
Abstract
Introduction:
The most common cause of acute renal colic is a ureteral obstruction caused by ureterolithiasis. Urgent intervention is often necessary due to intractable pain. Early extracorporeal shockwave lithotripsy (SWL) as an alternative treatment option to ureteral stenting becomes forgotten in times of rising ureterorenoscopy. However, definitive guidelines are lacking, in which urgent treatment should be preferred in the absence of signs of infection. Therefore, we assessed efficacy and safety of early SWL (eSWL) to secondary SWL (sSWL) after urgent ureteral stenting.
Patients and Methods:
One hundred four patients treated between January 2015 and November 2017 for obstructive ureterolithiasis were matched regarding stone size, stone localization, and assigned to group eSWL (n = 52) or group sSWL (n = 52). The eSWL group received shock waves (without prior ureteral stenting) and sSWL group ureteral stenting within 48 hours from diagnosis. Thereafter, patients in group sSWL were treated with shock waves for a median of 23 ± 14.6 days after ureteral stenting. Stone-free rates, complication rates, and reintervention rates were assessed. Univariable and multivariable logistic regression was applied to find predictors of outcomes in the two treatment groups.
Results:
Overall, there was no statistically significant difference between both groups regarding stone-free rate and complication rate. Reinterventions were more often addressed for patients in group sSWL (p = 0.05). eSWL was significantly superior to sSWL regarding stone-free rates for stones between 6 and 9 mm (p = 0.04). At the multivariable multinomial logistic regression none of the two treatment modalities was associated with better outcomes. A body mass index ≥30 was associated with a reduced 6-week stone-free status (p = 0.04), whereas stones ≥8 mm were associated with an increased need of reintervention (p = 0.04).
Conclusion:
eSWL seems to be an effective and safe emergency procedure compared with sSWL after urgent stenting within 6 weeks and should be considered as a treatment option in patients without absolute indications for immediate ureteral drainage. Clinical trial registration number: 2019-00155.
Introduction
Ureteral and pyeloureteral urolithiasis have a high prevalence among urologic emergency patients and leads to renal colic caused by ureteral obstruction. 1 These patients can be treated by different procedures due to the individual situation. Absolute indications for an urgent ureteral drainage are patients with obstructing ureteral stones and acute urinary tract infection or urinoma as well as anuria because of a single kidney. 2 However, even in the absence of these indications a ureteral drainage is often used as primary procedure in patients with analgesic noncompensable colic pain.
In general, stones ≤4 mm can be treated by medical (expulsion) therapy. Patients with larger stones or with colics refractory to medication therapy can be treated by one of the following options: draining the collecting system by Double-J stent (or percutaneous nephrostomy [PCN]) followed by secondary ureterorenoscopy (URS) or extracorporeal shockwave lithotripsy (SWL), early or delayed SWL, and early or delayed URS. Important factors predicting the selection of the abovementioned therapeutical options are stone location, stone size, stone density, patients' comorbidities, as well as patients' preference in cases with more than one equal treatment option. 3 In general, SWL can be recommended for stones located in the upper and middle pole of the kidney, as well as the proximal or distal ureter. 2 Picozzi et al. considered early SWL (eSWL) to be a safe and effective primary procedure. 4 SWL as an urgent procedure in patients with acute colic pain can lead to quick pain relief and can lower stone-related morbidity. 5
From our point of view, the main disadvantages of a primary ureteral drainage are stent-induced discomfort or complications (irritative bladder symptoms, hematuria, flank pain, or bacteriuria 6 ) and the need for a secondary stone therapy with increased anesthesia/procedure-derived risks and increased health-related costs. On the other hand, immediate ureteral drainage leads to rapid pain relief while patients after SWL are at risk of a recurrent colic in 2% to 4% of cases. 7 However, guidelines are unclear regarding an urgent treatment of ureteral and pyeloureteral urolithiasis.
The aim of our study is to assess whether early SWL within 48 hours and secondary SWL (sSWL) after emergency ureteral stenting within 48 hours show different efficacy and safety outcomes.
Patients and Methods
Study population
Patients treated for an obstructive urolithiasis between January 2015 and November 2017 were retrospectively screened for their primary procedure using the clinical electronic health record system of our hospital (EPIC hyperspace, EPIC System Corporation®).
A total of 104 patients with ureterolithiasis who underwent either eSWL (without ureteral stenting) or sSWL after urgent ureteral drainage within 48 hours after first presentation at the emergency department were included. Patients were matched regarding stone size (≤5; 6–9; > 10 mm) and stone location (proximal or distal ureter) and grouped regarding their primary surgical procedure into eSWL (n = 52) or sSWL (n = 52). Subanalysis was performed for stone size and stone localization.
