
Abstract
Purpose:
Our objective was to establish the incidence of positive surgical margins, recurrence patterns, and recurrence-free (RFS) and overall survival (OS) in a large cohort of patients undergoing robotic (robot-assisted radical cystectomy [RARC]) and open radical cystectomy (ORC).
Materials and Methods:
We performed a large retrospective cohort study at a high-volume academic tertiary referral center. Patients were those who underwent RC for bladder cancer from 2005 to 2017. Patients were allocated to ORC or RARC by patient and surgeon choice. Propensity matching and a multivariable analysis were performed to determine factors predictive of RFS and OS after RC. All analyses were done with SAS 9.4.
Results:
The study included 1885 patients, 13.5% of whom underwent RARC. There was no difference in positive soft tissue surgical margins (2.4% in ORC and 1.2% in RARC). There were no differences in recurrence patterns, nor in the severity of pathology distribution between the two cohorts. Peritoneal carcinomatosis was seen in 1.1% of ORC and 0.8% in RARC. Shorter RFS was associated with younger age (hazard ratio [HR] 1.04, 95% confidence interval [CI] 1.03–1.05, p < 0.001), neoadjuvant chemotherapy (HR 1.41, 95% CI 1.14–1.75, p = 0.002), higher pathologic stage (stage ≥T2 HR 2.45, 95% CI 1.91–3.16, p < 0.001), lymph node positivity at cystectomy (HR 1.92, 95% CI 1.50–2.47, p < 0.001), and positive surgical margins (HR 1.49, 95% CI 1.09–2.05, p = 0.01). RFS and OS did not differ by surgical approach (HR 1.04, 95% CI 0.83–1.30), p = 0.75 and (HR 0.89, 95% CI 0.67–1.19), p = 0.43, respectively.
Conclusion:
The data from this study support continued use of RARC as a safe oncologic procedure, with similar outcomes to ORC.
Introduction
Innovative minimally invasive approaches to perform radical cystectomy (RC) for the management of bladder cancer (BC) have evolved rapidly. However, it remains unclear whether the robotic surgery platform provides comparable oncologic outcomes to the open approach. Two randomized trials have shown that the use of robot-assisted radical cystectomy (RARC) provides noninferior oncologic outcomes compared to open radical cystectomy (ORC). 1,2 An additional radmozed trial compared RARC, ORC, and laparoscopic RC, which also demonstrated no difference in oncologic outcomes. 3 Despite these results, questions remain regarding the location and pattern of recurrences. Although RARC appears to confer less blood loss, higher lymph node (LN) counts, and shorter postoperative length of stay when compared to ORC, these potential benefits would be rendered irrelevant if oncologic excellence was attenuated or compromised. 4,5 The adoption of robotic surgery for most major urologic oncology procedures has occurred rapidly, despite a lack of long-term oncologic outcomes data supporting this trend. 6,7 The utilization of RARC in particular has been increasing annually, and it is currently estimated that nearly 25% of all cystectomies are RARC. 4 Oncologic outcomes are arguably the most important, and yet have been the last to be formally examined. 6,7
Recently, Ramirez and colleagues published data from the Laparoscopic Approach to Cervical Cancer (LACC) trial, which was closed early owing to the finding that minimally invasive (laparoscopic or robot assisted) radical hysterectomy for early stage cervical cancer was associated with lower rates of disease-free and overall survival (OS). 8 Subsequently, the U.S. Food and Drug Administration (FDA) released a safety communication to patients and providers advising that “the relative benefits and risks of surgery using robotically assisted surgical devices compared to conventional surgical approaches in cancer treatment have not been established.” Crucially, the communication also encourages the maintenance of patient registries to gather data and help characterize outcomes. 9 As utilization increases, and in light of ongoing concerns, evidence from large retrospective series remains important to provide critical safety and oncologic efficacy information within a “real-world” population, outside of the narrowly defined scope of clinical trials. 10,11 In addition, the historically high volume of our tertiary care cancer center and the outcomes achieved by the ORC surgeons present a challenging bar to meet for oncologic outcomes.
