To adjust for covariate influence on treatment selection, 1:1 propensity score-matched cohorts were created for each procedure type using all available clinical and sociodemographic variables. Analyses were repeated within the propensity score-matched cohorts. Analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC). This study was deemed exempt by the Cleveland Clinic Institutional Review Board.
Results
A total of 61,191 patients underwent MIS PN (n = 24,691), RN (n = 33,644), or NU (n = 2856) between 2010 and 2014. Baseline clinical and sociodemographic patient characteristics are given in Table 1. Across all cohorts, the majority of patients were non-Hispanic white patients 55–75 years of age with low comorbidity burden (Charlson 16 score 0 or 1) and clinically localized disease.
Baseline Demographic and Clinical Characteristics by Surgery Type and Surgical Approach
Median household income for patient zip code, categorized as quartiles.
Number of adults in patient zip code who did not graduate from high school, categorized as quartiles.
Based on typology from the USDA Economic Research Service.
Facility designation based on Commission on Cancer Accreditation program classification.
As given in Figure 1, the rate of unplanned conversion from MIS to open procedure was lower for robotics than for laparoscopy (PN: 2.1% vs 6.4%; RN: 4.9% vs 6.0%; NU: 3.8% vs 9.2%; P < 0.0001). On multivariate logistic regression adjusting for all relevant patient and provider factors, robotics was independently associated with lower likelihood of conversion to open as compared with laparoscopy (PN: OR = 0.34, 95% confidence interval [CI] = 0.29–0.39; RN: OR = 0.84, 95% CI = 0.75–0.94; NU: OR = 0.38, 95% CI = 0.26–0.54; Table 2).
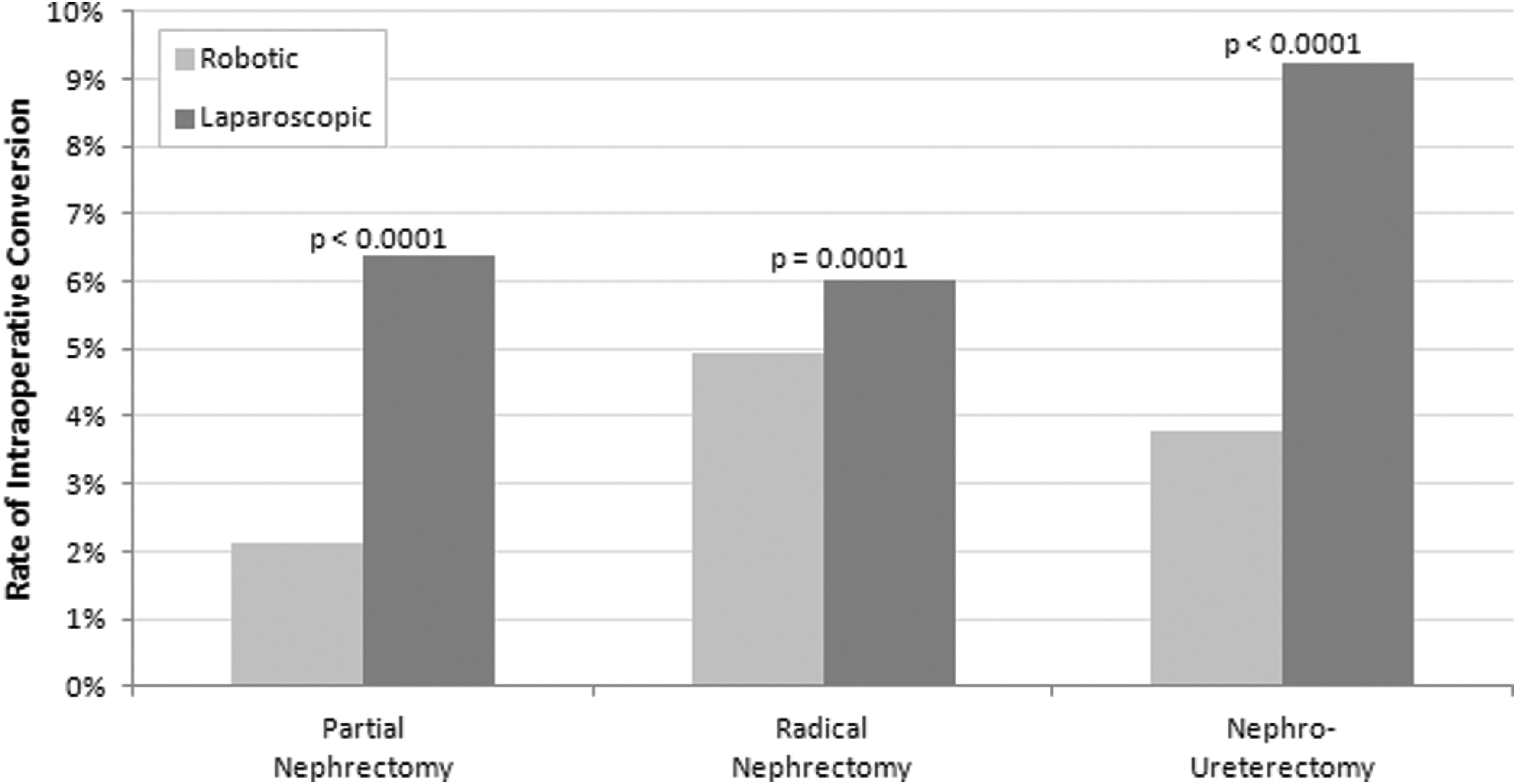
Unplanned intraoperative conversion from minimally iInvasive to open based on surgical approach.
