
Abstract
Background:
We describe the oncologic and functional outcomes and the surgical technique of the photodynamic diagnosis (PDD)-assisted en bloc transurethral resection of bladder tumor (EBTUR) using a rectangular cutting loop.
Methods:
We reviewed 40 patients with carcinoma in situ-free nonmuscle invasive bladder cancer undergoing PDD-TURBT. Of 40 patients, 12 underwent photodynamic diagnosis-assisted en bloc transurethral resection of bladder tumor (PDD-EBTUR) and 28 underwent PDD-assisted conventional TURBT (cTURBT). Two groups were matched in terms of clinicopathologic background and did not include patients treated with intravesical Bacillus Calmette–Guerin. The assessment of postoperative quality of life (QoL) was based on patient-reported outcome measure, including the International Prostate Symptom Score, Functional Assessment of Cancer Therapy-Bladder (FACT-BL), and 8-item Short Form (SF-8™) questionnaires before and 1 month after TUR. This study was approved by the Ethics commitee and all participants provided informed consent.
Results:
PDD guidance provided substantial help for circumferent demarcation around the bladder tumor, which precedes tumor dissection. One female patient (12%) treated by PDD-EBTUR had grade II bladder perforation requiring prolonged catheterization. Pathologic assessment of horizontal and vertical margins in resected specimens by PDD-EBTUR revealed that all specimens had muscularis propria, and the rate of en bloc resection was 100%. No patient had intravesical recurrence in the PDD-EBTUR group (median follow-up, 11 months), while two patients in the PDD-cTURBT group had Ta low-grade recurrent tumors (8 months). Postoperatively, scores of daytime frequency and nocturia were increased in both groups. QoL assessment using the FACT-BL and SF-8 revealed that postoperative deterioration of bladder-specific subscale and emotional/mental scores was found in the EBTUR group but not in the cTURBT group.
Conclusions:
Based on the initial experience on 12 patients, we considered that PDD-EBTUR is an acceptable surgical method. Further experience and research are mandatory to determine whether this technique yields better outcomes and has true clinical advantage.
Introduction
Transurethral resection of bladder tumor (TURBT) is the mainstay of treatment, diagnosis, and staging in bladder cancer, especially in nonmuscle invasive bladder cancer (NMIBC). 1 Pathologic examination on fragmented and heat-denatured specimens obtained by conventional TURBT (cTURBT) can be inaccurate and difficult, resulting in understaging and interobserver variability, largely due to poor anatomic orientation and indistinguishable muscularis propria from muscularis mucosae. 2 This drawback inherent in cTURBT could be overcome by tumor resection in one piece with intact surrounding normal tissues. Since the first report by Kawada and colleagues in 1997, the usefulness and safety of en bloc TURBT (herein referred to as “EBTUR,” also known as “TURBT in one piece, TURBO” 3 ) have been reported by several publications. 3 –9
The main purpose of developing the EBTUR technique is to not only conduct accurate pathologic assessment but also improve oncologic outcome without compromising safety. It is considered that intravesical recurrence (IVR) after surgery is largely attributed to dissemination of cancer cells and consequent seeding to the bladder mucosa. 10 This phenomenon is inevitable in cTURBT during resection and fragmentation of the tumor, while it could be minimized in EBTUR. Among several prospective and retrospective studies, only one prospective randomized controlled trial (RCT) was reported so far. This RCT failed to show any significant clinical advantage of EBTUR. 6 Two prospective studies 7,8 reported by an Indian group focused on yield of detrusor muscle on EBTUR and IVR after TURBT as the primary end point, respectively. The latter confirmed a significantly longer IVR-free survival, not progression-free survival, in the EBTUR group compared to that in the cTURBT group (45.1 vs 28.5 months, p = 0.018). 8 The clinical evidence regarding oncologic outcomes is still limited in this field.
One of the unsolved problems underlying EBTUR is the variation in technique, procedure, resection device, and extraction method of dissected specimens. Particularly, circumferent demarcation around the bladder tumor depends on the surgeon's preference and has not been established. Recently, the clear benefit of photodynamic diagnosis (PDD)-assisted TURBT using 5-aminolevulinic acid (5-ALA) has been confirmed by RCTs and meta-analyses. 11 Based on favorable evidence, oral 5-ALA was approved as an intraoperative diagnostic drug in Japan during December 2017. 12
In this study, we reported that PDD guidance could be useful and helpful for the decision of intraoperative circumferent demarcation around the bladder tumor. Furthermore, we hypothesized that PDD-EBTUR could suppress dissemination of cancer cells to bladder cavity compared to cTURBT. This study described a novel technique, PDD-assisted EBTUR (PDD-EBTUR) with a rectangular cutting loop, and evaluated the short-term IVR rate, complication, and postoperative health-related quality of life (QoL) compared with PDD-assisted cTURBT (PDD-cTURBT) in NMIBC.