Patients undergoing RC with any approach face multiple factors that determine oncologic and functional outcomes. Quality metrics for RC include negative surgical margins and an adequate LN dissection; both of these factors have an independent influence on recurrence-free survival (RFS) and OS. Clearly, positive margins are associated with more advanced BC, however, the rate of positive margins should remain low, regardless of surgical technique. 12 Persistence of low pathologic positive margin incidence is of utmost importance in maintaining the surgical integrity of both ORC and RARC, as is understanding the recurrence patterns between the techniques. 13 We sought to provide the pathologic outcomes and recurrence patterns of patients undergoing RARC and ORC from a large retrospective cohort.
Materials and Methods
We employed a retrospective cohort study with propensity matching. The study comprised all patients undergoing an RC for BC by either an RARC or ORC approach at a single, high-volume tertiary care center, between 2005 and 2017. The majority of the RARCs were done in 2013 and after that, RARC make up 1/3 of the volume since that time. Of the RARC, >90% were done in an intracorporeal manner; thus; this was not included as a predictive factor. Institutional Review Board approval was obtained. A total of 1885 cases were identified over the time period. All procedures included a bilateral pelvic LN dissection and urinary diversion. Each RC was completed by a fellowship-trained urologic oncologist, all of whom had significant experience and were past their learning curve (>50 robotic pelvic cases). Patients underwent either RARC or ORC based on patient and surgeon preference. Patients were clinical stage ≤T4N0M0 and all histologic subtypes were included. Additional staging was completed with cross-sectional imaging and a chest X-ray if there was no cross-sectional imaging of the chest. Follow-up for recurrence was performed according to the National Comprehensive Cancer Network guidelines. 14 RC specimens were reviewed by a genitourinary pathologist. Neoadjuvant chemotherapy (NAC) was administered for eligible high-risk patients based on previously described risk allocation (lymphovascular invasion [LVI], variant histology, clinically palpable disease, and hydronephrosis). 15 Follow-up was completed by mailed surveys and clinic visits. Pathologic and clinical outcomes were divided into ≤T1 and ≥T2 for analysis. Margins were divided into the following categories: negative, soft tissue, ureteral, and urethral. Soft tissue margins were anything other than ureteral or urethral.
Outcome measures
The primary outcome was a comparison of the incidence of positive surgical soft tissue margins for patients undergoing ORC and RARC. Secondary outcomes were loco-regional recurrence patterns, RFS and OS.
Statistical analysis
Patient characteristics were summarized by surgical approach using descriptive statistics. Differences between continuous variables were compared using Wilcoxon rank-sum tests, and differences between categorical variables were compared using Fisher's exact tests or chi-square tests as appropriate. RFS was defined as the time interval between date of surgery and date of disease recurrence or date of death, whichever occurred first. Patients who were alive and without disease recurrence at the last follow-up were censored at that time. OS was defined as the time interval between date of surgery and date of death, and was censored at the last follow-up date for patients who were alive. RFS and OS were estimated using the Kaplan–Meier method, and differences among subgroups were assessed using log-rank tests. 16 Cox-proportional hazards regression models were fit to assess the association between patient characteristics and RFS or OS. 17 Kaplan–Meier cohorts were mutually exclusive, and if patients had a positive margin, they were grouped with that cohort regardless of pathology status.
Propensity score matching with inverse probability weighting on a 2:1 ratio was implemented to reduce the possibility of selection bias on the surgical approach and included age at diagnosis, gender, clinical stage, and NAC. Weighted Cox-proportional hazards regression models with robust standard errors were applied to assess the association between patient characteristics, RFS and OS. All statistical analyses were performed using SAS 9.3 and Splus 8.2. STROBE guidelines were followed for reporting.
