
Abstract
Introduction:
We sought to identify the factors associated with deterioration of renal functions after robot-assisted radical cystectomy, and to develop a nomogram to detect the probability of progression to chronic kidney disease (CKD).
Materials and Methods:
A retrospective review of our prospectively maintained database. Estimated glomerular filtration rate (eGFR) was calculated using the CKD-Epidemiology Collaboration creatinine formula utilizing all follow-up creatinine values. CKD was defined as stage 3b (eGFR <45 mL/minute/1.73 m2) based on the National Kidney Foundation classification. Kaplan–Meier curves were used to depict CKD-free survival. A multivariate Cox regression model was used to determine predictors for CKD and to build the perioperative nomogram.
Results:
The data set comprised 442 patients with a median follow-up of 25 months (12–59). Thirty-seven percent developed CKD at a median of 9 months (4–18). CKD-free survival rates at 1, 3, and 5 years were 75%, 58%, and 50%, respectively. CKD was significantly associated with preoperative eGFR (hazards ratio [HR]: 0.96, 95% confidence interval [CI]: 0.95–0.97, p < 0.01), body mass index (HR: 1.03, 95% CI: 1.01–1.05, p = 0.03), Charlson Comorbidity Index ≥3 (HR: 2.20, 95% CI: 1.35–3.58, p < 0.01), diabetes (HR: 1.59, 95% CI: 1.09–2.31, p = 0.02), 90 days postoperative strictures (HR: 4.04, 95% CI: 1.76–9.30, p < 0.01), 90 days postoperative hydronephrosis (HR: 2.26, 95% CI: 1.34–3.79, p < 0.01), 90 days recurrent urinary tract infection (HR: 1.84, 95% CI: 1.08–3.14, p = 0.02), 90 days acute kidney injury (HR: 1.70, 95% CI: 1.19–2.43, p < 0.01), and node positive disease (HR: 1.94, 95% CI: 1.31–2.86, p < 0.01). A 5-year CKD-free survival nomogram was developed.
Conclusion:
We have developed and cross-validated a nomogram for detecting CKD-free survival. This nomogram may have a role in counseling and follow up of patients. This study was done after the approval of the IRB committee (I-79606).
Introduction
Bladder cancer is the ninth-most common tumor worldwide with 81,190 estimated new cases and 17,240 estimated deaths in the United States in 2018. 1 Radical cystectomy (RC) with pelvic lymphadenectomy and urinary diversion is the standard of care for surgical management of organ-confined muscle invasive bladder cancer and refractory nonmuscle invasive disease. 2 Robot-assisted radical cystectomy (RARC) has risen from 0.6% in 2004 to 32.4% of cystectomies in 2017 in the United States. 3 RARC has provided equivalent early oncologic outcomes to open RC, and probably superior when it comes to perioperative outcomes. 4 However, RC remains a morbid procedure with high complication rate, most of which are diversion related. 5 Among the long-term complications of urinary diversion is deterioration of renal function. 6,7
Chronic kidney disease (CKD) is associated with higher risk of cardiovascular disease, immunodeficiency, prolonged hospitalization, as well as recurrence and mortality rate. 8,9 While bladder cancer is one of the most expensive cancers to treat, the presence of CKD may pose an additional health care and economic burden. 10 Nomograms have been widely accepted by physicians as tools for assessing patient prognosis. We sought to identify the factors associated with deterioration of renal functions after RARC, and to develop a nomogram to detect the probability of progression to CKD.
Materials and Methods
A retrospective review of our quality assurance institutional database of 630 patients who underwent RARC between 2005 and 2019 was performed (I-79606). Patients with incomplete data, preoperative CKD (estimated glomerular filtration rate [eGFR] <45 mL/minute/1.73 m2), or <3 months of follow-up were excluded (Fig. 1). Data were reviewed for preoperative characteristics, operative, and postoperative outcomes. Patients were divided into those who developed CKD [defined as stage 3b (<45 mL/minute/1.73 m2) based on the National Kidney Foundation classification at least 90 days after RARC] and those who did not.