Methods
Clinical data and follow-up
This study was approved by the Ethics Committee of the Nara Medical University, and all participants provided informed consent (reference ID: 1719 and 1966). Informed consent to participate in the study was obtained from all participants. The study was conducted in compliance with the study's protocol and in accordance with the provisions of the Declaration of Helsinki (2013).
All patients found to have bladder tumor underwent white-light flexible cystoscopy at the outpatient clinic, dynamic contrast-enhanced CT, and/or MRI before PDD-EBTUR or PDD-cTURBT. The main exclusion criteria were radiographically muscle invasive disease (suspected T2–T4 disease) and contraindications for oral administration of 5-ALA. Random or target biopsy was added when there were any lesions suspected for carcinoma in situ (CIS). Visibly complete resection was achieved in all patients by PDD-TURBT.
Surgical procedure and device for PDD-EBTUR
Surgical procedures of PDD-EBTUR were performed by a single surgeon (M.M.). Approximately 3 hours (range, 2–4 hours) before surgery, patients orally received a water-dissolved 5-ALA solution at a dose of 20 mg/kg (ALAGLIO®; Chugai Pharmaceutical Co., Ltd., and SBI Pharmaceuticals Co., Ltd.). EBTUR was performed using a bipolar 26F resectoscope (KARL STORZ Endoscopy Japan) with a rectangular cutting loop (Fig. 1a). The Storz Professional Image Enhancement System (IMAGE1 S™) was utilized for the visualization of tumors during surgery. This system provides a white light, blue light (fluorescence cystoscopy), and imaging enhancement modes, such as spectra A, spectra B, chroma, and clara. 11
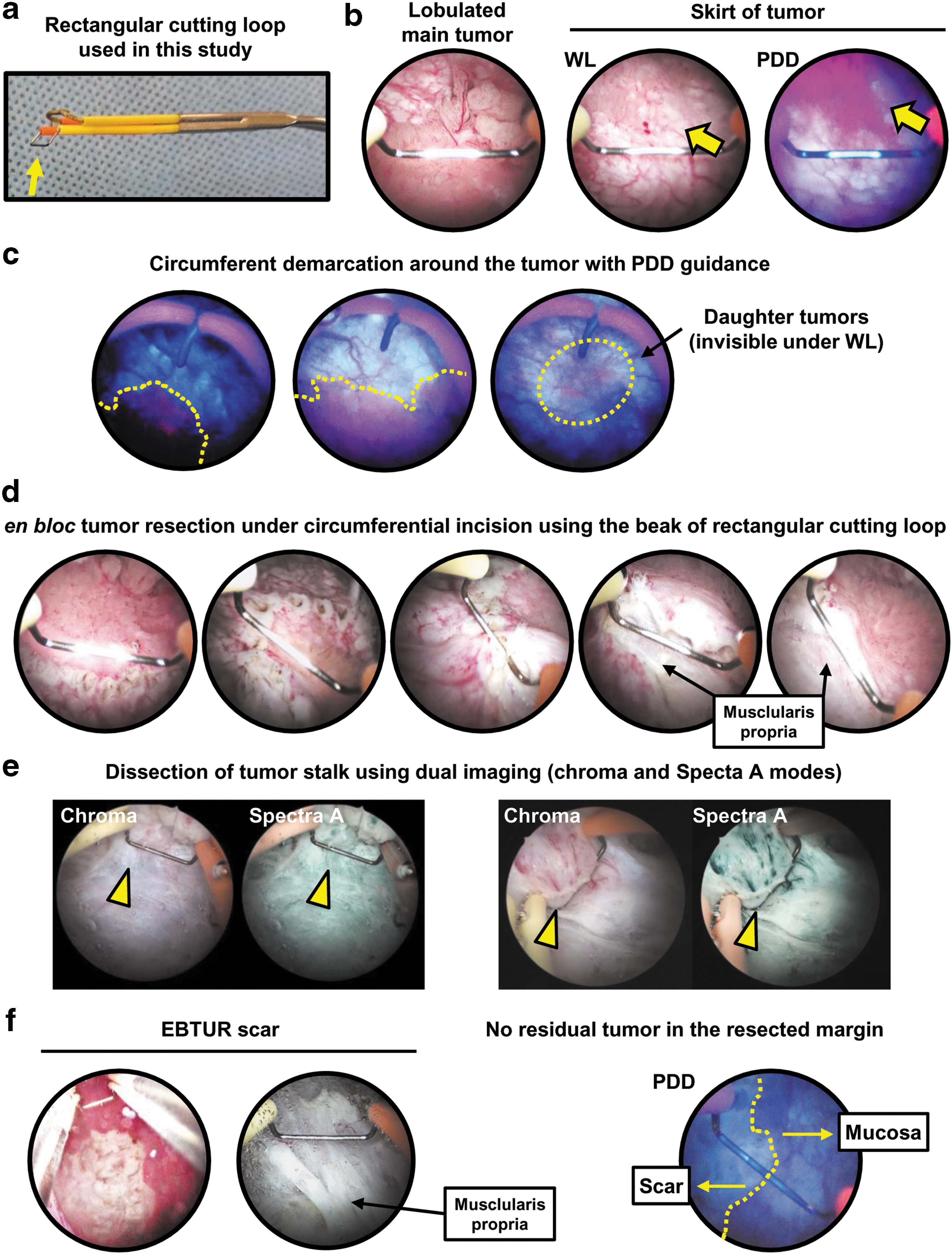
Procedure of PDD-EBTUR.