Results
There were 1630 patients treated with ORC and 255 treated with RARC. There was no difference in demographics between the two cohorts. There was no difference in clinical staging between the two cohorts and the collapsed categories of ≤T1 and ≥T2 (35.8% of ORC and 35.3% of RARC were ≤T1, p = 0.88). Similarly, there was no difference in the pathologic stages between the two cohorts. Patients who had pathologic stages ≤T1 made up 54.6% of the ORC cohort and 59.6% of the RARC cohort (p = 0.13). In addition, there was no difference in the nodal stage for the RARC and ORC groups (p = 0.11). More patients in the RARC cohort underwent NAC, 51.8% compared to 43.6% for those in the ORC group (p = 0.02). The median number of LNs counted were higher in the RARC compared to the ORC cohort (27 nodes vs 22, p < 0.001). More patients in the ORC cohort had LVI identified in the surgical specimen (24% compared to 15.7%, p = 0.003).
There were no statistically significant differences in soft tissue or overall positive margin rates between the two groups (7.1% of the ORC cohort vs 4.7% of the RARC cohort, p = 0.16). Furthermore, there was no statistical difference with respect to the location of positive margins (p = 0.26). Soft tissue margins were positive in 2.4% of ORC patients and 1.2% in RARC patients. Ureteral margins were positive in 1.7% of ORC cases and 2.4% of RARC cases. Urethral margins were positive in 2.3% of ORC patients and 1.2% of RARC patients. Table 1 details patients who had positive margins and their pathologic stages, none of which had significant differences between the ORC and RARC cohorts.
Baseline Characteristics of Patients Treated with Open Radical Cystectomy and Robot-Assisted Radical Cystectomy
LN = lymph node; ORC = open radical cystectomy; RARC = robot-assisted radical cystectomy; UCC = urothelial carcionoma.
Cancer reoccurred in 29.2% of the patients treated with ORC and in 20% of those who underwent RARC. Distant metastases were detected in 18.2% of patients undergoing ORC and in 13.7% after RARC. The most common sites of distant metastasis were lungs (6.3% for ORC and 4.7% for RARC), followed by the extrapelvic LNs (5.1% for ORC and 4.7% for RARC). Peritoneal carcinomatosis was rare in both cohorts (1.1% for ORC and 0.8% for RARC). Local recurrences, most commonly in the cystectomy bed, occurred in 5.6% of the ORC cohort and 3.9% of the RARC cohort and infield nodal recurrences were rare (1.2% for ORC and 0.8% for RARC). Secondary urothelial cancers were seen in 4.3% of the ORC patients and 1.6% of the RARC patients. Table 2 shows the recurrence patterns after ORC and RARC.
Distribution of Locations Among Patients with Recurrence and Secondary Urothelial Carcinomas
PLND = pelvic lymph node dissection.
On multivariable analysis after propensity matching, patients with positive surgical soft tissue margins had a 49% (hazard ratio [HR] 1.49, 95% confidence interval [CI] 1.09–2.05) greater chance of recurrence compared to those with negative margins (p = 0.01), details in Table 3. Recurrence of BC after RC was not associated with surgical technique, HR 1.04 (95% CI 0.83–1.30, p = 0.75). Figure 1 shows the associated Kaplan–Meier graphs for RFS in ORC and RARC. Recurrence was associated with a younger age at the time of RC, HR 1.04 (95% CI 1.03–1.05, p < 0.001), and in those treated with NAC, HR 1.41 (95% CI 1.14–1.75, p = 0.002). Pathologic stage ≥T2 was most predictive of RFS with an HR of 2.45 (95% CI 1.91–3.16, p < 0.001). Both LVI and pathologic nodal status were also predictive of RFS (p < 0.001). Supplementary Figure S1a–d contain the Kaplan–Meier graphs with RFS stratified by pathologic categories.