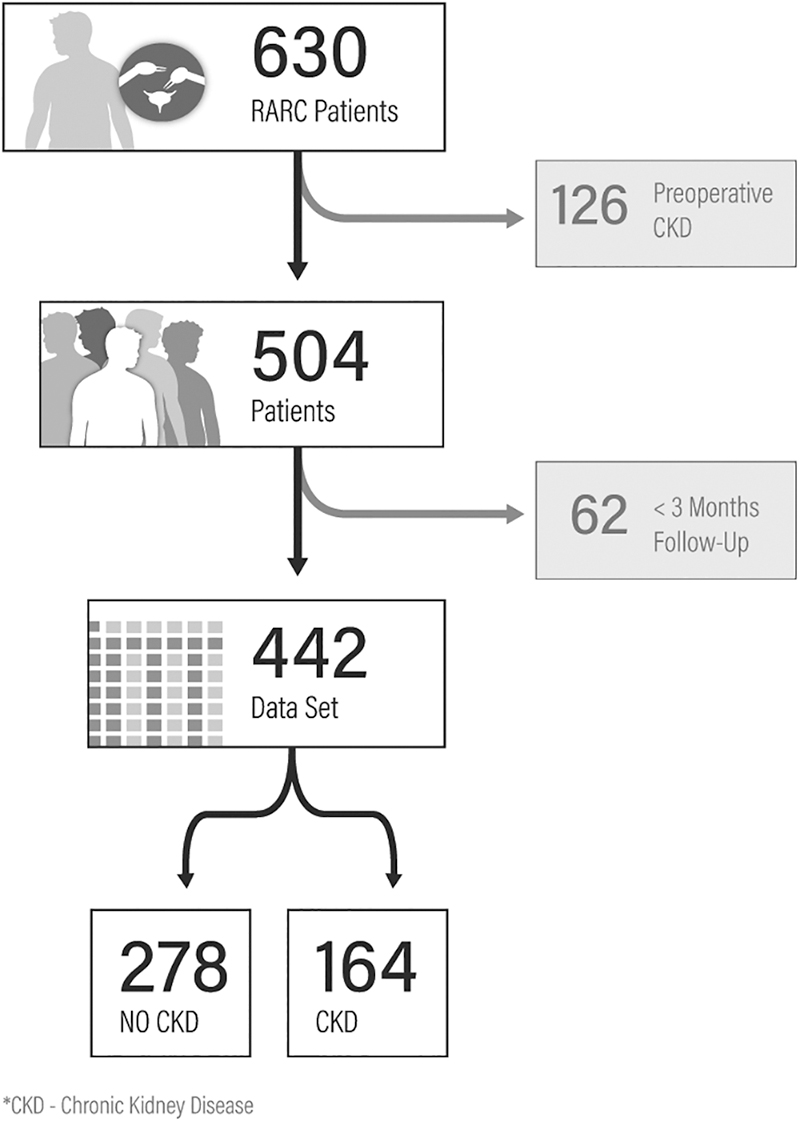
Flowchart of patient selection.
eGFR was computed using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine formula utilizing all follow-up creatinine values (excluding the first 3 months post-RARC). Acute kidney injury (AKI) was defined as an abrupt (within 48 hours) reduction in kidney function, defined as an absolute increase in serum creatinine of more than or equal to 0.3 mg/dL (≥26.4 μmol/L), or a percentage increase in serum creatinine of more than or equal to 50% (1.5-fold from baseline). 11 Urinary tract infections (UTIs) were defined as the presence of positive urine culture (≥105 cfu/mL with no more than two organisms) and documented urinary symptoms, including fever (≥38°C), chills, flank, or abdominal pain.
Data were analyzed with double-sided t-test and Wilcoxon test and described in terms of means ± standard deviations (SDs) and median (interquartile range [IQR]). Multivariable stepwise Cox regression model was used to depict predictors of CKD. The Kaplan–Meier method was used to compute CKD. After 90 days, an eGFR <45 mL/minute/1.73 m2 was considered an event; the duration from day 90 to the date of event/censor is defined as survival time. The nomogram prognosticators included preoperative, operative, and 90-day postoperative variables based on the multivariate model. The nomogram was constructed to provide visual explanation for predicted probabilities of a survival outcome, as obtained by the statistical predictive model. The point system was carried out in scoring based on the weighted relative importance of individual risk factors, and individual 1-, 2-, 3-, 4-, and 5-year CKD-free survival probability.