Under general or spinal anesthesia, careful examination of the entire bladder mucosa with white and blue light modes was conducted (Fig. 1b) according to the previous phase III trial. 12 The effect setting was set to 3 for cutting and 4 for coagulation in the bipolar cautery system (AUTOCON® III 400; KARL STORZ Endoscopy Japan). Physiologic saline was used as an irrigant during surgery. First, the tumor was demarcated circumferentially in the normal urothelium with PDD guidance, and the point markings were connected using a pointed cutting electrode (Fig. 1c and Supplementary Movie S1) or rectangular cutting loop (Supplementary Movies S2 and S3). Bladder cancer is characterized by growth with a skirt of tumor and small daughter tumors. When setting margins of resection, these occult tumors are often missed under the white light mode but captured under the blue light mode. Superficial blood vessels feeding the tumor were coagulated first. En bloc tumor resection was initiated through the superficial muscularis propria under circumferential incision (Fig. 1d). The tumor base was lifted off using the beak of rectangular cutting loop (Fig. 1e). After the tumor was dissected with the surrounding normal tissues and muscularis propria, we confirmed no residual tumor in the resected margin with PDD guidance (Fig. 1f).
The dissected specimens were extracted using grasping forceps through the lumen of the 26F resectoscope sheath and subjected to pathologic processing. If specimens were too large to be extracted through the resectoscope, the papillary-growing portion was superficially cut by TUR to avoid disrupting the tumor base architecture.
Tissue processing and pathologic diagnosis
The dissected specimens were immediately stretched with 27G needles close to the original shape and fixed in 10% neutral buffered formalin. The fixed specimens were serially sectioned at 2- to 3-mm intervals and embedded into paraffin. Well-oriented histologic sections were stained with hematoxylin and eosin and subjected to histologic examination by an experienced uropathologist (T.F.). Pathologic diagnosis of the specimens was made to determine T categories (2009 Union for International Cancer Control TNM Staging System), tumor grades (1973 and 2004 World Health Organization [WHO] classifications), and presence of CIS.
Surgical procedure and device for PDD-cTURBT
The preoperative process for administration of ALA, anesthesia, resection device, and imaging device for PDD-cTURBT was same as used for PDD-EBTUR. Initial circumferent demarcation with PDD guidance was not routinely performed in PDD-cTURBT. Instead, we switched imaging modes of white light and blue light frequently during the operation to set the resection margin. TUR of all the visible tumors accompanied with or without cold cup biopsy was performed according to the surgical method previously described. 1,12
Adjuvant therapy and follow-up
Basically, a second TUR was indicated if high-grade Ta or T1 was pathologic detected or there was no adequate muscularis propria in the specimen. Whether second TUR was performed or not depended on judgment of the physician. Adjuvant therapy depended on the physician's preference but was mostly performed as follows: single immediate instillation of epirubicin or pirarubicin for low-risk NMIBC, intravesical Bacillus Calmette–Guerin (BCG; Immunobladder®, Tokyo-172 strain) induction (6–8 doses weekly) for intermediate NMIBC, and BCG induction followed by BCG maintenance (1–3 years) for high-risk NMIBC.
