
Abstract
Objectives:
Urolithiasis is one of the most common presentations in urological practice and it is becoming increasingly important to provide structured, simulation-based training using validated training models. This systematic review aims to identify current simulation-based training models and to evaluate their validity and effectiveness.
Methods:
Following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, a comprehensive search was performed on the Medline and EMBASE databases for English language articles published between 2000 and 2018 describing and/or assessing validity of simulation models for urolithiasis procedures. Studies were qualitatively assessed for validity using the Messick validity framework and models were assigned levels of recommendation using the McGaghie model of translational outcomes.
Results:
A total of 98 studies were included in this study assessing 51 models, with 28 studies concerning models for urethrocystoscopy, 46 studies for ureterorenoscopy, and 39 studies for percutaneous access and/or nephrolithotomy. Only four models demonstrated a level of recommendation of 4. The most validated models were the URO/PERC-Mentor (Simbionix, Lod, Israel) with multiple studies for each across various procedural skills.
Conclusion:
There is a wide spectrum of simulation-based models currently available for urolithiasis procedures, mostly with limited validity evidence from small studies. Further research is required with higher levels of evidence including randomized controlled trials. In addition, long-term transfer of skills to the operating room should be assessed to establish whether there is genuine skill development and retention using simulation models and whether this helps to reduce surgical complications.
Introduction
Urolithiasis is one of the most common presentations in urology, with trends showing numbers of uretero(reno)scopy (URS) performed worldwide increasing by 252% in the last two decades. 1 During this period, we have also witnessed the introduction of modern minimally invasive surgery (MIS) techniques, such as percutaneous nephrolithotomy (PCNL). These relatively new interventions have reduced transfusion rates and hospital costs. 2 MIS training, however, is more challenging and associated with higher costs, which consequently requires time and money to establish skills required for these procedures. 3
Simulation is thought to be effective during the initial phase of training. 4 Previously, residents underwent traditional methods to acquire surgical skills in the operating room (OR) on patients. Strict ethical imperatives have further reduced training opportunities and fast-tracked the growth of simulator use to form the gateway of the next level of surgical training. This approach allows exposure to crucial surgical skills without presenting any risk to patients. In terms of achieving desired outcomes, simulation-based practice in surgical education illustrates a dose–response relationship, whereby more practice yields better results. 5
Much of the current literature is still loosely centered around a subjective and outdated concept of validity. Although this taxonomy maintains some relevance to simulation-based training, behavioral scientists no longer accept this method of assessment. The newer concept considers validity as a unitary construct with an added focus on the interpretation of simulator data. 6
The principal objectives of this review are follows: To identify current simulation-based modalities pertaining to urolithiasis procedures, to evaluate the evidence behind its validity status according to updated definitions, and to make recommendations for use in surgical training based on evidence.
Materials and Methods
This study was conducted using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement guidelines 7 and registered on PROSPERO (CRD42019118734). 8
Eligibility criteria
Articles selected for review included various study types including observational, randomized controlled trials (RCTs), nonrandomized studies of interventions, pilot studies, and questionnaires. Review articles were included, subject to them presenting new information not already mentioned in original studies. Articles that mentioned use of a simulation-based model for urolithiasis surgical training and/or had its validity assessed were also considered eligible for selection. Conference abstracts were included if they matched the search criteria and presented novel information. Reference lists in retrieved studies were hand-searched for other relevant studies. The exclusion criteria included research articles that did not discuss a relevant procedure, were not in the English language, or published before 2000. Articles that did not explicitly evaluate a model/simulator for use in urolithiasis training were also excluded, as were articles that did not present sufficient information.
Information sources and search method
The Medline and EMBASE databases were searched for articles discussing simulated training methods for urolithiasis procedures and/or assessing its validity. A wide initial search was conducted to identify existing articles dated between 2000 and November 2018. The terms of this literature search were set out to identify the majority of relevant articles, and to include three principle concepts:
urolithiasis (the condition)
endourology/urethrocystoscopy/ureterorenoscopy/ureteroscopy (the intervention) and
training/models/simulation.