The utility of the nomogram was evaluated using time-dependent receiver operating characteristic (ROC) curves, area under the curve (AUC), calibration plots, and prediction errors. Standard cross-validation techniques were used to generate these measures. All tests were two sided, with statistical significance defined as p ≤ 0.05. All statistical analyses were performed using SAS® software (version 9.4; SAS Institute, Inc., Cary, NC) and R® software 3.6.1.
Results
The final cohort included 442 patients with a median follow-up of 25 months (IQR 12–59). Thirty-seven percent developed CKD at a median time of 9 months (IQR 4–18). Patients who developed CKD were older (70 ± 9 years vs 66 ± 11 years, p < 0.01), had Charlson Comorbidity Index (CCI) ≥3 more frequently (87% vs 73%, p < 0.01), and had a lower mean preoperative eGFR (68 mL/minute/1.73 m2 vs 82 mL/minute/1.73 m2, p < 0.01). There was no statistical difference between the groups with regard to body mass index (BMI) (p = 0.08), race (p = 0.48), American Society of Anesthesiology (ASA) ≥3 (p = 0.69), receipt of neoadjuvant chemotherapy (NAC) (p = 0.12), rate of intracorporeal urinary diversion (p = 0.73), ileal conduit urinary diversion (p = 0.54), estimated blood loss (p = 0.26), and operative time (p = 0.86).
Patients who developed CKD experienced a higher rate of overall (91% vs 80%, p < 0.01) and high-grade complications (54% vs 27%, p < 0.01). There was no significant difference in terms of ≥pT3 (36% vs 31%, p = 0.40), positive soft tissue surgical margins (4% vs 6%, p = 0.28), node-positive disease (pN+ve) (22% vs 19%, p = 0.54), and recurrence rates (29% vs 26%, p = 0.51) (Table 1).
Baseline and Perioperative Characteristics
Boldface indicates significant values.
BMI = body mass index; CCI = Charlson Comorbidity Index; CKD = chronic kidney disease; IQR = interquartile range; NAC = neoadjuvant chemotherapy; pN+ve = node positive disease; SD = standard deviation.
CKD-free survival rates at 1, 3, and 5 years were 75%, 58%, and 50%, respectively (Fig. 2). CKD was significantly associated with preoperative eGFR (hazards ratio [HR]: 0.96, 95% confidence interval [CI]: 0.95–0.97, p < 0.01), BMI (HR: 1.03, 95% CI: 1.01–1.05, p = 0.03), CCI ≥3 (HR: 2.20, 95% CI: 1.35–3.58, p < 0.01), diabetes (HR: 1.59, 95% CI: 1.09–2.31, p = 0.02), 90-day postoperative ureteroileal strictures (HR: 4.04, 95% CI: 1.76–9.30, p < 0.01), 90-day postoperative hydronephrosis (HR: 2.26, 95% CI: 1.34–3.79, p < 0.01), 90-day recurrent UTI (HR: 1.84, 95% CI: 1.08–3.14, p = 0.02), 90-day AKI (HR: 1.70, 95 % CI: 1.19–2.43, p < 0.01), and pN+ve (HR: 1.94, 95% CI: 1.31–2.86, p < 0.01) (Table 2). A 5-year CKD-free survival nomogram was developed based on these predictors (Fig. 3). The strongest predictor for CKD was baseline eGFR.