Diagnosis of urolithiasis was made by unenhanced CT and abdominal X-Ray, measuring the largest available stone diameter each time. All patients were afebrile and had no signs of infection in blood and urinary analysis. Excluded from the study were patients with previous surgical treatment for the same calculi, ureteral pathologies, or clotting disorders.
SWL was performed using the Storz Modulith Lithotripter at a shockwave rate of 60 to 90 Hz. A maximum number of 3000 shockwaves and a maximum energy of 9 were delivered in each session for patients with ureteral stone disease, whereas patients with pyeloureteral stones received a maximum of 2500 shockwaves and a maximum energy level of 7. A precise focus was selected until (partial) fragmentation was observed. The treatment was then continued with an extended focus to ensure optimal fragmentation. All patients were treated under a need-based sedoanalgesia by the colleagues in Anesthesia (intravenous Metamizol, nonsteroidal anti-inflammatory drugs and opioids). Ureteral drainage was performed under general anesthesia by insertion of a 6F Double-J stent for all patients in the sSWL group. Stent removal was carried out routinely 6 weeks after sSWL in our outpatient clinic under local anesthesia (Instillagel®) and was not included in our evaluation as an independent intervention.
After SWL, patients of both groups received a standard needs-based analgesic therapy with Metamizol and Diclofenac, as well as an expulsive treatment with Tamsulosin for a maximum duration of 6 weeks. A follow-up visit routinely took place 6 weeks after eSWL or sSWL and stone passage was assessed by abdominal X-ray and ultrasound. Any residual fragment detected during the follow-up visit was considered as SWL failure. Complications were assessed according to the Clavien–Dindo classification. 8
Primary and secondary endpoints
Primary endpoint was defined as stone-free rate 6 weeks after eSWL or sSWL. Secondary endpoints were complications and the reintervention rate within the observation period of 6 weeks.
Statistical analysis
Descriptive statistics are reported as mean ± standard deviation. Normal distribution was tested using the Shapiro–Wilk test. To compare independent variables, Student's t-test and Fisher's Exact test were addressed. A conventional p-value of ≤0.05 was considered as statistically significant. For the prediction of stone-free rates, reintervention and complication-dependent variables were tested by univariable and multivariable logistic regression. Statistical analysis was carried out with Prism GraphPad Version 7.0 (GraphPad Software, La Jolla, California).
This study was approved by the national research committee “Ethikkomission Nordwest- und Zentralschweiz” under the registry 2019-00155. We hereby confirm that all methods were performed in accordance with the relevant guidelines and regulations.
Results
Patients and stone data are shown in Table 1. After propensity match scoring, 52 patients treated by eSWL and 52 by sSWL after urgent ureteral Double-J stenting due to analgesic noncompensable flank pain were obtained. Eighty patients (78%) were male, 24 patients (22%) female. The mean age was 48.1 ± 14.9 years in the eSWL group and 54.6 ± 13.2 years in the sSWL group. The mean stone size was 7 mm (range: 5–12 mm) in both study groups; 70% of stones were located in the proximal ureter (n = 40) and 30% in the distal ureter (n = 12) in both study groups. The mean time from patients' first presentation at the emergency department until initial procedure was 20.3 ± 13 hours for the eSWL group and 13.3 ± 7.1 hours for the sSWL group. The mean time between ureteral stenting and sSWL was 23 ± 14.6 days. sSWL was carried out with Double-J stent in situ for all patients.
Patient and Stone Characteristics of Matched Pairs (eSWL vs sSWL)
BMI = body mass index; eSWL = early SWL; HUmax = maximal Hounsfield Units; SWL = extracorporeal shockwave lithotripsy; sSWL = secondary SWL.
Overall, we did not find any significant difference between eSWL and sSWL regarding stone-free rate and complication rate. Thirty-two out of 48 patients (67%) in group eSWL and 22/45 patients (49%) in group sSWL were stone free after 6 weeks (p = 0.10) (Fig. 1A). Clavien–Dindo Grade 1 and 2 complications occurred in 17/51 (33%) cases of the eSWL group and in 18/52 (35%) cases of the sSWL group (p > 0.99) (Fig. 1B). In group eSWL 16/17 patients (94%) needed additional brief analgesic therapy (oral opioids), which is classified as Grade 1 complications according to the Clavien–Dindo classification. One case of postinterventional fever was recorded (Clavien–Dindo Grade 2). In group sSWL 16/18 patients (89%) needed additional brief opioid therapy (Clavien–Dindo Grade 1) and 2 cases of fever occurred (Clavien–Dindo Grade 2). No Clavien–Dindo Grade 3 to 5 complications and no renal hematomas were reported in both groups.