Patients were followed up according to our institutional protocol as previously described. 1 Briefly, cystoscopy with urine cytology was performed every 3 months for 2 years, every 6 months for the subsequent 3 years, and annually thereafter. Recurrence of pelvic and upper urinary tract was checked using CT every 6 or 12 months. IVR and progression were defined as previously described. 1
European Organisation for Research and Treatment of Cancer and Japanese Nishinihon uro-oncology extensive collaboration group tables for NMIBC risk stratification
Both the European Organisation for Research and Treatment of Cancer (EORTC) 13 and Japanese NIshinihon uro-onCology Extensive collaboration group (J-NICE) 14 risk tables for IVR incorporated six parameters (Supplementary Table S1) to categorize patients into risk groups according to the summed scores. These score models were applied to our cohort to calculate each patient's risk for IVR after TURBT.
Perioperative complications and postoperative QoL
Perioperative complications were objectively evaluated using the Clavien-Dindo classification system. 15 This system consists of seven grades (I, II, IIIa, IIIb, IVa, IVb, and V). The assessment of postoperative QoL was based on patient reported outcome measures, including the 8-item Short Form (SF-8™), Functional Assessment of Cancer Therapy-Bladder (FACT-BL), 16 and the International Prostate Symptom Score (IPSS) questionnaires before and 1 month after TUR.
Statistical analyses
Prism software version 7.00 (GraphPad Software, Inc., San Diego, CA) was used in the statistical analyses and data visualization. Fisher's exact test or Mann–Whitney U test was applied to compare the background between PDD-EBTUR and PDD-cTURBT. IVR-free survival was estimated using Kaplan–Meier analysis and compared using log-rank test in the two groups. Postoperative changes in QoL were evaluated using the Wilcoxon signed-rank test. A p-value <0.05 was considered statistically significant.
Results
Surgical movies of three representative cases are uploaded in Supplementary Movies S1 to S3. The circumferent demarcation was made with PDD guidance using a pointed cutting electrode (case 1) or rectangular cutting loop (cases 2 and 3). The tumor was located on the left wall close to the left ureteral orifice in cases 2 and 3. The EBTUR technique seems to prevent damage of the ureteral orifice and intramural ureter due to minimized tissue coagulation. Active urine efflux could be confirmed after intravenous injection of indigo carmine.
