
Abstract
Introduction and Objective:
Single-use flexible ureteroscopes have the benefit of decreasing infection transmission, avoiding sterilization need, and no maintenance cost. Primary objective was to compare in vivo performance and surgical outcomes with two single-use ureteroscopes: LithoVue (Boston Scientific, USA) and Uscope PU3022a (Zhuhai Pusen, China) with secondary objective being to compare in vivo vision by independent endourologist blinded to ureteroscope manufacturer.
Materials and Methods:
Fifty patients undergoing retrograde intrarenal surgery with <2 cm renal stones were prospectively allocated: Group 1 (25 patients) for LithoVue and group 2 (25 patients) for Uscope. Pre-, intra-, and postoperative parameters were evaluated. Vision of both ureteroscopes with and without accessory was evaluated by an independent endourologist, blinded to the make of the ureteroscope. Stone clearance was assessed with kidney, ureter, and bladder radiograph (KUB) and ultrasonography KUB at 1 month. Student's t-test for quantitative and chi-square for categorical data was used.
Results:
Pre- and intraoperative parameters such as need for ureteral dilatation (p > 0.05), ureteral access-sheath size (p = 0.78), accessibility to pelvicaliceal system (p > 0.05), and maneuverability (p > 0.05) were comparable in both groups. Lower-pole access was possible in all cases of LithoVue and slightly difficult in three cases of Uscope (p > 0.5). Intraoperative vision was hazy in four cases of LithoVue and eight cases of Uscope (p = 0.32) during lasing along with three cases of Uscope with accessory (p = 0.24). Blinded endourologist reported more cases of hazy vision with or without accessory or lasing in Uscope arm (p > 0.05). One device had malfunction in LithoVue arm. Complete stone clearance was achieved in all cases at 1 month.
Conclusions:
We conclude that performance of these two single-use ureteroscopes, LithoVue and Uscope, is comparable in clinical settings with similar clinical outcomes and complications.
Introduction
The first documented case of ureteroscopy (URS) was conducted in 1912 by Hugh Hampton Young and RW MacKay using a 9.5F pediatric cystoscope. 1 The first ureteroscope was created in 1964 after technological advancements. 2 The initial flexible ureteroscopes had limitation of smaller working channel and limited amount of deflection. With further advancements, there was transition from fiber-optic to digital flexible ureteroscopes. There were still some concerns about their durability and significant costs associated with sterilization and repair. 3,4 Many factors, including sterilization technique, procedure type, surgeon experience, and prior ureteroscope refurbishment, contribute to the reduced durability and subsequent repair cost of reusable ureteroscopes. 4 –7 There are various studies comparing the cost analysis of single-use and reusable flexible ureteroscopes with varied outcomes. 6,8,9 The other most important aspect of reusing flexible ureteroscope is transmission of infection. There are studies describing association between various multidrug-resistant Enterobacter cloacae and Pseudomonas aeruginosa and the poor sterilization of reusable ureteroscopes. 10,11 A study conducted by Ofstead and colleagues showed that even when reusable ureteroscopes were cleaned manually and sterilized by hydrogen peroxide gas, contamination (by bacteria, adenosine triphosphate, hemoglobin, and/or protein) could still be found in the ureteroscopes tested. 12
Many single-use disposable flexible ureteroscopes have been introduced into market by different manufacturers. The first single-use disposable flexible ureteroscope was the LithoVue (Boston Scientific, USA), which is the most widely used and studied, and has a well-established track record in clinical studies and has equivalent consistent performance with reusable flexible ureteroscope. Inclusion of a metal oxide semiconductor sensor located at the tip of the endoscope that provides a 0° direct view with 85° field of vision is the additional advantage of LithoVue™. 13,14 There are many other single-use digital flexible ureteroscopes already on the market, including Uscope PU3022a (Zhuhai Pusen, China), Polyscope (Polydiagnost, Germany), Semi-Flex Scope (Maxiflex, CA, USA), FlexoVue (Cook Medical, USA), and Yc-FR-A (YouCare Tech, China). 15 Many studies have done in vitro testing and have shown that single-use ureteroscopes have equivalent optics, deflection ability, and working channel flow rates to reusable ureteroscopes. 16 –20 Limited studies have compared the single-use flexible ureteroscopes in vivo. 21 Uscope PU3022a (Pusen), a recently available single-use flexible digital ureteroscope, is also evaluated in some studies. 20,22
The primary objective was to compare these two single-use ureteroscopes in a clinical setting: LithoVue and Uscope PU3022a with the secondary objective being to compare in vivo vision by an independent endourologist blinded to ureteroscope manufacturer.