Search terms included “urology,” “endourology,” “ureteroscopy,” “endourology,” “urethrocystoscopy,” “cystoscopy,” “ureterorenoscopy,” “PCNL,” “percutaneous,” and “percutaneous nephrolithotomy” followed by combinations of the terms “model*,” “train*” or “simulat*.” Articles that mentioned the term “ureter*” in the abstract were also screened and considered for inclusion.
Study selection
Titles and abstracts of retrieved studies were examined to identify relevant studies to be included. Duplicates of articles were removed. The remaining studies were then further examined with a full text review. Where disputes on inclusion occurred, a consensus was determined among the authors.
Data items
Information obtained from each study included authors, year of publication, study design, number of participants, training time, interventions and outcomes as well as data reflecting simulator use such as time taken to compete the task, number of attempts, number of adverse outcomes, Objective Structured Assessment of Technical Skills (OSATS) scores in addition to expert and participant feedback. Details of the models such as the name, manufacturer, mechanism of function, and the cost of production were also retrieved. Data analysis of study data were also utilized to establish whether there were any statistically significant differences between control and intervention groups. Statistical evidence presented to evaluate interrater/test-retest reliability, such as Cohen's kappa or Cronbach's alpha, were also considered as a measure for reliability and internal consistency, respectively.
The selected models were classified into distinct groups: Augmented Reality (AR), Virtual Reality (VR), Bench, Organic, Animal and Cadaveric models.
Data analysis
Studies were analyzed according to the modern concept of validity set out by Messick's framework to identify its level of evidence (LoE). 6 These were given a rating subject to the study addressing parameters such as content, response processes, internal structure, relations to other variables, and consequences of using the simulated model. Studies were rated from N to 2, where N represents no discussion regarding validity evidence and zero indicates mention of validity with no evidence presented. A score of 1 or 2 suggests that the data support the studies validity.
Selected models were given levels of recommendation (LoR) as assessed per McGaghie's model of translational outcomes to establish whether it is an effective tool recommended for surgical training. 9 This was quantified using an LoR score from level 1 to 5, where LoR 1 indicates reference to a single parameter mentioned in the model. An LoR 5 indicates a cumulative reference of internal acceptability, contained effects, downstream effects, and target effects with the introduction of data signifying a wider systematic level of consequence. 9 Where an LoR could not be awarded, it was denoted with N/A (not applicable or not available). Studies that presented insufficient information were hyphenated in the relevant sections of the table (Table 1). Because of the heterogeneity of studies, it was not possible to perform a quantitative analysis.
Validation Studies on Urological Training Models (2000–2018) for Urethrocystoscopy
LoR = level of recommendation; VR = virtual reality.
Quality assessment
LoE for each study was ascertained according to the guidelines indicated by the validated modified Oxford Centre for Evidence-Based Medicine assessment tool. 10 Scores were assigned to each study that were then ranked according to the LoE presented (levels 1–5). Studies that attained LoE 5 were discarded and ineligible for inclusion owing to the strong risk of bias it presented. Study scores may be upgraded/downgraded based on study quality, precision, and consistency between other similar studies. Three examiners independently reviewed all identified studies to determine if they met the inclusion criteria and whether they matched the quality of evidence required. In the event of disagreement surrounding the inclusion of studies, named authors reached a consensus on inclusion.
Results
A total of 98 studies were included from 2525 initially retrieved studies (Fig. 1) and reference screening (Tables 1 –3).