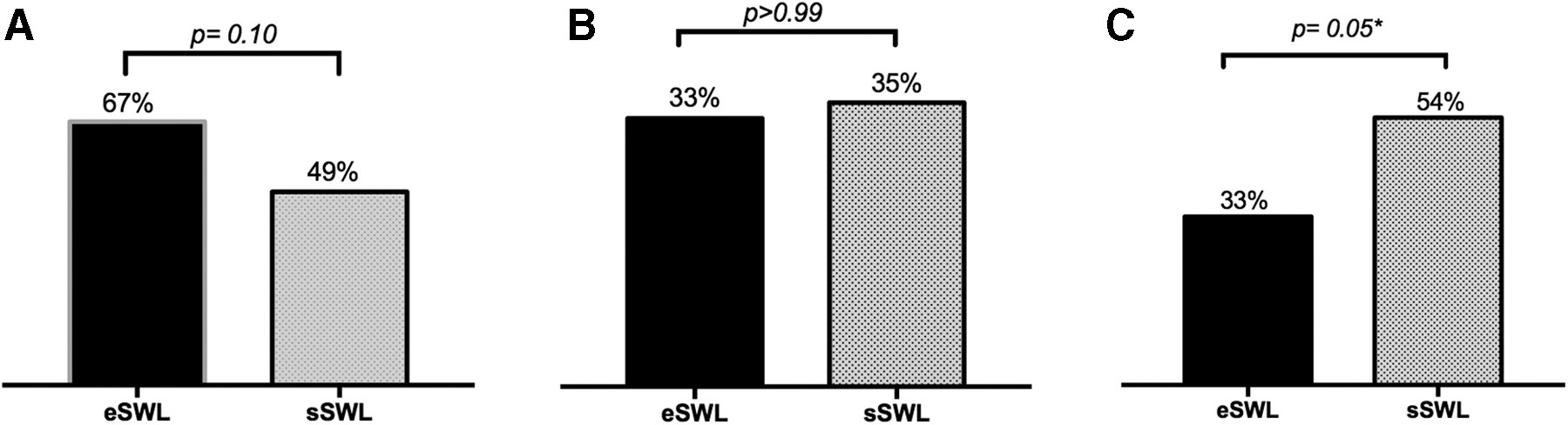
Reintervention rate was significantly higher in group sSWL (p = 0.05). A total of 17/51 patients (33%) in group eSWL and 27/50 patients (54%) in group sSWL needed a reintervention due to stone persistence and/or recurrent flank pain (Fig. 1C). No case of postinterventional ureteral stenting was reported in the eSWL group. Reinterventions consisted either of repeated SWL or secondary URS. The mean number of total procedures until stone-free status was achieved was n = 84 in group eSWL and n = 132 in group sSWL, respectively.
In patients after eSWL, 8/17 reinterventions (47%) were carried out as a second SWL session. Five out of eight patients (62.5%) were stone free after their second SWL session. Three out of eight patients (37.5%) had to undergo secondary URS after ureteral drainage due to stone persistence. Nine out of 17 patients (53%) received a secondary URS after elective Double-J stent placement without undergoing a second SWL session.
Interestingly, in group sSWL secondary URS was carried out in 14/27 patients (52%), whereas a repeated SWL was still performed in 13/27 patients (41%). All 14 patients who underwent secondary URS after initial SWL failure were stone free afterward. Out of 13 patients who underwent a second SWL session, 1 patient needed further treatment by URS after pigtail insertion due to stone persistence.
The subgroup analyses are reported in Tables 2 and 3. Patients with 6 to 9 mm stones reached a significantly higher stone-free rate after eSWL in comparison with sSWL (72% vs 45%, p = 0.04) (Fig. 2). Regarding complication and reintervention rates, no significant difference was detected within the subgroups. The reintervention rate in patients with eSWL vs sSWL was insignificantly different for stones sizes 5 mm (20% vs 50%; p = 0.35) and 6 to 9 mm (33% vs 58%; p = 0.08) and almost equal for calculi size >10 mm (50% vs 43%; p > 0.99). More minor complications were detected after sSWL when compared with eSWL (20% vs 40%; p = 0.63) in patients with stone size of 5 mm. For patients with stone sizes 6 to 9 mm (35% vs 38%; p > 0.99) and ≥10 mm (38% vs 13%; p = 0.57), complication rates were almost equal or slightly lower for group sSWL (Table 2).

