
Abstract
Background and Purpose:
Ureteral stricture is a rare, but serious complication following ureteroscopy (URS) for stones. The aim of this study was to investigate how many patients ended up with a ureteral stricture after URS at our hospital and how these were treated. We also wanted to identify potential risk factors for postendoscopic stricture formation.
Materials and Methods:
A retrospective evaluation of 1001 URSs for stone treatment at the day-case surgery unit between 2013 and 2018 was performed. Data on pretreatment status, the surgical procedure, and follow-up were recorded. Exact χ2 and independent samples t-tests were used comparing data among those who developed strictures and those who did not. Multiple logistic regression was performed analyzing risk factors for stricture formation.
Results:
In total, 1001 URSs were performed in 725 patients, 289 women and 436 men. Of these, 995 cases were eligible for analysis. At follow-up with CT after 3 months, 28 (3.0%) strictures were identified. Of these, 20 received endourologic treatment with balloon dilatation of which 15 (75%) were effective. Definitive treatment in the 13 patients with failed or unattempted endourologic treatment included nephrectomy, reconstructive surgery, permanent nephrostomy, or observation with no further treatment. In multiple regression analysis, use of ureteral access sheath (UAS; odds ratio [OR] 4.6, p = 0.011), ureteral perforation (OR 11.8, p < 0.0001), and surgical time >60 minutes (OR 5.7, p < 0.005) were found to be risk factors for stricture formation.
Conclusion:
Ureteral stricture is a rare complication of URS. Balloon dilatation should be the first line of treatment. Use of UAS, perforation, and excessive operating time were found to be risk factors for postendoscopic ureteral stricture formation. Special attention to these risk factors should be given to reduce the incidence of ureteral strictures.
Introduction
A
The introduction of small diameter endoscopes, lasers, and auxiliary equipment is thought to have contributed to a reduction in the occurrence of postendoscopic strictures in recent years, with current rates reported to be 0.3% to 4%. 2,5 –7 However, the role of ureteral access sheaths (UASs) in the development of ureteral strictures is still debated. 8,9
The present study was planned with the aim of clarifying questions and identifying factors related to development of ureteral strictures following URS for stone disease. The main objective of this study was to determine how many patients ended up with a ureteral stricture after URS for urolithiasis at our hospital. Furthermore, we wanted to identify possible risk factors for postendoscopic stricture formation.
Secondary aims were to point out possible specific causes for stricture development in each case and see how these strictures were treated.
Materials and Methods
Setting, study population, and data collection
In October 2013, a new day-case surgery unit opened at Haukeland University Hospital (HUH) in Bergen, Norway. The URS procedures were reorganized from regular in-patient cases to being performed as day-cases in the new unit.
As part of an internal quality evaluation of the endoscopic activity in our department, a retrospective review of all the retrograde ureteroscopic stone treatments performed in the day-case surgery unit since the opening in October 2013 until June 2018 has been done. The indications for URS were the same in the 5-year time frame, and there was no major change in the performance of the procedure or in the equipment used.
In total, 1001 URSs for stones were performed in 725 patients, 289 women and 436 men. The mean age at the time of endoscopy was 55 years (range 4–95 years). The patients' general condition was assessed using the American Society of Anesthesiologists Score (ASA-Score), with 2 being the median ASA-Score.
A noncontrast CT was performed before the URS. Stone size was defined as the largest diameter of the calculus. If multiple stones were present, the largest diameter of the biggest stone was registered. Preoperative obstruction was defined as presence of dilatation proximal to the stone seen on preoperative CT, persistent pain, or finding of an impacted stone at the time of the URS. Table 1 presents the pretreatment basic characteristics.
Preoperative Characteristics
Some patients had stones in multiple locations.
CI = confidence interval; URS = ureteroscopy.
The URS procedures were performed using a semirigid endoscope (8F/9.8F tapering shaft; Richard Wolf Medical Instruments Corporation, Vernon Hills, IL), a flexible endoscope (URF-V-V3 or P6/P7; Olympus Corporation, Tokyo, Japan), or both. The decision to use a UAS or a safety guidewire (SGW) was entrusted to the surgeon in each case based on their personal preferences. In these cases, either a 10/12F or 12/14F UAS (UroPass®; Olympus Corporation) was inserted depending on the flexible endoscope used, while a super stiff hydrophilic guidewire with floppy tip (SureGlide® 0.035″; Olympus Corporation) was the standard guidewire. It should be noted, however, that a sheath- and wireless procedure is routine at HUH. A holmium laser was utilized for fragmentation of the stone when deemed necessary, and fragments were retrieved with forceps, baskets, or left in situ for spontaneous passage depending on the preferences and judgment of the urologist in each case.