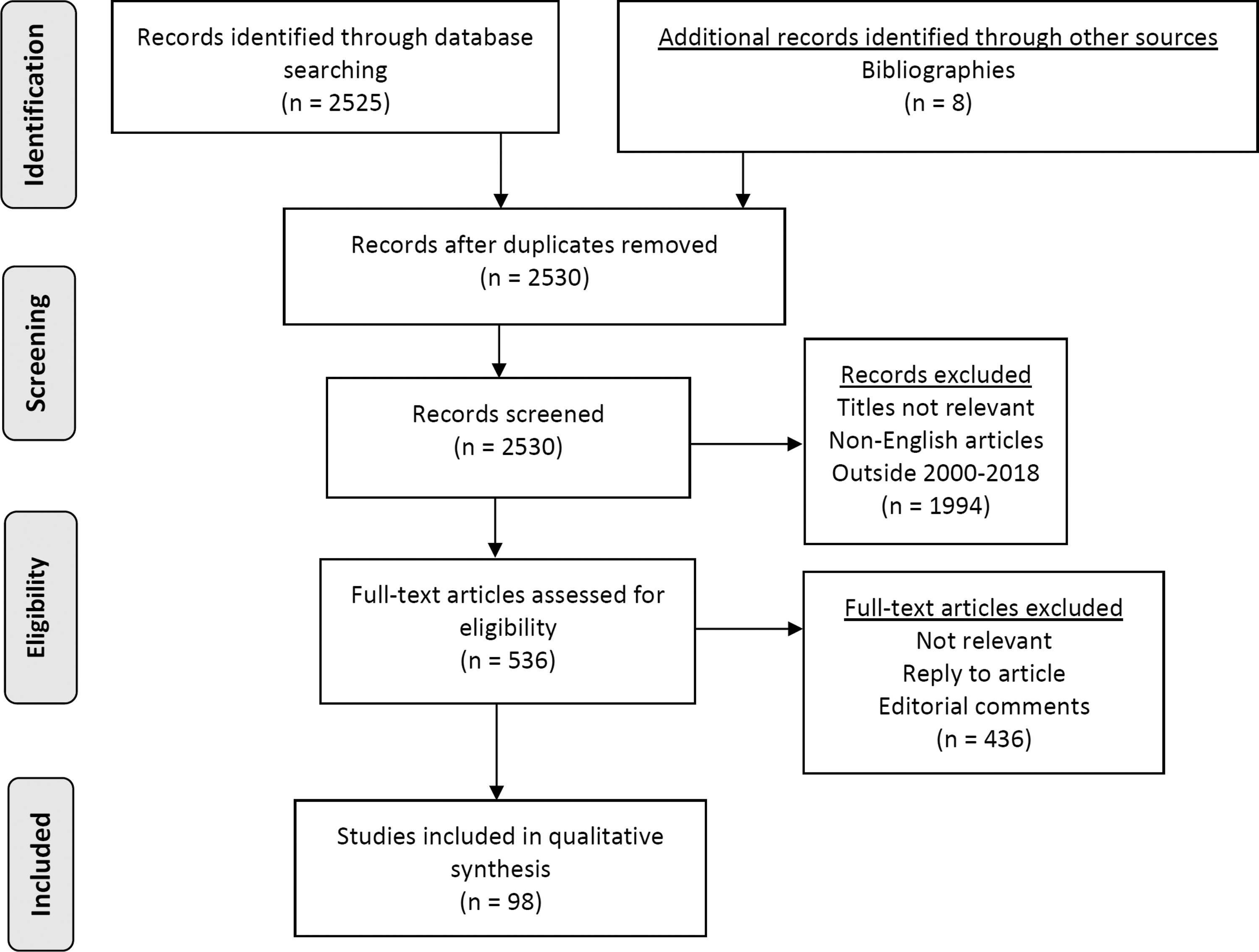
Study selection process, according to the PRISMA statement. PRISMA = Preferred Reporting Items for Systematic reviews and Meta-Analysis.
Validation Studies on Urological Training Models (2000–2018) for Ureterenoscopy
fURS = flexible ureterorenoscopy; rURS = semi-rigid ureteroscopy; URS = uretero(reno)scopy.
Validation Studies on Urological Training Models (2000–2018) for Percutaneous Nephrolithotomy
AR = augmented reality; CAT = C-Arm Trainer; PCNL = percutaneous nephrolithotomy.