Materials and Methods
A prospective single-center double arm comparative study was carried out by Muljibhai Patel Urological Hospital, a tertiary care center, from January 2019 to April 2019. Fifty patients, aged >18 years and normal upper tract anatomy with renal stones <2 cm, planned for retrograde intrarenal surgery (RIRS) were prospectively allocated to two groups: Group 1 had 25 patients in which single-use LithoVue ureteroscope was used and group 2 had patients in which single-use Uscope was used. All procedures were performed by the same urologic team having experience of >300 RIRS procedures. Patients with known ureteral stricture, pregnancy, presence of renal insufficiency, and active kidney infection were excluded.
The preoperative patient demographic details, stone size, density, location, number, and laterality along with preoperative stenting were collected. Various intraoperative parameters were recorded such as preoperative, intraoperative vision (with/without accessory and laser and during lasing), and reinsertion vision on a 3-point Likert scale as sharp, hazy, or blurred. The other parameters included ureteral access sheath dilatation, accessibility to pelvicaliceal system, maneuverability of ureteroscope in pelvicaliceal system, and lower pole access (with/without accessory and laser) on various Likert scale by operating surgeon. Clinically important parameters such as operative and lasing time and hemoglobin drop were also evaluated. Intraoperative malfunction and postoperative complications were noted. The videotape of both the ureteroscopes were also evaluated by endourologist blinded to the make of the ureteroscope. He rated vision of both ureteroscopes (with/without accessory and during lasing) as sharp or hazy. Stone clearance was evaluated at 1 month with X-ray and ultrasonography (USG) kidney, ureter, and bladder radiograph (KUB).
Informed consent was taken, and the study had institutional ethical clearance. The statistical analysis was done using IBM SPSS Statistics for Windows, version 23.0 (IBM Corporation, Armonk, NY, USA). After checking for the normality of the data, the continuous data were compared using Student's t-test and the categorical data were compared using chi-square test. The significance level was kept at p < 0.05.
Results
The preoperative demographic parameters were comparable in both the groups (Table 1). Intraoperative parameters, including the need for ureteral dilatation (p > 0.05), ureteral access sheath size (11/13 or 12/14; p = 0.78), accessibility to pelvicaliceal system (very easy/slight difficult; p > 0.05), and maneuverability within pelvicaliceal system(very easy/slight difficult; p > 0.05) were comparable in both the groups. The lower pole access was possible in all cases of LithoVue but was slightly difficult in three cases of Uscope (two with laser [p = 0.49] and one with basket [p > 0.05]) but was statistically comparable.
Patient Demographic Parameters and Stone Characteristics and Postoperative Parameters
SD = standard deviation.
Intraoperative vision was hazy in four cases of LithoVue during lasing, whereas sharp in all remaining cases. It was blurred in one case of Uscope arm and hazy in three cases of Uscope with accessory (p > 0.05) and eight cases during lasing (p = 0.32), whereas all remaining cases had sharp vision but were statistically comparable (Table 2).
Intraoperative Parameters
One case had intraoperative device malfunction in LithoVue arm. All patients had complete stone clearance at 1 month with X-ray and USG KUB. The blinded endourologist reported more cases with hazy vision in Uscope arm but was statistically insignificant (p = 0.17 for vision with accessory, p = 0.34 during lasing) (Table 3).