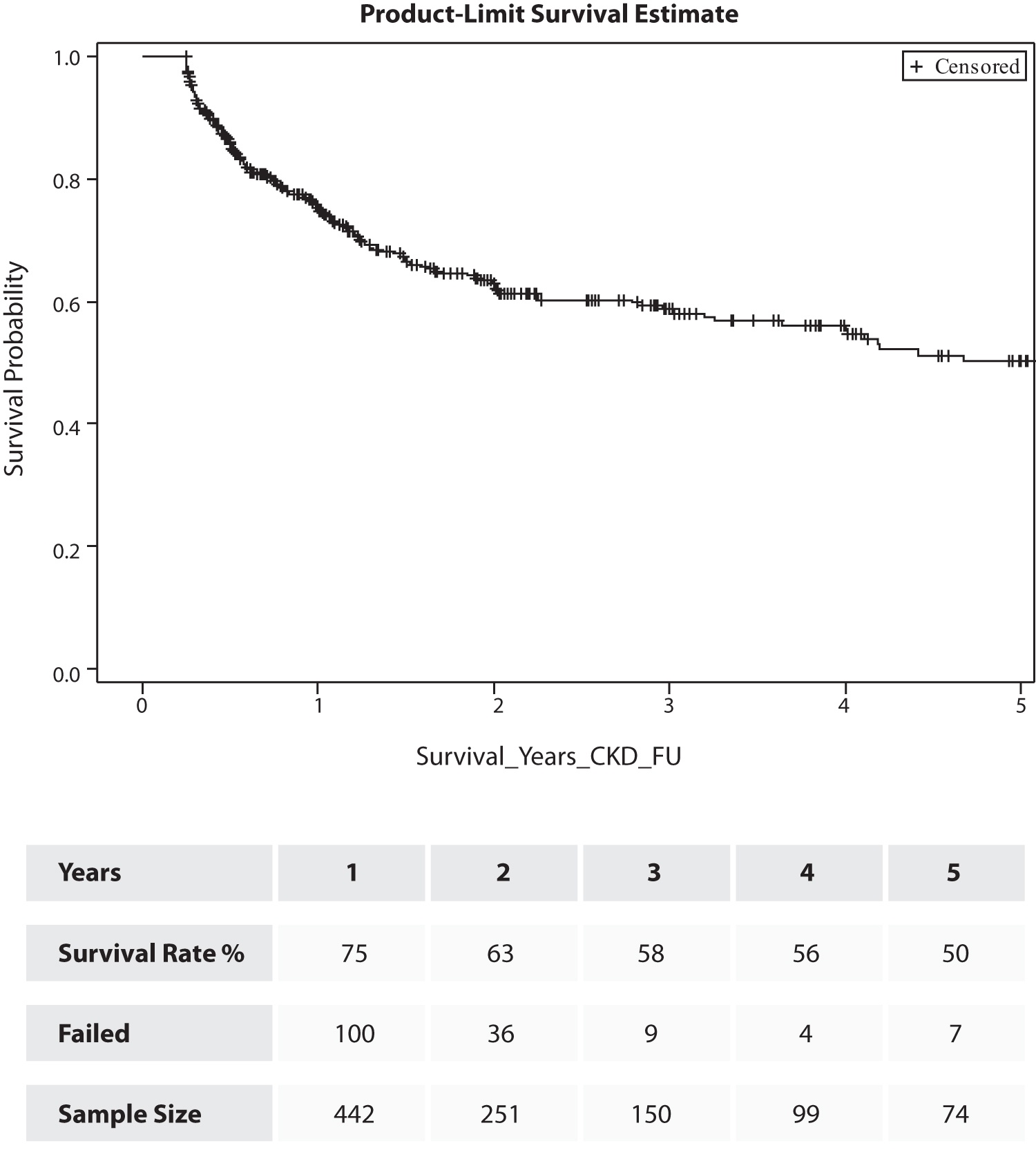
Kaplan–Meier curve showing CKD-free survival. CKD = chronic kidney disease.

Nomogram for prediction of chronic kidney disease after RARC. PR = predicted; RARC = robot-assisted radical cystectomy.
Multivariate Analysis Predicting Chronic Kidney Disease
AKI = acute kidney injury; eGFR = estimated glomerular filtration rate; UTI = urinary tract infection.
The quantified ROC curve was plotted, and the AUC at year 1 to 5 was 0.77, 0.79, 0.77, 0.77, and 0.78, respectively (Fig. 4). Calibration plots for CKD-free survival probability at all 5 years showed acceptable calibration, and the predictions reasonably approximated actual survival probabilities. On average, our model slightly underestimates the CKD-free survival rates by less than 0.5%; the SD of prediction error is controlled to a range of 2.6% to 4.2% (Fig. 5).