From October 2018 to September 2019, 69 consecutive patients found to have NMIBC underwent PDD-assisted TURBT in our hospital. Of 69 patients, 12 (17%) and 57 (83%) underwent PDD-EBTUR and PDD-cTURBT, respectively. None of the 12 patients undergoing PDD-EBTUR received intravesical BCG treatment postoperatively. To minimize the difference in the patient background, we excluded 29 (51%) patients receiving intravesical BCG treatment due to the presence of CIS lesion from 57 patients undergoing PDD-cTURBT, leaving 28 patients (Fig. 2). The clinicopathologic background between PDD-EBTUR (n = 12) and PDD-cTURBT (n = 28) is compared and presented in Table 1. None of the variables, including histology, tumor size, and risk stratification, showed significant difference between the two groups. One female patient in the PDD-EBTUR group had grade II bladder perforation requiring prolonged catheterization (for 7 days). The other 39 patients did not have any complications of grade II or higher.
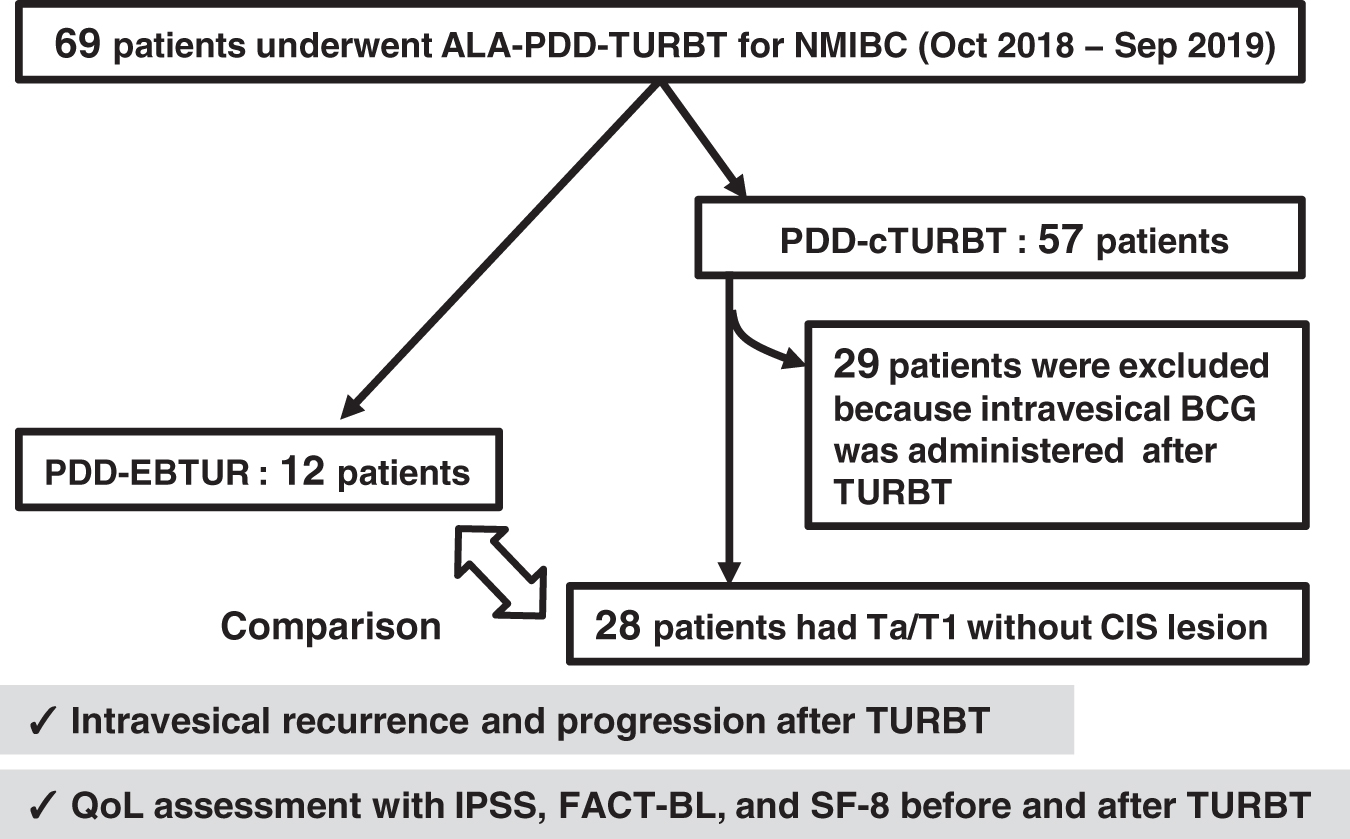
Flowchart of the patient's cohort dataset. ALA, aminolevulinic acid; CIS, carcinoma in situ; cTURBT, conventional TURBT; EBTUR, en bloc TURBT; FACT-BL, Functional Assessment of Cancer Therapy-Bladder; IPSS, International Prostate Symptom Score; OABSS, overactive bladder symptom score; QoL, quality of life; TURBT, transurethral resection of bladder tumor.
Characteristics of Patients Undergoing Photodynamic Diagnosis-Assisted Transurethral Resection of Bladder Tumor and Comparison Between En Bloc Transurethral Resection of Bladder Tumor and Conventional Transurethral Resection of Bladder Tumor
cTURBT = conventional transurethral resection of bladder tumor; EAU = European Association of Urology; EORTC = European Organisation for Research and Treatment of Cancer; HG = high-grade; IQR = interquartile range; J-NICE = Japanese Nishinihon uro-oncology extensive collaboration group; LG = low-grade; PDD = photodynamic diagnosis; PDD-EBTUR, photodynamic diagnosis-assisted en bloc transurethral resection of bladder tumor; SD = standard deviation; TURBT, transurethral resection of bladder tumor; WHO = World Health Organization.
Representative data of tissue processing are shown in Figure 3. Well-oriented histologic sections were obtained by EBTUR (Fig. 3a, b), while cTURBT yielded fragmented tumor specimens with poor anatomic orientation (Fig. 3c). This drawback is associated with interobserver variability and understaging in pathologic diagnosis. EBTUR successfully diagnosed a T1 high-grade tumor that invaded the deep area of the lamina propria but not the muscularis propria (Fig. 3d). Pathologic assessment of the horizontal and vertical margins in resected specimens by PDD-EBTUR revealed that all specimens had muscularis propria, and the rate of en bloc resection was 100%. Accurate T category can be diagnosed only when resected specimens include appropriate muscularis propria with negative vertical margin.