Urethrocystoscopy
Twenty-eight studies 11 –38 were identified describing a total of 14 simulation-based training models, consisting of bench (n = 4), VR (n = 3), animal (n = 4), cadaver (n = 2), and organic (n = 1) subtypes. The mean number of participants was 32.9 (range 2–89). An LoR of 3 was achieved by six models, whereas four demonstrated LoR 2. Only one model had maximum validity for the consequences concept and six for content validity, the internal structure concept, and the response processes concept. The URO Mentor (Simbionix, Lod, Israel) was the most commonly reported model with a total of 13 studies retrieved. The primary function of this VR simulator was to provide training for ureterenoscopy, and also includes a number of basic tasks on systematic bladder inspection and bladder biopsies, which enables urethrocystoscopy (UCS) training.
Validated models
Twenty-seven studies were identified that validated 12 simulation models for UCS training, with 13 studies pertaining to the URO Mentor. This model demonstrated a good level of validity (Table 1) achieving an LoR of 3 owing to favorable responses and evidence of skills development.
Gettman and colleagues 11 used the URO Mentor to develop a curriculum and showed significant improvement in simulator time among 10 novices (p < 0.001). A complementary study 12 with 80 participants highlighted the simulator's ability to produce scores that correlate with user's experience level. The practical significance of the results were quantified using effect sizes (ES), where scores of 0.10, 0.30, and 0.50 were considered small, medium, and large, respectively. Data on novice performance demonstrated significant improvement with large ES scores in time (p < 0.001, ES = 0.66) and mean Global Rating Scale scores (p < 0.001, ES = 0.84). Furthermore, an RCT by Schout and colleagues 13 of 100 participants highlighted the transfer of skills from the VR simulator to the OR (p ≤ 0.003). Another RCT 14 utilized this VR simulator to teach UCS skills to 32 medical students. The VR simulator was used in combination with a low-cost, low-fidelity glass model. The intervention arm utilized both models together and outperformed the control arm, which used the URO Mentor alone.
Three studies were identified, each of which described an animal model for UCS. Grimsby and colleagues 15 used a suspended boar urinary tract utilized by two novices, which described its use as a high-fidelity tissue surrogate. This model can be used to enhance core urological skills including cystoscopy in novices. It was also able to differentiate between levels of experience for foreign body retrieval and bladder biopsy procedures. Similarly, Soria and colleagues 16 developed a training model for UCS using a live female porcine bladder. This study used 50 participants and demonstrated realistic domains that accurately represent human anatomy. It also determined that the simulator was a useful tool and realistically simulated the procedure while discriminating between independent theoretical relations of skill (p = 0.000). Hammond and colleagues 17 described a novel model that uses a porcine liver submerged in irrigant within a cored-out pumpkin. This model is yet to be validated; however, it received an LoR of 1 owing to its high fidelity-to-cost ratio.
Two studies 18,19 were identified describing the use of fresh frozen cadavers (FFC) for rigid and flexible UCS skills. Ahmed and colleagues 19 described evaluation of the British Association of Urological Surgeons (BAUS) Cadaveric Training Programme, with 81 residents and demonstrated that FFCs give an accurate representation of a number of surgical procedures including rigid/flexible cystoscopies and bladder biopsies. FFCs displayed feasibility, cost-effectiveness, and a high value for educational influence for cadaveric simulation and therefore achieved an LoR of 3. An RCT study by Bowling and colleagues 18 on 29 obstetric residents highlighted the models ability to correlate with theoretical relationships of skill and therefore achieved a score of 2 for relations with other variables.
Uretero(reno)scopy (URS)
Forty-seven studies 16,17,19,20,22 –28,39 –74 were identified that described a total of 20 models used for URS, consisting of bench (n = 14), VR (n = 1), animal (n = 3), and cadaver-based (n = 2) models. Seventeen studies described the URO Mentor (Simbionix), a computer-based VR simulator for training in both semi-rigid/flexible URS and rigid/flexible UCS procedures. The Uro-Scopic Trainer (Limbs & Things, Bristol, United Kingdom) was the second most described trainer and mentioned in seven studies. This high-fidelity bench model allows for both semi-rigid and flexible URS training with real instruments and consumables.