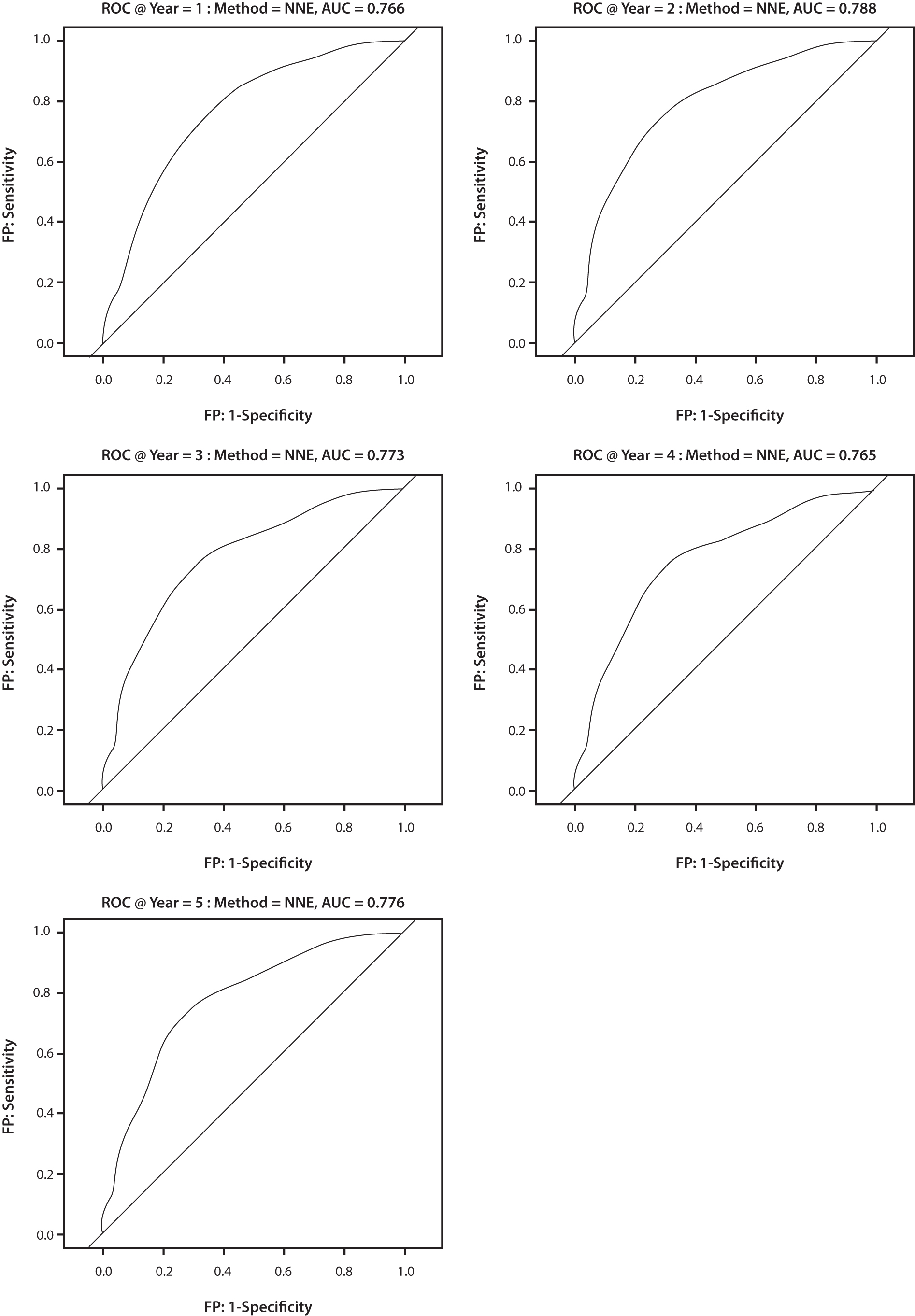
Receiver operation curve showing the accuracy of the nomogram at years 1, 2, 3, 4, and 5, respectively. FP = false positive.

Calibration plots for estimating CKD-free survival at 1, 2, 3, 4, and 5 years.