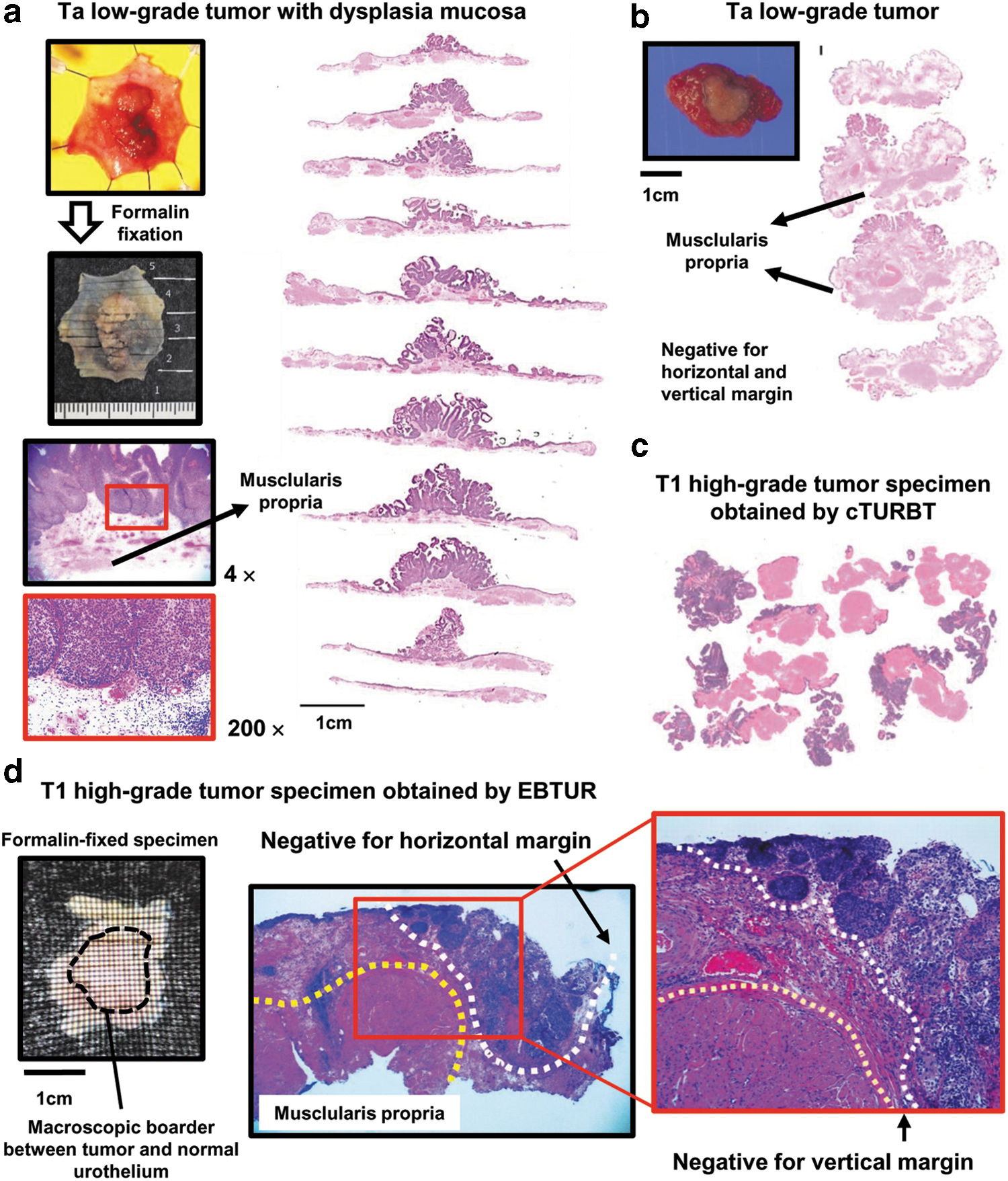
Tissue processing and pathologic diagnosis in EBTUR.
The median follow-up period was 11 and 8 months in the PDD-EBTUR and PDD-cTURBT groups, respectively. No patient had IVR in the PDD-EBTUR group, while two patients had Ta low-grade recurrent tumors at 10 and 16 months after initial TURBT in the PDD-cTURBT group (Fig. 4a). Progression to muscle invasive disease was not noted in any patient.