Three models demonstrated LoR of 4 and another three demonstrated LoR of 3, with the majority achieving an LoR of 2 (n = 14). Three models had maximum validity for the consequences concept, 17 for content validity, 10 had maximum score for the internal structure concept, 17 for relations to other variables, and 12 for the response processes concept.
Validated models
Forty-five studies were identified, validating 20 models for URS. Seventeen of these studies were aimed at the URO Mentor, which was by far the most evaluated option for URS training. Matsumoto and colleagues 39 used the URO Mentor as an assessment tool on a case of distal ureteral stones with 16 residents, whereas Wilhelm and colleagues 25 utilized it as a training tool in their RCT of 21 medical students and demonstrated statistically significant improvement in the trained group in parameters such as ability to perform the task (p = 0.035), total evaluator score (p < 0.001), and overall performance (p = 0.004). Mishra and colleagues 41 identified a mean realism score of 7.16 on a 10-point Likert scale (7.16 ± 1.69), among a group of 21 urologists performing flexible URS.
The study conducted by Ogan and colleagues 65 used cadavers and the URO Mentor for simple diagnostic URS among medical students and residents to determine the ability of these models to accurately predict OR performance. Within the medical student cohort, the performances of the VR model and cadaver showed a strong correlation for several measured parameters including total anatomy score (p = 0.008), time for task completion (p = 0.022), and overall score (p = 0.010). However, there was little correlation between the two models in residents, with statistically significant differences observed in manipulation (p = 0.043) and tasks (p = 0.046) only. The URO Mentor was accredited with an LoR of 4.
Chou and colleagues 57 used a porcine model to assess 16 medical students trained either by the Uro-Scopic Trainer or the URO Mentor. This study established that the ability of medical students to perform a basic URS procedure was independent of the training modality, thus confirming that incorporation of either simulator may improve clinical performance. Brunckhorst and colleagues 58 also developed a curriculum, incorporating a selection of tasks from models. The authors demonstrated the accuracy of the Uro-Scopic Trainer in mimicking the procedure and its ability to reflect the user's level of experience.
In addition to the Uro-Scopic Trainer, 13 other bench models were validated by a total of 20 studies. A high-fidelity bench model, the Adult Ureteroscopy trainer (Ideal Anatomic Modeling, Holt, MI), was evaluated by White and colleagues 40 on a cohort of 46 participants. This model demonstrated great accuracy in illustrating a realistic procedure with all participants rating the trainer as realistic and easy to use. It also displayed its ability to differentiate user levels of skill effectively with experienced surgeons scoring significantly higher on the global rating score (GRS) (p < 0.0001) and checklist (p = 0.004). They also required less time to completion on the task (p = 0.01). The Adult Ureteroscopy trainer achieved an LoR score of 2.
An anatomically accurate, transparent model of the urinary tract was assembled by Hu and colleagues 23 This was then compared with a similar model layered with black paint. Thirty-six medical students participated in this study and concluded that the cohort that trained with the transparent simulator had superior OSATS scores (p = 0.001).
Soria and colleagues 16 described utilizing the ETXY Uro Adam (ProDelphus, Olinda, Brazil) high-fidelity bench model, a porcine “renoureteral tissue” model, and a live porcine model for URS training among 40 trainees and 10 experts. The authors concluded that this model demonstrated satisfactory evidence for its ability to correlate with operating experience in all assessed parameters, and as a useful tool for residents-in-training (p < 0.001). Time for completing the task reduced with successive training, eventually plateauing at the sixth attempt (18 ± 3.4 to 11 ± 1.2 minutes, p < 0.05). This model received an LoR of 3.