To achieve the best possible estimate of postendoscopic strictures, cases in which dilatation of a ureteral stricture was required to reach the level of the calculus before stone treatment were excluded from further analysis. Characteristics of the URS procedures are presented in Table 2.
Comparison of Characteristics Related to the Ureteroscopic Procedure
Disturbing bleeding was registered as a complication when vision was impaired to an extent that hindered further endoscopy. Perforation was assessed endoscopically or as contrast leakage on retrograde pyelogram. Mucosal abrasion was defined as grade 2 or higher according to the classification of ureteral wall injuries presented by Traxer and Thomas. 15
Follow-up with noncontrast CT was performed after 3 months. A postendoscopic ureteral stricture was defined as dilatation of the upper urinary tract proximal to a ureteral narrowing verified on CT or verified directly at a second URS. Ureteroscopically, a stricture was noted if the narrowing was not passable for the endoscope in a location where a stenosis or tapering of the ureteral lumen was not registered during the first endoscopy. If dilatation was noted at follow-up, the patient was scheduled for a second URS to verify the presence of a ureteral stricture and continue with endoscopic treatment if considered appropriate.
Initial follow-up imaging was performed 3 to 6 months after the endoscopic treatment. Effective treatment was defined as regression of the dilatation seen on CT or ultrasound together with persistent relief of symptoms. Further follow-up was assessed in each case. In cases with persistent dilatation, a subsequent URS with a second attempt of endourologic treatment was performed. If still unsuccessful, an isotope renography was performed whenever there was doubt about renal function before reconstructive surgery, nephrectomy, or permanent drainage.
Statistics
Independent samples t-tests were performed comparing continuous variables, such as stone size and operating time. Categorical variables, such as sex and ASA-Scores, were compared using exact chi-squared tests. Multiple logistic regression analysis was performed to determine risk factors for ureteral stricture.
IBM SPSS Statistics 25 (IBM, Armonk, NY) was used for statistical analysis. The p-value was considered significant when <0.05.
Ethics
The study was approved by The National Committees for Research Ethics in Norway (ID No. 2018/2545 REK) and The Data Protection Authorities at HUH (ID No. 1041).
Results
During the study period, 1001 URSs were performed for the treatment of calculi. Six cases were excluded from further analysis because a ureteral stricture was identified and treated during the URS procedure before reaching the level of the stone. Of the remaining, 535 (53.8%) were done for stones located in the renal pelvis, 348 (35.0%) for ureteral stones, and 112 (11.3%) for both renal and ureteral stones combined. The preoperative stone status is provided in Table 1.
Follow-up after 3 months with a CT scan was registered in 947 cases (95.2%), and 28 (3.0%) strictures were identified. Figure 1 shows the stricture rate partitioned per year from 2013 to 2018. The stricture rates were stable throughout the study period with a mean rate of 1.8% per year, except 2017 when there was a peak in the number of strictures.