Multivariate Logistic Regression to Identify Factors Associated with Unplanned Intraoperative Conversion from Minimally Invasive Surgery to Open Surgical Approach
Median household income for patient zip code, categorized as quartiles.
Number of adults in patient zip code who did not graduate from high school, categorized as quartiles.
Based on typology from the USDA Economic Research Service.
Facility designation based on Commission on Cancer Accreditation program classification.
OR = odds ratio; CI = confidence interval.
Robotic versus laparoscopic approach was the only variable that was independently associated with unplanned conversion across all multivariate models. In the PN and RN cohorts, higher clinical T-stage, clinical N1 disease, larger tumor size, and low surgical volume were all associated with increased likelihood of unplanned open conversion.
To examine the clinical impact of unplanned conversion, length of stay and 30-day mortality rate were compared among patients who underwent successful MIS, unplanned conversion from MIS to open procedure, and a priori open procedure. As given in Figure 2, patients who experienced conversion had longer inpatient length of stay than patients undergoing successful MIS across all surgery types (P < 0.0001). Figure 3 demonstrates that 30-day mortality rate was significantly higher in patients undergoing unplanned conversion than patients undergoing either successful MIS or a priori open procedure. Multivariate logistic regression confirmed a lower likelihood of 30-day mortality rate for successful MIS or a priori open surgery compared with unplanned conversion even after adjusting for clinical and sociodemographic characteristics (PN: MIS odds ratio 0.19 [95% CI = 0.09–0.41], open 0.32 [0.15–0.68]; RN: MIS 0.34 [0.24–0.49], open 0.59 [0.42–0.83]; NU: MIS 0.31 [0.11–0.88], open 0.82 [0.3–2.3]; Supplementary Table S2).

Association between unplanned intraoperative conversion and inpatient length of stay.