Use of Thiel-embalmed cadavers (TECs) for URS was reported in three studies 27,28,74 effectively highlighting its usefulness as a tool for OR preparation. The use of FFCs for semi-rigid and flexible URS was described by Ahmed and colleagues 19 as part of the BAUS Training Programme and again demonstrated to be beneficial as a teaching model and in its detail at mimicking the operating environment. The use of TECs and FFCs both received an LoR of 3.
Percutaneous access and/or nephrolithotomy
Thirty-nine studies 17,32,75 –111 were identified pertaining to a total of 17 models used for percutaneous renal procedure, consisting of bench (n = 11), VR (n = 1), AR (n = 1), animal (n = 3), and organic (n = 1) modalities. One model demonstrated LoR of 4 and six models demonstrated LoR of 3 with the majority otherwise scoring an LoR of 2 (n = 10). Two models had maximum validity for the consequences concept, eight for content validity, two for the internal structure concept, seven for relations to other variables, and two for the response processes concept.
Nine studies described the PERC Mentor (Simbionix) VR simulator, 32,75 –81,110 which is a platform often combined with the URO Mentor and allows for percutaneous puncturing of a mannequin under fluoroscopy guidance, using a virtual C-arm through a range of clinical cases. The mannequin has simulated layers of the epidermis and palpable ribs, enabling haptic feedback.
Bruyere and colleagues 90 created a rapid prototyping model that utilized patient CT images allowing for patient-specific simulation before the procedure. The PCNL Trainer (Limbs and Things) consists of a slab comprising multiple calices where stones may be placed. It also responds realistically to the use of instruments. 82
Three main animal models were utilized for training. The porcine kidney was used while wrapped in silicon, 111 foam, 100 or placed inside a chicken carcass to simulate the posterior tissue layers. 17,105,106 Several other studies have reported use of live porcine models for training. 77,80,81
Validated models
Thirty-nine studies were identified validating 17 models for percutaneous renal procedures. Nine were attributed to the PERC Mentor. 32,75 –81,110 These studies established the model's usefulness as a surgical learning tool and also its ability to correlate with external, independent factors. This was highlighted by Knudsen and colleagues, 75 who concluded that training using the simulator significantly improved performance in complete novices (n = 31) and residents (n = 32). Shamim Khan and colleagues 32 reinforced this concept in their evaluation of a dedicated urology simulation program utilizing the PERC Mentor among other simulators where senior trainees performed significantly better than juniors in all simulation sessions (p < 0.001). The studies evaluating this model cumulatively displayed good quality control using standardized, validated assessment scales thus minimizing examiner bias. The PERC Mentor's ability to predict OR performance was established by Mishra and colleagues 80 where novices were trained using the PERC Mentor. Before training, 1/5 novices attained baseline success in contrast to 5/5 novices who demonstrated post-training success. Participants who were unavailable to perform testing on the porcine model were excluded from the final analysis to avoid test result bias.
Another study by Noureldin and colleagues 110 employed a cohort of 26 postgraduate trainees who used the PERC Mentor to assess competency in attaining percutaneous renal access. The correlation between previous experience with the PERC Mentor and other endourological procedures were assessed comparing GRS. Results revealed that 100% of the trainees with previous experience with the simulator were competent, compared with 38% in the group without sufficient experience (p < 0.001). All postgraduate trainees who had utilized the simulator for training also performed the task with significantly shorter operating (p < 0.001) and fluoroscopy times (p < 0.001) and achieving a significantly higher number of successful punctures to access renal calices (p = 0.001). This model attained an LoR score of 3.
Six bench models were identified, 84,87,89 which negate the need for fluoroscopy and subsequent radiation exposure. The Fluro-less C-arm Trainer (CAT; SimPORTAL, MN) was evaluated by 14 urologists 87 demonstrating validity evidence for its content, its ability to accurately reflect a realistic operating environment, and its worth as a surgical learning tool. Chrouser and colleagues 88 conducted a 2-day training program utilizing the CAT among 23 residents, following which significant improvements in performance were observed in upper pole renal access (p = 0.0015), but with no changes seen in lower pole access. Furthermore, participants perceived the CAT as a “very helpful” training tool for familiarizing with PCNL access. These results highlight the model's ability to correlate with levels of experience, thus achieving an LoR of 2.