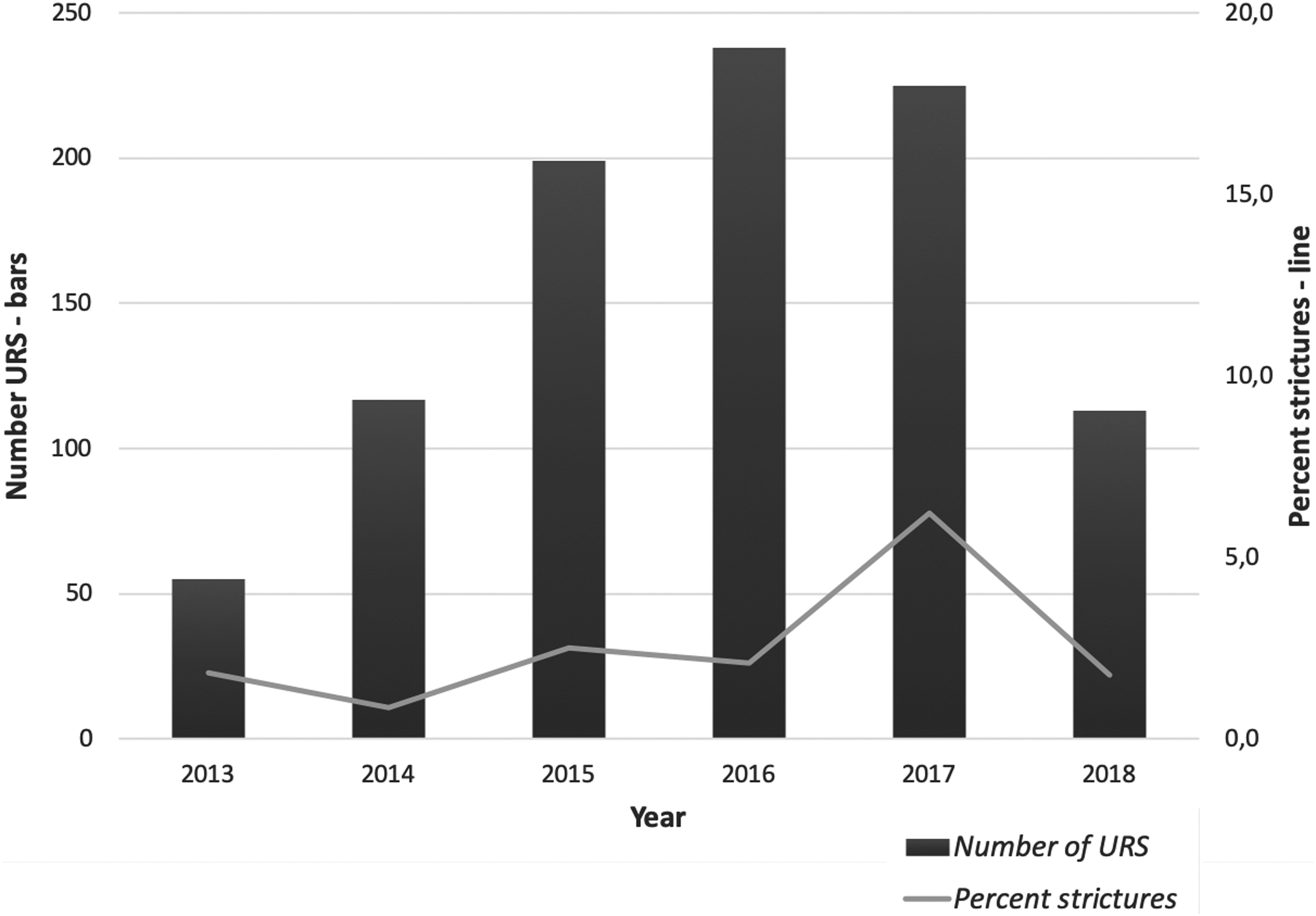
Ureteral stricture rates per year throughout the study period. In 2013, only procedures performed between October and December were included. In 2018, only procedures performed before July were included.
Preoperative, operative, and postoperative characteristics were compared for patients who developed a postendoscopic ureteral stricture and those who did not. There was no significant difference in the number of patients having obstruction before the URS in the stricture group compared to the nonstricture group, 13 (46.4%) and 305 (33.2%) cases, respectively, p = 0.157. Preoperative treatment with a Double-J stent was significantly more frequent in the stricture group with 11 cases (39.3%) compared to the nonstricture group with 122 cases (13.3%), p = 0.001. This may be related to the trend of more patients in the stricture group having previous URS attempts for the same stone (10 cases, 35.7%) compared to the nonstricture group (211 cases, 23.0%), p = 0.170.
Table 2 compares characteristics from the surgical procedures between patients who did not develop ureteral strictures and those who did. Two high volume endourologists performed more than half the number of procedures in addition to assisting residents in most of their URSs. The remaining procedures were performed by another six urologists.
UAS was used almost exclusively when treating renal stones. Only two cases of ureteral stones required UAS. The opposite was found regarding SGW, which was used in 3 cases of renal stones and 16 cases with ureteral stone.
In 21 cases (75.0%) the strictures occurred on the left side. Distal ureter was the predominant location for stricture formation followed by proximal and middle ureter in 12 cases (42.9%), 11 cases (39.3%), and 5 cases (17.8%), respectively. Twenty-two strictures (78.6%) were <2 cm long.