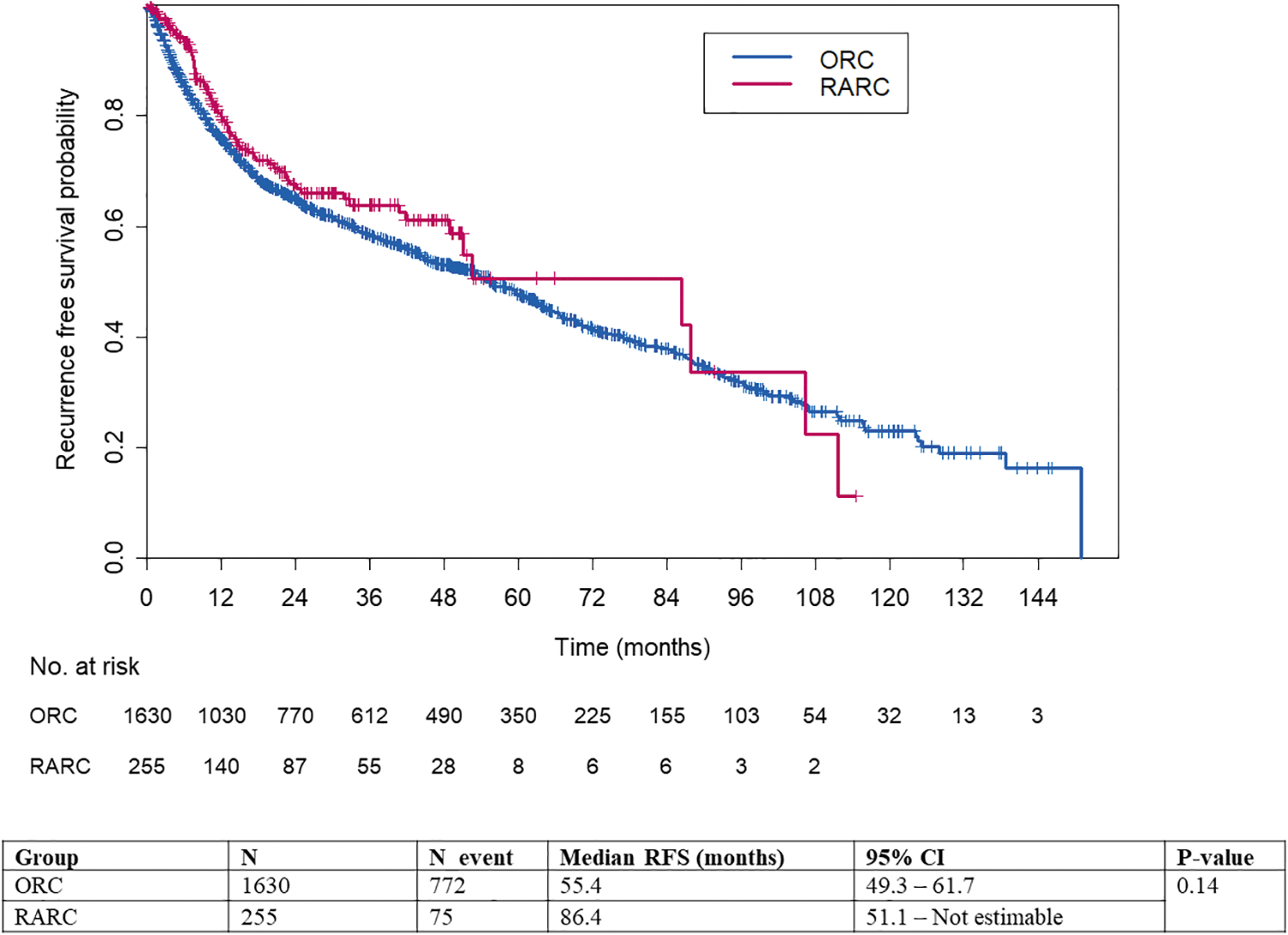
This shows the associated Kaplan–Meier graphs for RFS in ORC and RARC. Recurrence was associated with a younger age at the time of RC, HR 1.04 (95% CI 1.03–1.05, p < 0.001), and in those treated with neoadjuvant chemotherapy, HR 1.41 (95% CI 1.14–1.75, p = 0.002). Pathologic stage ≥T2 was most predictive of RFS with an HR of 2.45 (95% CI 1.91–3.16, p < 0.001). Both LVI and pathologic nodal status were also predictive of RFS (p < 0.001). CI = confidence interval; HR = hazard ratio; LVI = lymphovascular invasion; ORC = open radical cystectomy; RARC = robot-assisted radical cystectomy; RFS = recurrence-free survival. Color images are available online.