The use of the nomogram is best illustrated with an example. Assume a patient has been diagnosed with refractory nonmuscle invasive bladder cancer and he underwent RARC after patient counseling. The patient has a baseline eGFR of 90, and BMI of 35. He did not receive NAC. He developed postoperative stricture, hydronephrosis, and recurrent UTI. At the 3-month follow-up, the patient will be counseled regarding his CKD-free survival. His scores based on the nomogram will be 44, 15, 43, 25, and 19, respectively. The sum of the scores is 146 points. The CKD-free survival for this patient based on the nomogram is 50% at 1 year and 10% at 5 years (Fig. 6).
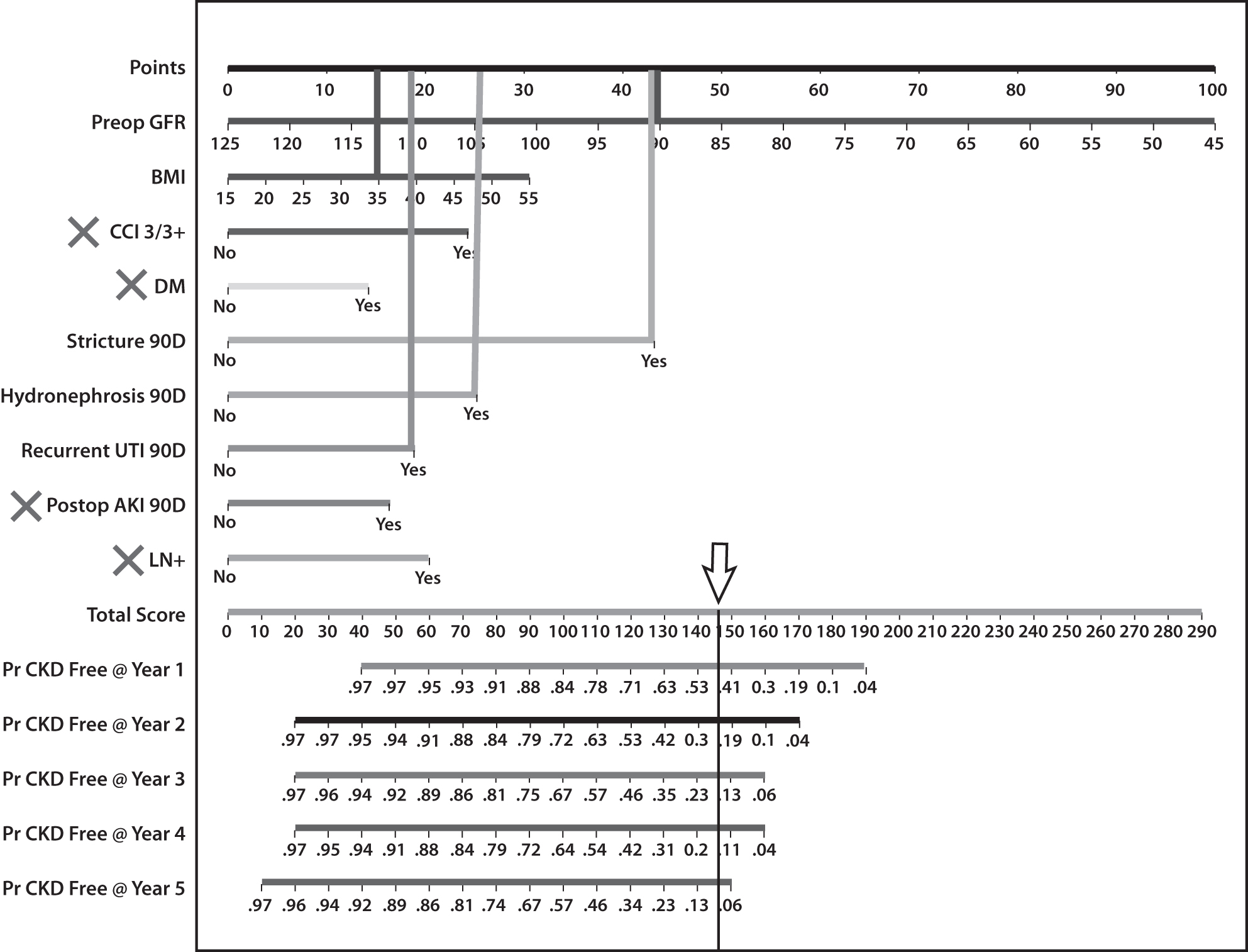
Example of how to use the nomogram.