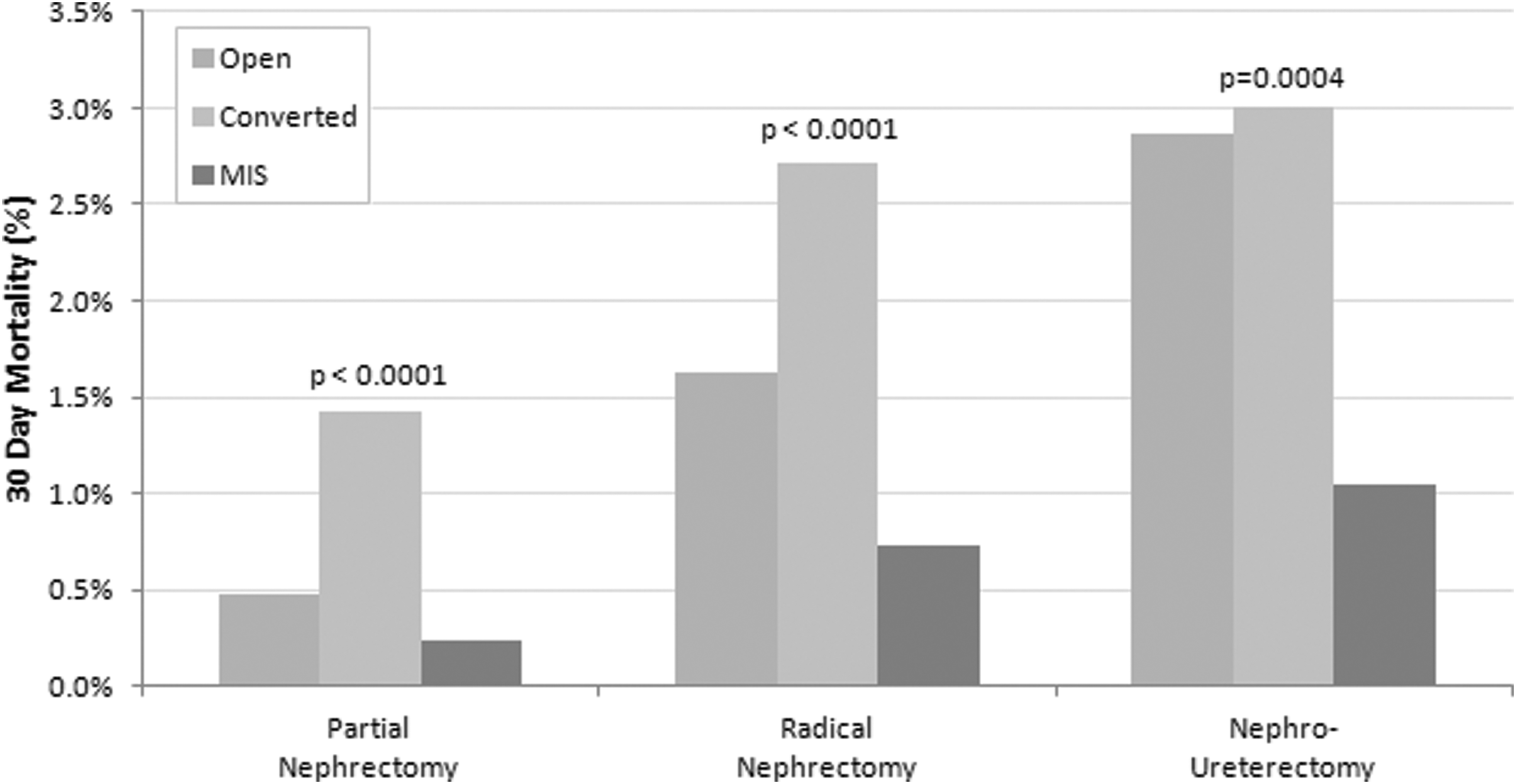
Association between unplanned intraoperative conversion and 30-day mortality rate.