Three animal models were validated 17,77,80,81,83,99 –106,111 and used for training experts and novices. A porcine kidney including its own skin, subcutaneous fat, fascia, and muscle layers was described by Zhang and colleagues 99 where the authors recruited 42 urologists to perform percutaneous procedures on the model. All participants rated the model “helpful” or “very helpful” and it received an LoR of 2. Mishra and colleagues 81 described the use of live anesthetized pigs for percutaneous renal access and the PERC Mentor with 24 experts. The study concluded that both models were equally useful (mean [SD], 4.6/5 [0.6] vs 4.65 [0.5]). Although the former was more realistic (p < 0.001), the PERC Mentor proved to be more useful in terms of repeating tasks (4.85 [0.4] for both, p < 0.001). The use of live porcine received an LoR of 2.
Discussion
For many years, the fundamentals of surgical skills were acquired using the Halstedian principle of “see one, do one, teach one”; however, this outdated method presents ethical and safety issues for patients. Without underestimating its importance, it is now being swept aside by more contemporary forms of training with the introduction of simulation-based models to further master the practical and theoretical knowledge required for urolithiasis procedures. Simulation-based training not only allows assessment of technical skill, but also allows evaluation of imperative surgical qualities such as decision making, time management, and communication skills that all have a significant bearing on surgical outcomes.
This study found that among the validated VR trainers available, the majority of studies were conducted on the URO/PERC Mentor, which is, to date, the only available and most thoroughly evaluated VR simulator with the highest LoE. They both display a high level of validity with substantial evidence supporting each domain. The URO/PERC Mentor VR simulators have multiple advantages including reusability, quick set-up time, data capture, and objective performance evaluation metrics. As a result, this model has established itself as the forefront VR simulator for urolithiasis procedures; however, more evidence is required for interpretation of the scores achieved from the simulator and its implications in the workplace. There are other limitations to this model such as its cost, maintenance, and lack of real instruments.
Bench models have become the mainstay of surgical training in urolithiasis owing to their portability, reusability, and use of real instruments. Advanced bench models that allow for complex procedures are better suited for senior residents who have more expertise in the field. Basic models may be more useful to novices as an introduction to the field, allowing for effective allocation of resources. A large proportion of bench models have demonstrated its ability at accurately resemble the surgical environment. It also displays qualities in correlating with theoretical relationships of skill, time, and experience and consequently makes it a useful teaching tool for novices.
The Uro-Scopic Trainer and CREST KUB model demonstrated the highest LoE among the bench models. Of the validated models, the Adult Ureteroscopy Trainer (Ideal Anatomic Modeling) and Endo-Urologie Modell (Karl Storz, Tuttlingen, Germany) do not seem to be commercially available any longer. PCNL models displayed the least amount of evidence and future studies ought to focus assessment of validity evidence. The majority of the available models are of high fidelity and therefore expensive, nevertheless significantly cheaper than the URO Mentor.
In contrast, studies evaluating animal models have been limited. The principal benefits of animal models are their similarity to human anatomy, and the ability to get tactile feedback. These qualities befit the use of these models for advanced procedural training. However, the use of animals presents potential ethical issues and consequently affects their availability for training. At present, the only well-validated model is ex vivo porcine kidney-ureter tissue, which has shown to be very useful and effective for URS. 16,20,22 Studies supporting its use also scored well with its internal structure and response processes both achieving a score of 2, highlighting the quality of evidence presented, and its reproducibility, respectively.
Although cadavers have long been utilized for surgical training, there is poor evidence supporting their use. Most conducted studies are of either low participant size or constitute evaluation surveys. Recently, it is now thought that TECs have a greater degree of realism in contrast to FFCs, but is yet to be comprehensively compared in studies. Nevertheless, participants and experts alike both highly recommend cadaveric training in the form of masterclasses.