Discussion
Approximately 70% of patients undergoing RC with urinary diversion experience renal function decline regardless of type of diversion. 12 The presence of CKD significantly affects the management of bladder cancer patients, alters decisions for treatment, and can also affect patients' prognosis. CT imaging with contrast is the mainstay for diagnosing and follow up of bladder cancer. CKD may hinder patients from receiving CT scans. CKD will deem the patient ineligible for chemotherapy whether neoadjuvant or adjuvant. 13 Significant reduction in kidney function is considered by many an absolute contraindication for continent urinary diversion; although some studies (including the current) did not find a significant association between the type of diversion and probability of CKD. 2,14 A systematic review and meta-analysis found that preoperative CKD is associated with a significantly worse recurrence-free, disease-specific, and overall survival. 15 Another has shown that CKD was an independent risk factor for bladder/upper urinary tract tumor recurrences and overall survival among patients with nonmuscle invasive bladder cancer. Thus, preservation of renal function should be one of the primary goals after RC and urinary diversion. Previous reports have studied several predictors for poor renal function after RC. 16 However, there is a lack of nomograms to predict the probability of CKD after RARC. In this study, we developed a nomogram to predict long-term renal functions for patients undergoing RARC.
Previous studies have used serum creatinine, nuclear imaging, and eGFR to calculate renal function. We have used the eGFR based on the CKD-EPI creatinine formula, which was proven accurate and comparable with the Modification of Diet in Renal Disease formula especially in older age (>65). 17 There is lack of a standardized definition for renal function deterioration after RC. A study that has looked into long-term renal function after RC has defined decreased renal function as a decrease in eGFR >10 mL/minute/1.73 m2. 16 Hautmann and colleagues defined a 25% decline in eGFR from baseline as renal function decline, and Jin and colleagues and Eisenberg and colleagues defined the decline as a 10% decline in eGFR from baseline. 16,18,19 It is evident that a certain level of decline in renal function is expected after urinary diversion, but no clear evident threshold value has been determined for renal function decline after urinary diversion. We chose CKD stage 3b as a threshold as this was associated with worse progression-free, cancer-specific, and overall survival. 20
Prevalence of CKD after RC varies widely in the literature. In the Mayo Clinic series, 20% of patients undergoing RC progressed to CKD (stage III–V) after a median follow-up of 5.8 years. 21 Mayo Clinic did not exclude patients with preoperative CKD, which could explain the lower percentage of progression as these patients probably received an extensive nephrologic evaluation and follow-up. Jin and colleagues have demonstrated an incidence rate of CKD (stage III–V) of 26% and 17% for ileal conduit and orthotopic urinary diversions, respectively, at 10 or more years after surgery. 16 Our CKD incidence rate is 37%, which was defined as stage ≥3b compared with Jin and colleagues, which was defined as stage ≥3a.
The importance of baseline eGFR is well established for patients undergoing partial nephrectomies. This might be attributed to the presence of the inevitable impact of aging and medical comorbidities, which is supported by the findings of Simmons and colleagues showing that the kidney tissue quality, as measured by baseline eGFR, has a significant effect on the long-term renal function outcomes after partial nephrectomy. 22 Baseline eGFR was the strongest predictor for CKD-free survival in our nomogram as suggested by previous extensive literature for partial nephrectomies.
BMI, CCI ≥3, and diabetes were all significant in our model. Obesity is often associated with diabetes and hypertension as a part of the metabolic syndrome. Studies have shown that obesity is a preventable risk factor for renal function deterioration and although hypertension and type 2 diabetes are important mediators, additional pathways may exist. 23 Higher BMI increases the complexity of the procedure, which may increase the operative time, predisposing to AKI, which also increases the risk of CKD. 24 Diabetes mellitus is a well-established risk factor for CKD. 25 Our study agrees with the literature and further highlights the importance of optimization of comorbid conditions, especially diabetes control for renoprotection. AKI is associated with a significant risk of CKD (HR: 1.91). 26 Also, postoperative AKI is associated with increased morbidity, mortality rate, and length-of-hospital stay following many types of major surgeries. 27 The incidence of AKI after open RC is 11%–33%. 28 Predictors of AKI were BMI, preoperative plasma creatinine, intraoperative blood loss, volume of administered crystalloids, fluid balance, and duration of surgery. 28 Optimization of the patient condition and adhering to the enhanced recovery after surgery principles may help reduce the incidence of AKI.