When compared to sSWL, *stone-free rates are significantly higher in patients underwent eSWL for calculi sized 6–9 mm (p = 0.04).
Stone-Free, Complication, and Reintervention Rate Depending on Stone Size in Patients After eSWL and sSWL
Significant result.
Stone-Free, Complication, and Reintervention Rate Depending on Stone Localization in Patients After eSWL or sSWL
In addition, subanalysis for stones in the proximal or distal ureter showed no significant difference between both groups regarding stone-free rate, complication rate, and reintervention rate. Stone-free rate after 6 weeks was slightly higher for patients treated with eSWL for calculi located in the proximal (61% vs 43%; p = 0.16) or the distal ureter (83% vs 70%; p = 0.62), whereas reintervention rate was higher for stones in the proximal (36% vs 53%; p = 0.17) and distal ureter (25% vs 58%; p = 0.21) in the sSWL group. Primary ureteral drainage before SWL is associated with an insignificant increase of minor complications for calculi located in the distal ureter (42% vs 58%; p = 0.68) but not for calculi located in the proximal ureter (33% vs 28%; p > 0.99) (Table 3).
At univariable logistic regression analysis, only stone localization of the distal ureter was significantly associated with stone-free rates after 6 weeks (odds ratio [OR] 3.12; 95% confidence interval [CI] 1.04–9.39; p = 0.04). At multivariable logistic regression analysis, a body mass index (BMI) ≥30 kg/m2 was found to be an independent predictor of a lower stone-free rate after 6 weeks after SWL (OR 0.18; 95% CI 0.03–0.98; p = 0.04) (Table 4). Multivariable logistic regression showed also that stone diameters ≥8 mm are significantly associated with a higher reintervention rate (OR 3.45; 95% CI 1.01–11.91; p = 0.04) (Table 5), whereas none of the variables tested was able to predict a high risk of complications (Table 6).
Univariable and Multivariable Logistic Regression Analyses for the Prediction of Stone-Free Status in Patients Who Underwent Immediate (eSWL) vs Delayed (sSWL) Shockwave Lithotripsy
A BMI ≥30 kg/m2 significantly predicts a lower stone-free rate 6 weeks after SWL (p = 0.04).
CI = confidence interval; OR = odds ratio.
Univariable and Multivariable Logistic Regression Analyses for the Prediction of Need of Reintervention in Patients Who Underwent Immediate (eSWL) vs Delayed (sSWL) Shockwave Lithotripsy
Stone sizes ≥8 mm are associated with a significantly higher probability for auxiliary procedures after SWL (p = 0.04).
Univariable and Multivariable Logistic Regression Analyses for the Prediction of Complications in Patients Who Underwent Immediate (eSWL) vs Delayed (sSWL) Shockwave Lithotripsy
Discussion
Acute flank colic due to obstructive ureteral calculi can be treated depending on stone size and location conservatively, by Double-J stenting, nephrostomy, ureteroscopy, or SWL. Double-J stents are widely used as a primary procedure. First introduced in 1980, SWL became a standard treatment option for patients with ureteral or renal calculi especially due to its noninvasive nature, low morbidity, and high efficacy. In our study, we focused on early SWL and delayed SWL after urgent ureteral stenting. Our data suggest that eSWL, compared with urgent ureteral stenting and sSWL, is more effective and leads to fewer reinterventions.