Multivariable Cox Regression Analysis of Variables Associated with Recurrence After Radical Cystectomy (Recurrence-Free Survival), After Inverse Probability of Weighted Adjustment by Propensity Score
CI = confidence interval; HR = hazard ratio; LVI = lymphovascular invasion.
OS for patients after RC was significantly associated with age and pathologic features on multivariable analysis, details in Table 4. Pathologic stage ≥T2 remained the factor most associated with survival, HR 2.52 (95% CI 1.88–3.38, p < 0.001). LVI and pathologic positive LN were also associated with poorer OS (HR 1.56, 95% CI 1.16–2.10 and HR 1.93, 95% CI 1.45–2.57, p = 0.003 and p < 0.001, respectively). The Kaplan–Meier graph for OS is seen in Figure 2, the median follow-up for OS was 53.6 months for ORC and 22.3 months for RARC patients. Supplementary Figure S2a–d contain the Kaplan–Meier graphs with OS stratified by pathologic categories. Figures 3 and 4 show the Kaplan–Meier graphs for RFS and OS for ORC and RARC broken down by no tumor on pathology, ≤T1, ≥T2, or nonorgan-confined BC as defined by the patient's worst pathologic features.

This shows the associated Kaplan–Meier graph for OS in ORC and RARC. OS for patients after RC was significantly associated with age and pathologic features on multivariable analysis, details in Table 4. Pathologic stage ≥T2 remained the factor most associated with survival, HR 2.52 (95% CI 1.88–3.38, p < 0.001). LVI and pathologic positive LN were also associated with poorer OS (HR 1.56, 95% CI 1.16–2.10 and HR 1.93, 