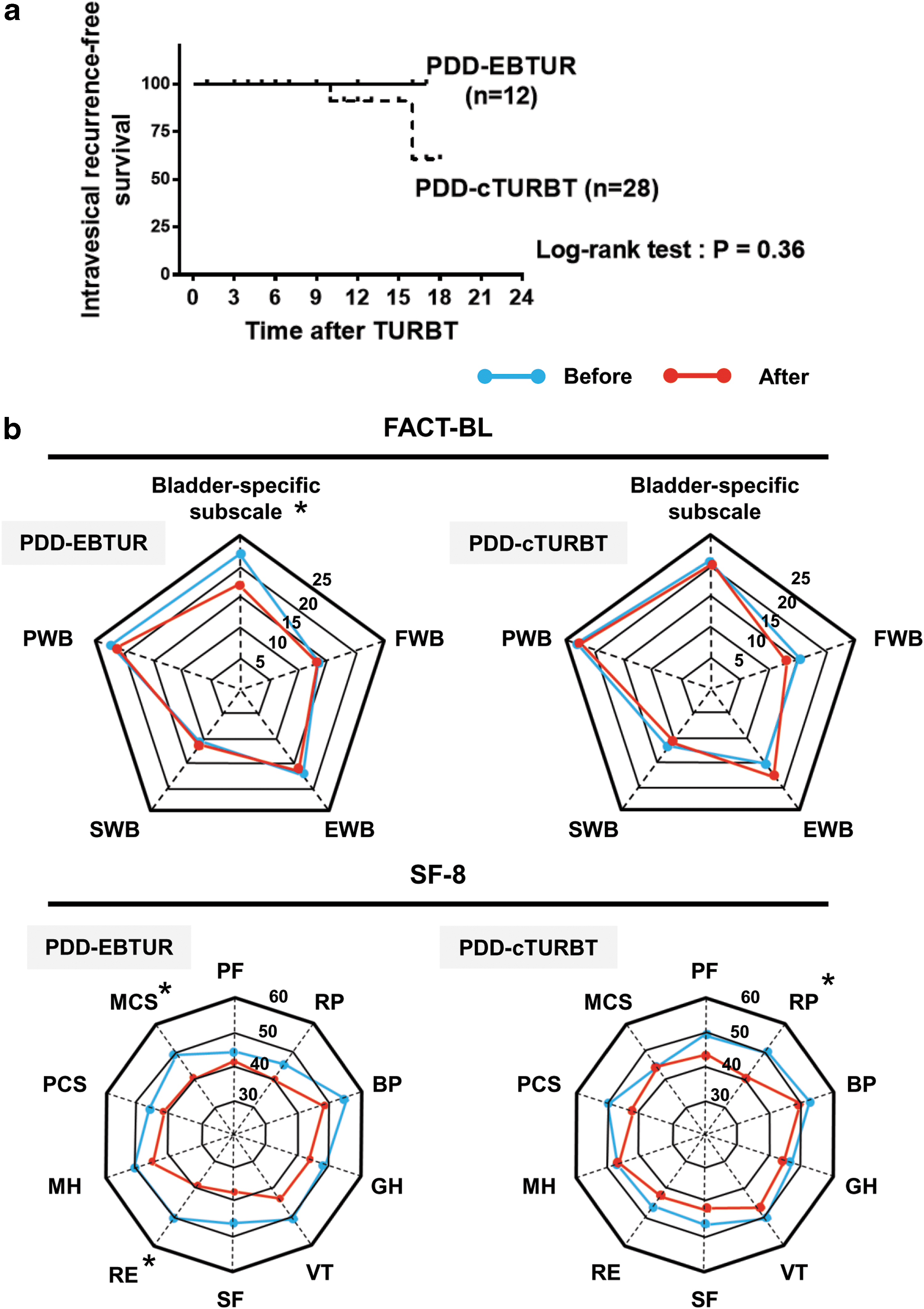
Comparison of intravesical recurrence rate and QoL assessment between the PDD-EBTUR and PDD-cTURBT groups. Intravesical recurrence-free survival after TURBT was compared between the two surgical techniques.
The postoperative changes in the seven IPSS parameters, voiding and storage subscores, and total IPSS are summarized in Table 2. Elevated scores of frequency (question 2) and nocturia (question 7) were observed in the PDD-EBTUR group, whereas only the nocturia score was increased in the PDD-cTURBT group. Assessment of FACT-BL revealed that most domains did not change postoperatively; however, a significant decrease in the bladder-specific subscale was observed in the PDD-EBTUR group (Fig. 4b, upper panels, and Supplementary Table S2). Changes in the eight domains and two summary scores from the SF-8 survey are summarized in Supplementary Table S2. While all domains and scores showed a decrease to some degree postoperatively (Supplementary Table S3), there was a significant change noted in the two scores (role limitation because of emotional problems and mental component summary) in the PDD-EBTUR group and one score (role limitation because of physical problems) in the PDD-cTURBT group (Fig. 4b, lower panels).
Changes in the International Prostate Symptom Score After Transurethral Resection of Bladder Tumor and Comparison Between Two Surgical Techniques
Data are expressed by mean ± SD and compared between “Before” and “After” (∼1 month) with Wilcoxon signed-rank test. A high score indicates more severe symptoms.