Table 3 presents possible risk factors for development of ureteral strictures determined by multiple logistic regression analysis. Use of UAS, intraoperative ureteral perforation, and operating time above 60 minutes all increased the risk for postendoscopic stricture significantly.
Multiple Logistic Regression Analysis of Potential Risk Factors for Ureteral Stricture Development
OR = odds ratio.
In most cases, more than one cause associated with stricture formation could be identified. In 20 cases (71.4%), events related to the URS procedure were registered as a possible cause of stricture development and impacted stones in 18 cases (64.3%). Previous radiation therapy as a contributing factor to stricture formation was registered in three cases (10.7%).
Of the 28 patients who ended up with a ureteral stricture, endourologic treatment was attempted in 21. Of these, 20 were treated with balloon dilatation. Fifteen patients (75.0%) were treated successfully with this procedure. Ten patients required a single treatment, and five patients needed two consecutive URS procedures with balloon dilatation before persistent success. One patient had laser incision of the ureteral stricture as the only endourologic treatment, which was unsuccessful. Endourologic treatment was not effective in any of the patients with previous radiation therapy.
Mean follow-up time was 14 months (range 1–42 months) in patients receiving endourologic stricture treatment with a mean number of 3 follow-up consultations (range 1–6). Mean follow-up time for the 15 patients with effective treatment with balloon dilatation was 17 months (range 2–42 months), with 3 consultations (range 1–6). In the six patients with unsuccessful endourologic treatment, the mean time from failed balloon dilatation or laser incision until final surgery was 8 months (range 1–15).
Location of the stricture in the ureter was not related to effective management with balloon dilatation. In contrast, strictures <2 cm had significantly higher success rate after endourologic treatment compared to strictures >2 cm, 14 cases (87.5%) and 1 case (20.0%), respectively, p = 0.011.
Definitive treatment in the 13 patients with failed or unattempted endourologic treatment includes nephrectomy in 4, reconstructive surgery in another 5, permanent drainage with a nephrostomy tube in 1, and observation with no further treatment in the last 3 patients who all had severe comorbidities or were asymptomatic secondary to a nonfunctioning kidney.
Discussion
By reviewing all the retrograde URS procedures performed for stones in the day-case surgery unit at HUH since the opening in October 2013, we have determined the incidence of postendoscopic ureteral strictures, identified risk factors for stricture formation, and mapped out how the strictures were treated.
At follow-up after 3 months, 28 strictures (3.0%) were identified. This is in accordance with other studies. 5,6,8,10 The stricture rates were stable throughout the study period except a peak in the number of incidences in 2017. We could not point out any specific reason for this increase as the indications for URS, the performance of the endoscopy, and the equipment used were unchanged during the study period.
The mechanisms of stricture formation following ureteroscopic stone treatment may be multifactorial and are not fully understood. Intraoperative ureteral injury and a long-term inflammation caused by impacted stones may be contributing factors. 11 The inflammatory process following injury produces a fibrinous exudate that precipitates on traumatized areas, promoting adherence and ultimately stricture formation. In addition, periureteral fibrosis may also develop when urine is extravasated from the ureter, especially in the presence of infection. 12 This means that any factor or event leading to ureteral wall injury is a potential risk factor for the development of ureteral stricture.
Impacted stones are considered to be one of the main predictors of stricture formation. 13,14 Detailed information regarding stone impaction was not available in the database. These data were retrieved from the patient charts for all patients who developed strictures. Preoperative obstruction may be an indication of the stone being impacted. However, dilatation may also be seen in stones that are unimpacted. This may explain why there was no significant difference in the number of strictures at follow-up in patients with preoperative obstruction compared to those with no preoperative obstruction.
Surprisingly, pretreatment with a Double-J stent was more frequent in patients who developed strictures. Prestenting has been demonstrated to reduce the risk of ureteral lesions during URS. 15 –17 Nevertheless, the protective properties of the stent might not fully have abolished the deleterious effects of an impacted stone in the present study and may explain why more strictures occurred in the prestented patients. In addition, there was a trend toward more patients in the stricture group having had a previous procedure for the same stone compared to the nonstricture group. This may also explain the higher incidence of prestenting. Another trend that may have contributed to the higher prestenting rate in the stricture group was larger stone size and more stones located in the ureter in these patients.