As given in Table 1, inherent between-group differences existed at baseline. Multivariate regression models were used to adjust for potential measured confounders in the association between surgical approach and unplanned open conversion. However, some covariates may have influenced treatment selection (robotics versus laparoscopy). To account for this, propensity score-matched cohorts were created for each of the three major kidney surgery types. As given in Supplementary Table S3, these cohorts were well matched across most baseline variables. The laparoscopic and robotic groups still differed in year of diagnosis, which was a function of increasing adoption of robotic technology over time. Multivariate regression models were repeated in the propensity score-matched cohorts, and again demonstrated that robotics was associated with lower likelihood of open conversion than laparoscopy (PN: OR = 0.32 [0.25–0.39]; RN: OR = 0.84 [0.74–0.96]; NU: OR = 0.32 [0.22–0.47]; Supplementary Table S4). Median length of stay (days) was again longer for patients undergoing unplanned conversion than for those undergoing successful MIS (PN: 4.0 vs 2.0; RN: 4.0 vs 3.0; NU: 5.0 vs 4.0; P < 0.0001 for all). On multivariate logistic models in propensity score-matched cohorts, likelihood of 30-day mortality rate was lower in patients undergoing successful MIS than those undergoing unplanned conversion for PN (OR = 0.23, 95% CI = 0.07–0.72) and RN (OR = 0.32, 95% CI = 0.18–0.57).
Discussion
In this study of 61,191 patients undergoing minimally invasive kidney surgery using the National Cancer Database, robotics was independently associated with a lower likelihood of unplanned intraoperative conversion to open surgery than laparoscopy. Patients who experienced conversion had longer length of stay and higher 30-day mortality rate than those who underwent successful MIS procedures, suggesting the relevance of this outcome when evaluating the value of robotic kidney surgery.
Earlier comparative studies of robotic versus laparoscopic PN have focused on outcomes such as blood loss, operative time, and warm ischemia time (WIT). Institutional series and meta-analyses have suggested that robotics is associated with less blood loss, shorter WIT, 17 –19 shorter operative time, and a favorable learning curve. 12,13 However, these metrics are of unclear clinical significance. The most robust reductions in operative time and blood loss observed with robotics in previous studies were <40 minutes 13 and 100 mL, 12,13 respectively. The clinical utility of such marginal advantages is unclear. Furthermore, the most favorable advantage in WIT observed for robotics across all meta-analyses was <5 minutes. 18 However, recent literature suggests that minor changes in WIT have minimal impact on long-term renal function. 20,21
Unlike many of the previously studied outcomes, unplanned conversion from MIS to open surgery is relevant to patients, surgeons, and the overall health care system. For patients, conversion is associated with greater morbidity and a slower recovery. For surgeons, conversion represents a failure to complete the planned surgery using the tools available. For the health care system, observed increases in length of stay associated with conversion result in greater resource consumption. For all stakeholders, increased short-term mortality rate associated with conversion is of great consequence. Thus, unplanned intraoperative conversion from MIS to open surgery is a relevant and important outcome that warrants close study.
No previous studies have been designed to specifically study unplanned conversion during MIS kidney surgery as a primary outcome. Two previous meta-analyses have included open conversion as a secondary outcome. 18,19 Both demonstrated lower rates of conversion for robotics as opposed to laparoscopy. In addition, the three largest meta-analyses combined would yield a sample size of <8,000 patients, far smaller than this study of >60,000 patients. Furthermore, meta-analyses collate data from publications of individual surgeon outcomes, which selects for the highest volume surgeons with the most robust experience. These data are likely not applicable to real-world practice. The current dataset, on the contrary, includes well over 1000 hospitals performing MIS kidney surgery across all payers and practice settings. Finally, meta-analyses aggregate inherently heterogeneous data, and analytic strategies on these pooled data are limited. Authors cannot adjust for a wide range of covariates, nor can covariate influence on treatment selection be taken into account. This study evaluates the impact of robotics on unplanned open conversion far more rigorously than earlier studies by accounting for relevant clinical and sociodemographic covariates and employing propensity score matching.