95% CI 1.45–2.57, p = 0.003 and p < 0.001, respectively). The median follow-up for OS was 53.6 months for ORC and 22.3 months for RARC patients. LN = lymph node; OS = overall survival. Color images are available online.
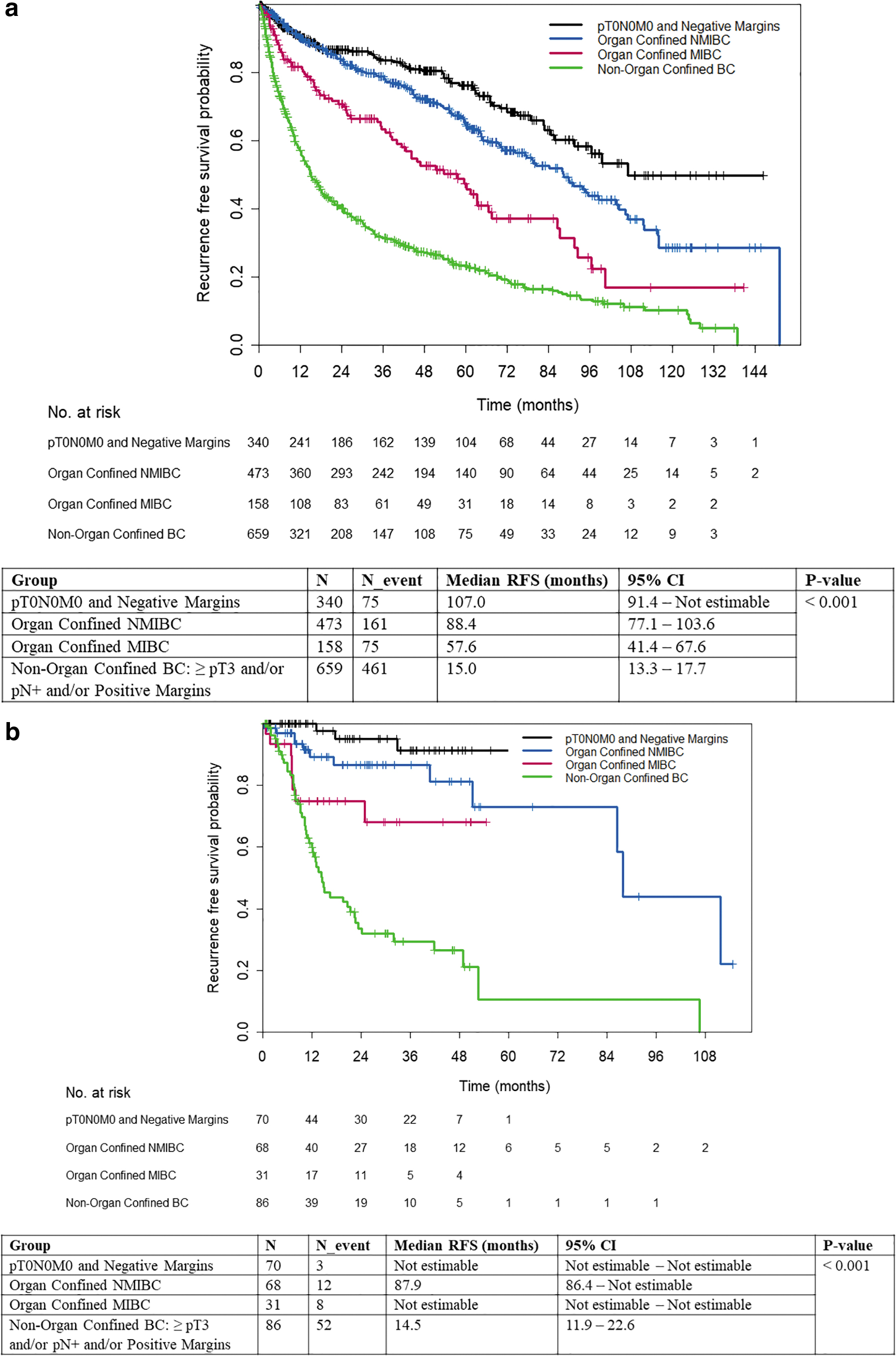
This shows the Kaplan–Meier curves for RFS in ORC and RARC for different pathologic stages. The nonorgan confined had, as expected, the worst survival and the pT0N0M0 and negative margins conferred the best survival. Color images are available online.
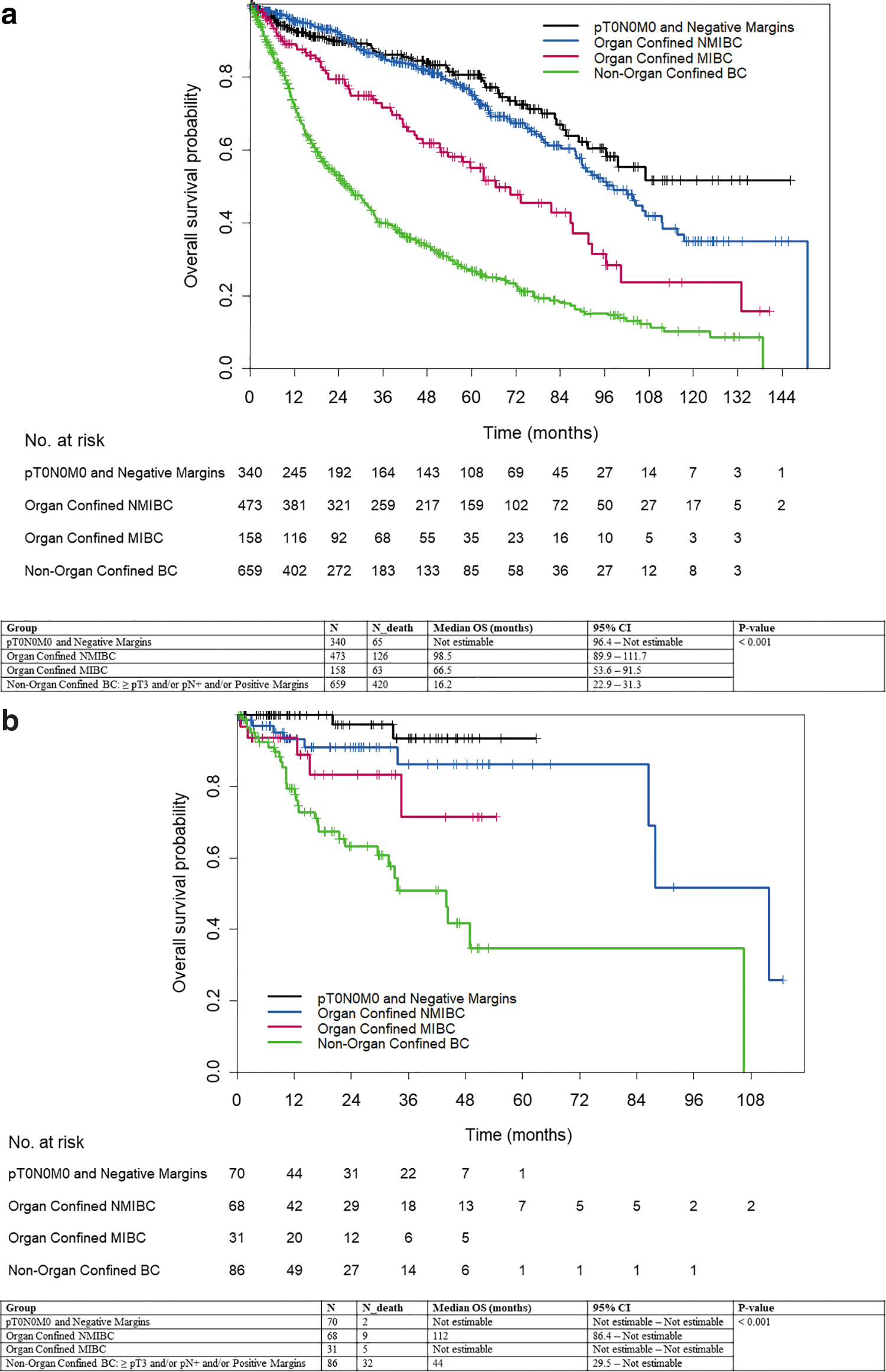
This shows the Kaplan–Meier curves for OS in ORC and RARC for different pathologic stages. The nonorgan confined had the worst OS and the pT0N0M0 and negative margins conferred the best OS. Color images are available online.