Three quarters of the strictures were located in the left ureter. May and colleagues have suggested that the left ureter might have an anatomical or functional predisposition to obstruction as more strictures seem to occur on this side. 2 This finding could not be confirmed in the present study. Nor could we identify a predilection site for strictures with regard to the level of the ureter. Castro and coworkers were also unable to demonstrate such an association. 18 In most cases, the level of the strictures coincided with the location of the stones.
Even though most strictures developed after treating stones in the ureter, we found no significant association between stricture formation and stone location. It is noteworthy that more than 35% of the strictures in our material were seen after URS for stones in the renal pelvis. This suggests that surgical technique is a major contributor to stricture formation.
A SGW was used in 19 (2.0%) cases only, with no difference between patients who developed strictures and those who did not. The use of a SGW has not been considered mandatory at HUH since URS was introduced in the early 1980s. In a previous study comparing URS for ureteral stones with and without a SGW, we could not demonstrate any difference in the number of intraoperative complications. 7 However, the postendoscopic stricture rate was significantly higher when a SGW was used compared to when it was omitted. 7
The use of UAS during URS is debated. Advocates for its use claim superior stone-free rates (SFRs), shorter operating time, and lower intrarenal pressure. 19,20 However, other studies have shown that insertion of UAS may lead to ureteral lesions. 15 In addition, large cohort studies have shown no difference in the SFRs whether a UAS has been used or not. 21 Due to these controversies, the EAU Guidelines on Urolithiasis state that the decision to use a UAS is up to the surgeon based on his or her preference. 10 UAS was rarely used in the present study, and conclusions should therefore be drawn with caution. Nevertheless, significantly more strictures were found when a UAS was used compared to when it was omitted. The use of UAS was also found to be a significant risk factor for development of stricture in multiple logistic regression analysis with an odds ratio of 4.6, p = 0.011. In a randomized trial, Lallas and coworkers demonstrated a transient decrease in ureteral blood flow when a UAS was inserted. 22 Even though blood flow returned to normal after a short period of time, the transiently impaired blood supply to the ureter may explain the higher rate of strictures when a UAS was used.
Intraoperative perforation and excessive operating time were found to be significant risk factors for stricture formation. These findings are in accordance with other reports. 1,2 The inflammatory response following a perforation may explain stricture formation. Excessive operating time might reflect a more complicated stone situation. In addition, an extended operating time undeniably causes reduced blood flow to the ureter either when dilatated by the endoscope or, even worse, by insertion of the bigger UAS.
Surgical experience was not found to increase the risk of stricture formation. This finding is in contrast to the increased risk of complications in URS performed by inexperienced surgeons reported by others. 3,4 An explanation may be that more complicated cases were operated by experienced surgeons in our series.
In total, 20 of the 28 patients who developed strictures were treated with balloon dilatation, 15 (75%) successfully. The success rate was higher when the strictures were <2 cm compared to longer strictures. Both findings are in accordance with other studies. 2,5
The retrospective design of this study is a limitation. This may have contributed to rough registration of data and underestimation of complications that could have affected the outcome. Incomplete renographic data make it difficult to assess the renal function after endoscopic treatment. However, regression of dilatation and remission of symptoms may still indicate effective treatment. Furthermore, in cases of persistent dilatation or pain, patients were investigated with a subsequent URS or an isotope renography. The added diagnostic value of controlling all stricture patients with an isotope renography may therefore be questioned in the present study.
Detailed data on stone impaction were only available for patients who developed strictures. This limitation has prevented us from including stone impaction as an independent risk factor in the multiple logistic regression analysis. Another limitation is the relatively low number of strictures. This may have caused important risk factors to falsely turn out as nonsignificant in the analyses. In addition, the low number of adverse events makes adjusted analyses of the background characteristics difficult. Despite the relatively low number of strictures, the present study is still one of the largest of its kind.
Conclusion
Ureteral stricture is a rare, but serious complication following URS. Our study suggests that endourologic balloon dilatation should be the first line treatment, with an expected success rate of about 75%. Risk factors for postendoscopic ureteral stricture formation were found to be use of UAS, perforation, and excessive operating time. Special attention to these risk factors should be given to reduce the incidence of ureteral strictures.
Footnotes
Acknowledgment
A special thank you is extended to Mr. Ravi Rawal, consultant urologist, for his assistance in reviewing the article.
Author Disclosure Statement
Ø.U. is a consultant for Olympus Corporation, who was not involved in the design, collection, analyses, interpretation, or reporting of the data. The two other authors have nothing to disclose.
Funding Information
No funding was received.