Third-Person Observation Blinded to Ureteroscope Manufacturer
Discussion
There are multiple single-use flexible ureteroscopes available in market today. They are good alternatives to reusable ureteroscopes to prevent loss of deflection, repair cost, infection transmission, and operative turnover time. Various studies have evaluated these single-use ureteroscopes with reusable ureteroscopes. Many of these studies are in vitro. 17 –20 There is scarcity of literature about the comparison of single-use ureteroscopes. As there are many single-use ureteroscopes being marketed, there is need for comparison of these ureteroscopes.
The LithoVue (Boston Scientific, USA) was the first single-use ureteroscope to be universally accepted into clinical practice and remains the most widely used and studied single-use ureteroscope to date. The Uscope PU3022a (Pusen), recently available single-use digital ureteroscope has been evaluated in some in vivo and in vitro studies. The data on comparison of both these ureteroscopes in clinical settings are sparse.
Good optics with adequate irrigation is required for efficient, safe, and complete stone clearance. We evaluated vision of both ureteroscopes with and without accessory along with vision during lasing of stone. The vision of LithoVue was sharper than Uscope especially during lasing of stone, but the difference was not statistically significant (p = 0.32) (Fig. 1). The surgical video evaluated by a third-person blinded endourologist found sharper images in LithoVue than in Uscope with accessory and during lasing, but the difference was not statistically significant (p = 0.17, p = 0.34). On the contrary, Marchini and coworkers showed that LithoVue had higher resolution than Uscope (p < 0.001), but this was in in vitro condition. 20 Winship and coworkers also showed in their in vitro study the similar results only at 10 mm distance, whereas there was no significant difference at 20 and 50 mm distances. 19
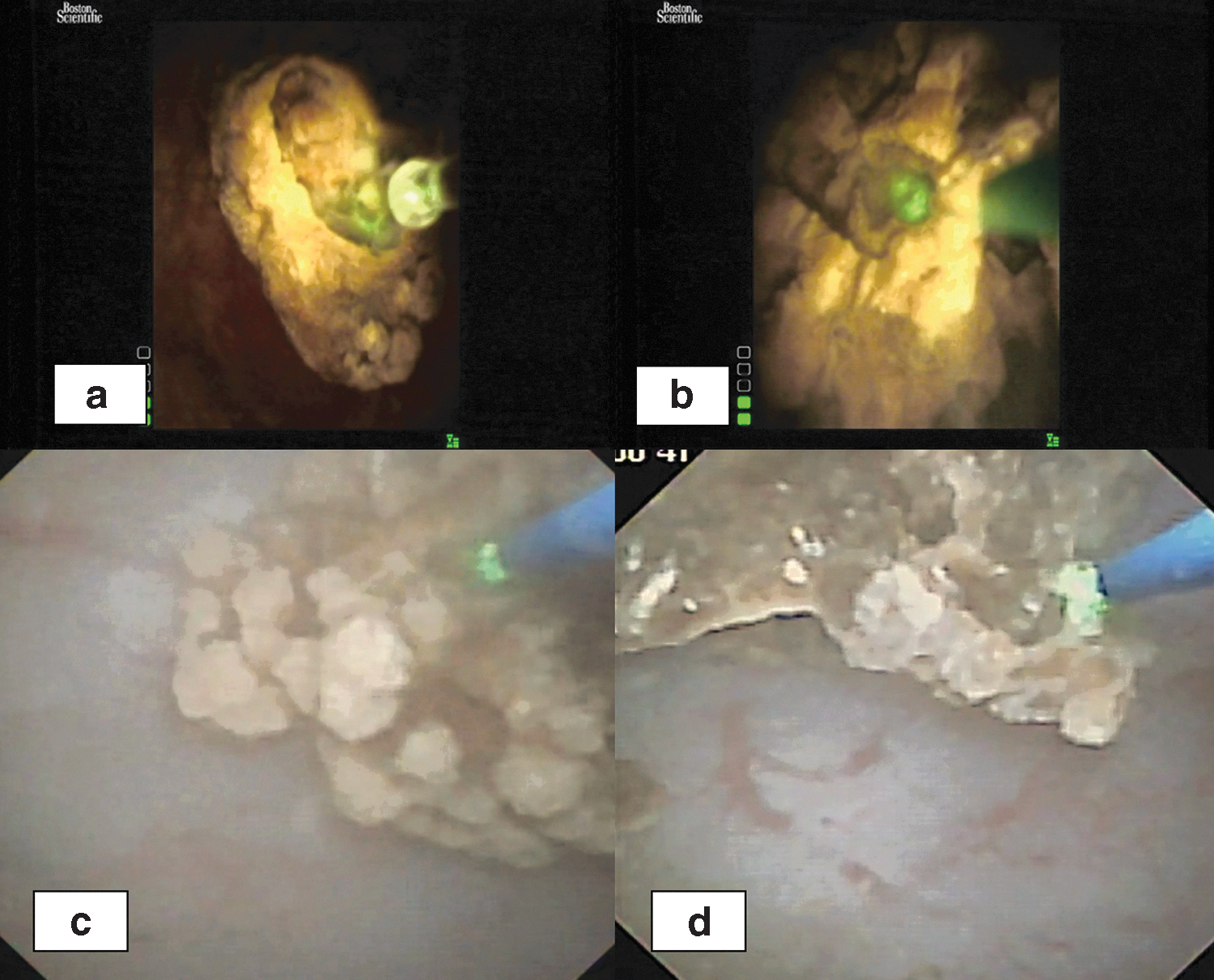
Figure demonstrates vision during lasing of LithoVue
The maneuverability in the pelvicaliceal system was similar for both the ureteroscopes. But, Marchini and colleagues in their in vitro study found that LithoVue handling was more comfortable than Uscope probably because majority of the surgeons were trained in the manner LithoVue is maneuvered. 20 Kam and coworkers comparing Uscope and LithoVue in the in vivo setting concluded that although there is difference in image quality and maneuverability, it did not translate into clinical significance as both the ureteroscopes had comparable surgical outcomes. 