Although many institutions used early SWL since years, in 1999 Joshi et al. 9 proposed SWL in this setting for the first time. The comparative retrospective analysis of 82 patients showed in situ eSWL superior to ureteral drainage or nephrostomy placement with following in situ SWL. The median success rate after eSWL was 89% compared with 70% after Double-J stenting and 54% after placement of a PCN. In our study overall stone-free rate of eSWL (67%) within 6 weeks was lower than reported for in situ SWL but still insignificantly superior when compared with sSWL (49%). Previously Double-J stenting was furthermore associated with a significantly higher probability of reinterventions in our cohort. The higher reintervention rate might be explained by a lower effectiveness in stone passage after SWL when the stent is in situ during the procedure compared with no stenting or PCN. 10 In line, our data support that there is no benefit of ureteral stenting in terms of complications in patients assigned for SWL in an urgent setting, although complication rates were slightly lower in patients with stones ≥10 mm undergoing sSWL. Kumar et al. 11 prospectively enrolled 160 patients comparing early SWL within 48 hours to delayed SWL (without ureteral stenting). After 3 months, the stone-free rate was 86% for early SWL and 76% for delayed SWL (p = 0.34). The mean time for stone clearance was significantly shorter within the early SWL group when compared with delayed SWL (10.2 days vs 21.1 days; p = 0.01). Supporting especially our findings on the safety profile of eSWL, a cumulative analysis identified four randomized controlled studies and two retrospective case–control studies comparing eSWL and delayed SWL. eSWL was not only superior to delayed treatment in terms of stone-free rate (OR 2.2; 95% CI 1.55–3.17; p < 0.001) but also in terms of the need of auxiliary procedures (OR 0.49; 95% CI 0.33–0.72; p < 0.001) with comparable complication rates for both techniques. Findings show high efficacy rates with a relatively low risk for complications highlighting that, in the literature, the definition for immediate treatment varies between 6 and 72 hours. 5 Regardless of ureteral stenting, time to SWL procedure is known to be relevant. Kumar et al. 11 found that a timeframe >48 hours after onset of colic pain to SWL is associated with lower stone clearance rates, higher reintervention rates, and a greater need for auxiliary procedures.
In 2008, Musa 12 published a prospective randomized series of 120 patients comparing elective SWL outcomes between patients previously stented and patients without a Double-J stent. Stone-free rates were higher in the unstented group, whereas more residual fragments were detected by X-ray within patients who received a Double-J stent before SWL. Furthermore, patients complained about typical side effects of Double-J stenting like urinary frequency, urgency pain, and hematuria. Also, in our series, Double-J stenting was associated with an insignificantly but higher risk for minor complications. This might be associated with the abovementioned well-known and common side effects of Double-J stents (e.g., flank pain and bladder irritation). 6 In line with these findings, we were able to show that in case of an urgent intervention due to intractable pain, and especially in the presence of stones, sizes up to 1 cm, ureteral stenting before SWL has no statistically significant benefit regarding stone-free rate. On the contrary, ureteral stenting was associated with a significantly lower stone-free rate in patients with stones sizes 6 to 9 mm. Besides, in our cohort, stone localization and patients' BMI predict stone-free rates, whereas greater stone dimensions are associated with a high risk of reintervention due to residual fragments along the ureter. A systematic review of eight randomized controlled trials conducted in 2011 shows only a benefit regarding the formation of Steinstrasse when a Double-J stent was previously placed, but not for stone-free rate and for the need of auxiliary treatment. 13 Another prospective randomized study of 186 patients investigating elective SWL with or without prior Double-J stenting was conducted in 2006 by El-Assmy et al. The authors described no significant benefit of prior ureteral stenting in terms of stone-free and retreatment rates. 14 Eventually our experiences in the urgent setting coincide with the evidence available on elective SWL stone treatment.
We can summarize that our data support the previously published evidence and that we were able to show that these principles also apply in the urgency setting. eSWL is efficient and safe and should be considered as a treatment option. Nevertheless, patients presenting at the emergency department often receive a Double-J stent as primary treatment to relieve the pain caused by ureteral obstruction or when SWL capacities are not available.
Despite several strengths, our study is not devoid of limitations. First of all, data have been collected retrospectively, therefore our results might suffer from the biases associated with this study design, although we tried to overcome this condition by performing a matched-pair analysis, which at least partially automatically adjusts the treatment populations for baseline characteristics. Second, the number of patients analyzed is limited and a confirmation of our findings should be performed on larger populations. Third, patients within the sSWL group were treated while the ureteral drainage was in situ. This might have led to an underestimation in sSWL efficacy as proposed by Middela et al. 10
Conclusion
We conclude that for patients presenting with obstructive ureterolithiasis, eSWL is an effective and safe alternative to primary Double-J stenting. eSWL should be considered especially for stone sizes up to 1 cm located either in the distal or proximal ureter. Prospective and randomized clinical trials are needed to validate our findings.
Footnotes
Author Contributions
J.C., L.M., H.D., A.M., and P.B. conceived the project; J.C., D.Z., and C.D.B. collected the data through the clinical operating system. J.C., L.A., S.Z., E.P., and M.M. performed the statistical analyses. J.C. and D.Z. contributed equally in the preparation of the article (co-shared first authors). All the co-authors actively contributed to interpret the data and write the article.
Author Disclosure Statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this article.
Funding Information
No funding was received.