A previous work from our group reported a ureteroileal stricture rate after RARC of 13%. More than two-thirds of the strictures developed in asymptomatic patients, which may delay the diagnosis, management, and subsequently exacerbate renal injury. 29 Jin and colleagues have looked at the long-term deterioration of renal function after RC and they concluded that obstruction is the single most important cause of renal function deterioration despite the diversion type. 16 A propensity score-matched study looking at renal function deterioration between different types of diversion identified hydronephrosis, strictures, and stones as significant predictors. 14 Strictures, hydronephrosis, and recurrent UTI may correlate significantly, however, our nomogram has highlighted the importance of each of them. Implanting the ureters in a refluxing manner causes minimal pelvicaliceal system dilatation, which could be confused sometimes with strictures causing mild obstruction. The latter may be asymptomatic in 75%, but can cause gradual loss of renal function over time. 29 The presence of higher grade hydronephrosis indicates more severe obstruction due to stricture disease, and a superimposed infection can dramatically worsen the kidney functions. UTI occurs in up to 36% of patients after RC, especially with the presence of hydronephrosis and/or ureteroileal strictures, and chronic UTIs have been associated with deterioration of renal functions after RC. 16,30 This highlights the importance of regular follow-up for early detection and management of postoperative complications.
pN+ve may be attributed to stricture formation and hydronephrosis. pN+ve disease will require more aggressive lymph node and ureteral dissection, which may ultimately lead to more ureteroileal strictures. Patients with pN+ve disease may receive adjuvant chemotherapy, which is nephrotoxic. The contribution of adjuvant chemotherapy in this study may be underestimated, as we focused more on the preoperative, operative, and immediate 90-day postoperative variables associated with CKD. Adjuvant chemotherapy in many cases is delayed until patients fully recover from surgery and can tolerate chemotherapy.
NAC was not a predictor of CKD in our nomogram despite the known effect of chemotherapy on renal functions. This may be explained by patients with refractory nonmuscle invasive bladder cancer (45%) undergoing RARC. Also, the low utilization rate of NAC (27%) in our cohort. Both factors might affect the importance of NAC in our model.
Whether the type of urinary diversion affects renal functions after RC or not remains a matter of debate. Our model, as well as prior studies, has shown no difference between ileal conduits and neobladders. 14 However, other retrospective studies have shown opposite results. 16 Patients who receive ileal conduits tend to be older with multiple comorbidities at baseline, which may further worsen their kidney function. On the contrary, continent urinary reservoirs allow for more contact time between the urine and the intestine, which leads to increased absorption of electrolytes that can ultimately compromise renal function. 7
The importance of our nomogram is that it will aid in patient counseling about the future risk of developing CKD. Our nomogram also highlights the importance of preparing the patients medically and psychologically so that they are not blind to the outcome of their disease. Furthermore, getting a nephrologist early onboard adds diversity of thought to care. The choice of urinary diversion approach and follow-up protocols may be altered based on the patient's specific probability of CKD.
To our knowledge, this is the largest series investigating CKD-free survival after RARC and developing a nomogram. However, some limitations do exist. Although data were collected prospectively, our results are still subjected to the limitations and biases associated with retrospective analysis. This is a single-center study and external validation is required. All patients included had undergone RARC, and no ORC cases were included. Despite this, we do not believe that an open approach will pose a significant difference in prediction of renal function. The aforementioned variables rather than the technique are related to renal functions. Proteinuria was not captured for any of the patients, which may have a prognostic effect. Also, the hydration status at the time of creatinine withdrawal was not reported. A physiologic decrease in eGFR per year was not corrected for. The improvement of eGFR after the relief of obstruction was not captured. 16 External validation of the model is warranted before use in clinical practice.
Conclusion
We have developed and cross-validated a nomogram to estimate the CKD-free survival up to 5 years post-RARC, based on nine objective and easy to acquire variables.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.