21 This is also reflected in this study, as patients operated by both the ureteroscopes had complete clearance at 1 month as evidenced by X-ray and USG KUB. The operating and lasing time in LithoVue and Uscope arm was (48.8 ± 13.28 and 49.6 ± 22.17 minutes, p = 0.88) and (5.34 ± 4.56 and 5.05 ± 3.39 minutes, p = 0.80), respectively. Thus, both the parameters were comparable in both the groups.
Deflection of ureteroscope was evaluated as lower pole accessibility with and without accessory instruments. It was possible in all cases by LithoVue ureteroscope and slightly difficult only in three cases by Uscope especially when laser fiber and basket was used. However, the difference was not statistically significant (p > 0.05). Various in vitro studies have demonstrated greater deflection loss in Uscope than LithoVue. 19,20 Winship and colleagues in their in vitro study concluded that the difference between both the ureteroscopes is subtle and clinically insignificant. The deflection loss with laser fiber is more for Uscope, but Uscope has greater deflection with empty channel. Thus, it leads to similar absolute deflection with laser fiber for both ureteroscopes. Although these are single-use ureteroscopes, they also demonstrated durability as there was less deflection loss even after 200 cycles of deflection. 19
There was similar hemoglobin drop in both the groups (p = 0.35). There were two patients with postoperative fever in each arm requiring antibiotics (Clavien–Dindo Grade 2). The safety of both the ureteroscopes was proved by no major complications in both the arms. One ureteroscope failure (4%) in LithoVue arm was noted, which is in concordance with 3.2%–5% mentioned in literature. 23,24 The performance of single-use ureteroscopes are slowly approaching reusable ureteroscopes and would offer as a good alternative. 17,21 As a pilot project, the blinded endourologist predicted the stone composition visually in both the ureteroscopes arms and he could predict it in 60% cases in both the arms. However, this needs further evaluation.
There are some limitations in the study. We have not compared these two single-use ureteroscopes with reusable ureteroscopes.
Conclusion
We conclude that performance of these two single-use ureteroscopes, LithoVue and Uscope, is comparable in clinical settings with similar clinical outcomes and complications.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding information was received.