In assessing perioperative outcomes between robotic and laparascopic RN among ∼24,000 patients in the Premier Health care database, Jeong and colleagues did not demonstrate any difference in complication rates between the two techniques. However, the authors did not study conversion rates from MIS to open surgery, nor did they stratify patients by clinical stage. 22 Of interest, only 22% of MIS nephrectomies in the aforementioned study were robotic, which mirrors trends seen in this study. Although benefits to the robotic approach were not noted by Jeong and colleagues, our study suggests a comparative advantage to robotic RN with regard to unplanned open conversion. This may be further appreciated in patients with clinical T3 or T4 disease, or tumor size >10 cm, as these characteristics also predict for open conversion on our multivariable analysis. Although the literature comparing MIS approaches for NU is limited, a recent meta-analysis did suggest that robotics achieved similar perioperative and oncologic outcomes to laparoscopy. 23 The authors did not evaluate unplanned intraoperative conversion, although results from this study would suggest a lower risk of conversion when using a robotic approach.
Unplanned conversion from MIS to open surgery is itself a meaningful and relevant outcome for both patients and surgeons. However, the downstream effects of unplanned conversion are noteworthy. In this study, patients who experienced unplanned conversion remained inpatient for 1–2 days longer than those who had successful MIS procedures. Although cost is not directly reported in NCDB, length of stay has previously been proposed as a direct surrogate for health care costs. 24 Indeed, inpatient hospitalization has been suggested as a significant driver of global health care costs associated with the surgery. 25 Thus, unplanned conversion not only adds to patient morbidity, but likely leads to increased cost for both patients and hospitals.
In addition to longer length of stay, unplanned conversion from MIS to open was also associated with higher rates of 30-day all cause mortality rate. These results persisted on multivariate analyses after adjusting for tumor, clinical, and sociodemographic characteristics. Mortality rate was higher in converted cases than in either successful MIS or a priori open surgery, suggesting that unplanned conversion may be a marker for technical difficulty during the surgery, the repercussions of which persist beyond the operating room. Thus, the implications of unplanned conversion during MIS kidney surgery cannot be overstated. No known previous studies have explicitly demonstrated the impact of unplanned conversion during MIS kidney surgery on short-term mortality rate.
This study is not without limitations. First, a significant portion of the original cohort was excluded owing to missing data on covariates. However, as shown in Supplementary Table S1, the primary outcome was similar between the study cohort and excluded cohort. Thus, the exclusion of this cohort is not likely to have affected study findings. Second, although propensity score matching was used to adjust for potential covariate influence on treatment selection, any retrospective study of this nature is limited by potential unmeasured confounders. Although a prospective randomized study would be ideal in theory, the feasibility of doing so for rare outcomes is low. Third, this study focuses on unplanned conversion from MIS to open surgery. The NCDB cannot capture cases of MIS PN that are converted intraoperatively to MIS RN. Furthermore, it is theoretically possible that some conversions may not have been accurately captured in the data registry. However, there is no reason to believe that the rate of data entry error would differ across surgical techniques (laparoscopic versus robotic), and thus unlikely to impact study findings.
Despite these methodologic considerations, this study represents an important contribution to the urologic literature. The dataset utilized is larger than all previous meta-analyses of robotic versus laparoscopic kidney surgery combined, and is representative of real-world clinical practice across all practice settings and inclusive of all payers. Furthermore, the use of multivariate logistic regression models and propensity score-matched cohorts allows for rigorous study of the association between surgical approach and unplanned conversion. Meaningful real-world impacts of unplanned conversion are also examined, including length of stay and short-term mortality rate.
Conclusions
In this hospital-based study using the NCDB, robotics was associated with a significantly lower likelihood of unplanned intraoperative conversion to open surgery as compared with laparoscopy for PN, RN, and NU. Unplanned conversion was associated with longer inpatient length of stay, which may translate into increased health care costs. Conversion was also associated with higher 30-day mortality rate. These study findings should be considered when performing cost–benefit analyses of robotic technology for major kidney surgery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.