Multivariable Cox Regression Analysis of Variables Associated with Overall Survival After Radical Cystectomy, After Inverse Probability of Weighted Adjustment by Propensity Score
Discussion
This large, propensity-matched cohort comparison between patients undergoing ORC and RARC found few differences between surgical technique and oncologic outcomes. OS and RFS were dictated by pathologic stage and not factors intrinsically tied to either surgical technique. A key finding was both cohorts had acceptably low rates of positive soft tissue margins and similar recurrence patterns and rates. As expected, the occurrence of a positive margin influenced both RFS and OS. This observation supports the associations described in several previous investigations. 4,18,19 Interestingly, survival after a positive surgical margin in this study was better than what has been described previously. For instance, Moschini and coworkers reported an almost 3-fold increase in the risk of recurrence, which was double the 1.5-fold risk identified in this study. However, in both cases, the occurrence of a positive margin was marked by significant reductions in both RFS and OS. 20
Surgical quality has long been associated oncologic outcomes after RC and is dependent upon multiple factors. For instance, better outcomes are reported for high-volume RC centers. 21,22 Adequate LN dissection is also identified as a predictor of BC survival and is recognized as a quality metric after RC. In this study, LN yield was greater after RARC, but this observation is confounded by the routine practice among the ORC surgeons to send the pelvic LNs in fewer packets. 23 –25
Sathianathen et al. recently performed a systematic review and meta-analysis of randomized trials comparing ORC to RARC. 26 In addition to finding similar oncologic efficacy, randomized data have demonstrated that RARC confers lower blood loss and a decreased length of stay, contributing to its value. 26,27 Despite these possible benefits of robotic surgery, employing a new technique necessitates a demonstration of oncologic equipoise. Unlike other urologic cancers, reliable salvage treatments are lacking for BC and as a result any reduction in surgical quality rightfully raises red flags. This concern is augmented by demonstrations of distinct differences in the patterns of recurrence from reported randomized studies. 1,28 Data informing the management of cervical cancer have suggested that minimally invasive surgery is associated with lower rates of disease-free survival and OS than open approaches, potentially attributable to the use of a uterine manipulator or the unique effect of insufflation on cervical tumor cell growth or spread. 8,29 In addition, although noninferiority for progression free survival (PFS) has been demonstrated in a randomized clinical trial for BC, a criticism of the recently published multi-institutional RAZOR study points to the relatively high noninferiority threshold of 15%. 2
Our large study aims to diffuse these concerns and despite its retrospective nature, provides robust data demonstrating that RFS and OS rates are comparable between both surgical approaches. Furthermore, taken in the context of a high-volume, tertiary referral center where the established oncologic outcomes among ORC patients exceed the outcomes realized nationally, the bar set by ORC was exceptionally high for RARC to match. As a result, the finding of oncologic equipoise across all relevant domains provides complimentary data to the currently published prospective trials. Also, our study mitigates the criticism of the large threshold chosen by the RAZOR investigators.
Limitations of this study include the long study period during which time practice patterns may have changed. For example, more NAC use was observed in the RARC group, potentially reflecting contemporary changes to guidelines in administering NAC before RC. Alternatively, the greater use of NAC in the RARC cohort may suggest that the RARC patients were more commonly candidates for such therapy. OS was significantly higher in the RARC group, and may again reflect a selection bias in which patients who were healthier were selected for RARC. However, longer life expectancy and lack of comorbidities would not bias the positive margin incidence or RFS. We also did not have access to the smoking history or current smoking status of patients, nor did we have access to adjuvant chemotherapy use, which may have further influenced OS. The latter would not, however, have impacted the positive margin incidence, which was the primary outcome of the study. We did not present complication and safety data; however, there was no difference between these in the RARC and ORC groups. In addition, follow-up was shorter in the RARC group; however, most recurrences in urothelial cancer happen within the first 2 years; thus a median follow-up of 22 months should capture the highest volume of recurrences. Finally, hospital stay for RC is highly variable based on country as well as the presence of an enhanced recovery program; thus, hospital stay may be more relevant to some than others. Despite these limitations, strengths of this study include its large sample size and use of propensity matching to mitigate such confounders.
Despite concerns raised both in the lay press and in the medical literature regarding the safety of robotic surgery for certain oncologic operations, this study confirms that for BC, RARC is associated with low positive margin rates that are not statistically different from ORC when performed at a high-volume center by experienced surgeons. 8 Also, the location of positive surgical margins does not vary by surgical modality, nor do OS and RFS rates. Patients should continue to receive careful and thorough counseling of risks and benefits before proceeding with either surgical approach. RARC remains a safe and effective oncologic procedure, and should remain an option for the treatment of BC as specified in recent guidelines by the European Association of Urology Guidelines. 30 Patients should have an informed discussion with their provider to determine which surgical approach is most appropriate for them.
Conclusion
Surgical quality as evidenced by negative surgical margins at RC is the most important modifiable factor in patients undergoing RC for BC. RARC remains a promising technology, which is oncologically equivalent to ORC, resulting in similar RFS and OS rates.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.