In light of the current evidence, we recommend that simulation-based urolithiasis training (Fig. 2) for each procedure may be initiated with VR training using the URO/PERC Mentor, as it is the modality that least replicates procedures for the OR setting but may prove to be beneficial in gaining familiarity of concepts, instruments, and steps of the procedures. This can be followed with bench models with good LoR, using real surgical instruments and irrigation. Animal tissue models such as porcine kidney-ureter should be at the next phase of training owing to its resemblance with human anatomy. Moreover, nontechnical skills training using the validated full immersion simulation training should be incorporated alongside selected models, as recommended by Brunckhorst and colleagues 58 The final stage of procedural training should constitute masterclasses with live porcine and/or human cadavers, because of associated costs and ethics in gaining access to such facilities. 19

Figure illustrating simulation models and the recommended stepwise training approach. Color images are available online.
The majority of simulation studies have been conducted on a small number of participants with poor design and thus the field requires further research to critically compare simulators with reasonable LoRs against each other. Furthermore, longer follow-up periods must take place post-training to assess whether there is genuine skill development and retention. This will also reveal its transferability in the OR and will reflect whether they affect patient outcomes. Similarly, it is important that available models should each be analyzed to identify strengths and weaknesses to determine their best area of use for incorporation within formal curricula. Furthermore, future studies should focus on recruiting residents in-training, as they will ultimately be at the receiving end of such training programs.
There is also a growing literature base surrounding the use of objective assessment tools to evaluate manual dexterity using motion-tracking devices. 112 These have been extensively validated as an accurate motion-tracking device for evaluation of surgical dexterity and could be used alongside established assessment tools such as GRS and OSATS. In addition, substantiated by the work of Van Herzeele and colleagues, 113 cognitive training for urolithiasis procedures should be further explored for incorporation into training curricula. Its application to urolithiasis procedures must be evaluated and its integration into curricula alongside recommended models should be considered.
There was a clear lack of simulation data utilization for deciding progression in training and for use in selection criteria for surgical applicants. These are two areas with great potential for simulator data incorporation to prioritize higher ranking applicants, making it a great resource for program directors, managers, admission officers, and researchers alike.
This review accounted for a range of urolithiasis models, directing the scope of further research by giving each model an impartial retrospective score for their LoR, emphasizing their potential for clinical use in addition to evaluating studies using the updated definition of validity. To our knowledge, these are unique aspects of this study, which is a clear strength and separates itself from similar reviews performed in the past.
Limitations
The absence of training time data in many studies for participants was a clear limitation identified. Publication bias may have also skewed the validation studies of the simulators. The exclusion of non-English language articles, articles outside 2000 to 2018 and lack of randomization may also suggest evidence of selection bias to our analysis. Similarly, although systematic, the assignment of LoE and LoR was a subjective process and human error may have occurred. Another important limitation is that there are clearly a low number of RCTs assessing the validity evidence of simulators, most with few participants recruited. Furthermore, it is unclear from the current literature how skills obtained from a model-based training system are transferred into real-life surgical procedures; thus, the number of cases to reach competence is yet to be defined. 114
Conclusion
This study has highlighted the models that are available in this field and the evidence supporting their integration in training in urolithiasis. It is recommended for surgical trainers to utilize a combination of models mentioned in this study in a modular curriculum with preference given to models with the highest LoE and LoR. Further research is needed surrounding the transferability of skills through high-quality RCTs and the use of well-powered studies. Long-term follow-up studies are essential to establish whether these simulators genuinely retain the skills gained through simulator use and whether this helps to reduce surgical complications in the future.
Footnotes
Acknowledgments
The authors acknowledge support from The Urology Foundation, NIHR Biomedical Research Centre, MRC Centre for Transplantation, King's Health Partners, Guy's and St. Thomas' Charity, School of Surgery, Health Education England, Royal College of Surgeons of England, Olympus, The Pelican Group, Technology Strategy Board, and The Vattikuti Foundation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.