Values in bold indicate statistically significant.
IPSS = International Prostate Symptom Score.
Discussion
We described the surgical technique of PDD-EBTUR using a rectangular cutting loop with its oncologic and functional outcomes. Various types of electrocautery such as standard loop, 45° to 90° bended loop, J-shaped electrode, Collins loop, and snare were utilized for EBTUR so far. 2 To the best of our knowledge, this was the first study to address the utility and safety of the rectangular cutting loop. Surgical procedures of PDD-EBTUR were performed by a single surgeon in this study. The surgeon would say that this endoscopic method would be easy and reproducible in any of the urologists. Previous studies have reported the advantages of EBTUR, including accurate pathologic assessment and decreased risk of IVR through suppressed dissemination of cancer cells to bladder cavity. 2,3,8 Bladder cancer is characterized by an ambiguous border between the tumor and normal urothelium and white light-undetectable daughter lesions scattered around the main tumor. Therefore, PDD guidance provided substantial help for circumferent demarcation around the bladder tumor, which precedes tumor dissection. In this study, all dissected tumors by PDD-EBTUR were negative for horizontal and vertical margin, indicating that the rate of both en bloc resection and incidence of the muscularis propria in the specimens was 100%.
The systematic review of 544 patients with NMIBC treated with EBTUR demonstrated that the IVR rate was 23% (range, 6%–55%) in 20 months of mean weighted follow-up duration. To date, two RCTs compared IVR after TUR between EBTUR and cTURBT. 6,8 Chen and coworkers evaluated the practicability of 2 μm continuous-wave laser in EBTUR. Notably, obturator jerk occurred in 18 (25%) of 71 patients undergoing cTURBT, whereas none was noted in patients undergoing EBTUR with laser resection. However, EBTUR did not decrease the IVR rate. Another RCT demonstrated that EBTUR with 45° to 90° bended loop decreased the IVR rate compared to the cTURBT. Although our study did not show a significant difference in the IVR rate between the two groups, we cannot draw a conclusion because the sample size was extremely small in our cohort. The clinical evidence regarding oncologic outcomes is still limited in this field.
Maximal effort should be made to ameliorate postoperative urinary symptoms and deterioration of QoL even though they are transient. Tan and colleagues reported that patients found to have NMIBC are most psychologically affected during the period between initial diagnosis by cystoscopy and TURBT. 17 The functional patient-reported outcomes after TURBT, especially in EBTUR, have been rarely investigated. We focused on the difference in worsening of urinary symptoms and deterioration of health-related QoL between the EBTUR and cTURBT groups. Although an increase in the nocturia score (IPSS 7) was common in the two groups, the score of daytime frequency (IPSS 2) increased only in the EBTUR group. We speculated that resection of the deeper layer of the bladder wall, wider range of the bladder mucosa, and longer operative time in EBTUR compared with those in cTURBT might be associated with difference in worsening of urinary symptoms. Besides, a unique finding was noted in QoL assessment. A decrease in emotional and mental scores was noted in the EBTUR group but not in the cTURBT group. One of the possible interpretations would be that postoperative urinary problems, including frequent urination, nocturia, and bladder irritability, affect mental health. Further study with a larger sample size may elucidate the importance of QoL assessment in patients undergoing EBTUR.
The present study has several limitations. There is a potential selection bias because the decision between the EBTUR and cTURBT groups was made based on the physician's preference rather than randomization. Second, the sample size is small, only 12 patients in the EBTUR group, with a short follow-up duration. Finally, follow-up assessment and recovery regarding patient-reported outcome was not monitored.
Conclusion
Effective management of NMIBC depends on complete resection and accurate pathologic diagnosis. Based on the initial experience on 12 patients, we considered that PDD-EBTUR is a simple, easy, safe, and acceptable surgical method. Further experience and research are mandatory to determine whether this technique yields better outcomes and has true clinical value.
Footnotes
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of the Nara Medical University (reference ID: 1719 and 1966). Informed consent to participate in the study was obtained from all participants. The study was conducted in compliance with the study's protocol and in accordance with the provisions of the Declaration of Helsinki (2013).
Acknowledgment
The authors thank Editage for English language editing.
Author Disclosure Statement
M.M., N.T., and K.F. have received a research fund from SBI Pharmaceuticals Co., Ltd., that produces 5-aminolevulinic acid, ALAGLIO. Other authors do not have any competing financial interests.
Funding Information
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article, or in the decision to publish the results.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Movie S1
Supplementary Movie S2
Supplementary Movie S3
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.