
Abstract
Purpose:
To elucidate factors contributing to early urinary continence recovery after retzius-sparing robot-assisted radical prostatectomy (RS-RARP) by evaluating postoperative pelvic anatomical features between RS-RARP and conventional RARP (CON-RARP).
Materials and Methods:
We retrospectively examined 50 men who underwent RS-RARP (n = 25; the RS-RARP group) and CON-RARP (n = 25; the CON-RARP group) between October 2017 and June 2018. Perioperative outcomes and postoperative urinary continence were assessed in both groups. Anatomical features including the bladder neck-to-pubic symphysis ratio (determined from cystograms) and membranous urethral length (MUL) (determined from magnetic resonance imaging) were evaluated.
Result:
The daily urinary incontinence rate at discharge was significantly lower in the RS-RARP group than in the CON-RARP group (0.046 [range: 0.014–0.160] vs 0.357 [range: 0.139–0.616], p < 0.001). Postoperative urinary continence at 1, 3, 6, and 12 months was 80%, 92%, 96%, and 96% in the RS-RARP group and 24%, 40%, 68%, and 84% in the CON-RARP group, respectively (p < 0.001). The urgency scores in the international prostate symptom score (IPSS) questionnaire at 1 and 3 months were significantly lower in the RS-RARP than in the CON-RARP group (p = 0.028 and 0.033, respectively). The quality of life (QOL) indices were more significantly improved in the RS-RARP group than in the CON-RARP group 1 month (p = 0.027) and 3 months (p = 0.045) postoperatively. Receiver operating characteristic analysis revealed that a postoperative MUL of 12.1 mm (area under the curve: 0.852) was the optimal cutoff value predictive of continence recovery after 1 month. Multivariate analysis demonstrated that RS-RARP (odds ratio [OR]: 23.6; p < 0.001) and prostate volume (OR: 0.926; p = 0.049) were the independent factors of a longer MUL.
Conclusions:
RS-RARP results in an early continence recovery and a better urgency score in the IPSS by suppressing the descent of the bladder and maintaining a long MUL. RS-RARP may contribute to a better QOL recovery after RARP.
Introduction
Urinary incontinence is an associated robot-assisted radical prostatectomy (RARP) complication that decreases the patient's quality of life (QOL). 1 RARP has undergone various improvements for controlling incontinence; these include bladder neck preservation, restoration of the posterior aspect of the rhabdosphincter, and sparing of the pubovesical complex. 2 –4
In 2010, Bocciardi developed retzius-sparing RARP (RS-RARP), a novel technique that preserves the retzius cavity. 5 RS-RARP helps acquire early urinary continence by preserving the anatomical structures that are integral to maintaining potency and continence. 6,7 Anatomical parameters such as the bladder neck-to-pubic symphysis (BNPS) ratio and the membranous urethral length (MUL) measured from cystography are related to urinary continence recovery after RARP. 8 –10 However, no studies have investigated the postoperative anatomical features of patients undergoing RS-RARP using MRI, which allows a more accurate MUL measurement than cystography. We hypothesized that retzius preservation might contribute to a longer postoperative MUL and thus, an early continence recovery. Therefore, this study aimed to analyze the factors for early continence recovery following RARP and compare the associations between the early urinary symptoms recovery and the pelvic anatomical features between the RS-RARP and conventional RARP (CON-RARP).
Patients and Methods
Patients
This single-center, retrospective study was conducted with 50 consecutive patients undergoing RS-RARP (n = 25; RS-RARP group) and CON-RARP (n = 25; CON-RARP group) between October 2017 and June 2018. All surgeries were performed by the same surgeons (S.H. and A.O.) with over 100 experiences of CON-RARP. This study was approved by the Ethical Committee of the Nagoya City University (approval no. 60-19-0096). All patients provided written informed consent and completed a minimum follow-up of 12 months. Owing to our initial experience with the RS-RARP procedure at our institution, RS-RARP was adapted only for patients with low or intermediate-risk prostate cancer (PCa), whose clinical stage was T1c, T2a, or T2b. The tumors distributed widely near the apex and anterior region of the prostate were excluded.
Surgical procedures
Our RS-RARP technique is closely similar to those described previously. 11,12 Depending on the PCa localization, lateral dissection was performed in the intrafascial, interfascial, or extrafascial planes using Ligasure. We basically performed unilateral nerve-sparing surgery. Urethral anastomosis was performed using continuous sutures with two sets of absorbable barbed sutures (3-0 STRATAFIX®; Johnson & Johnson K.K, Tokyo, Japan). CON-RARP was performed as described previously. 13 Unilateral nerve-sparing surgery was performed in four cases. The Rocco stitch 3 and anterior suspension were performed in all cases.
Anatomical evaluations using cystogram and MRI
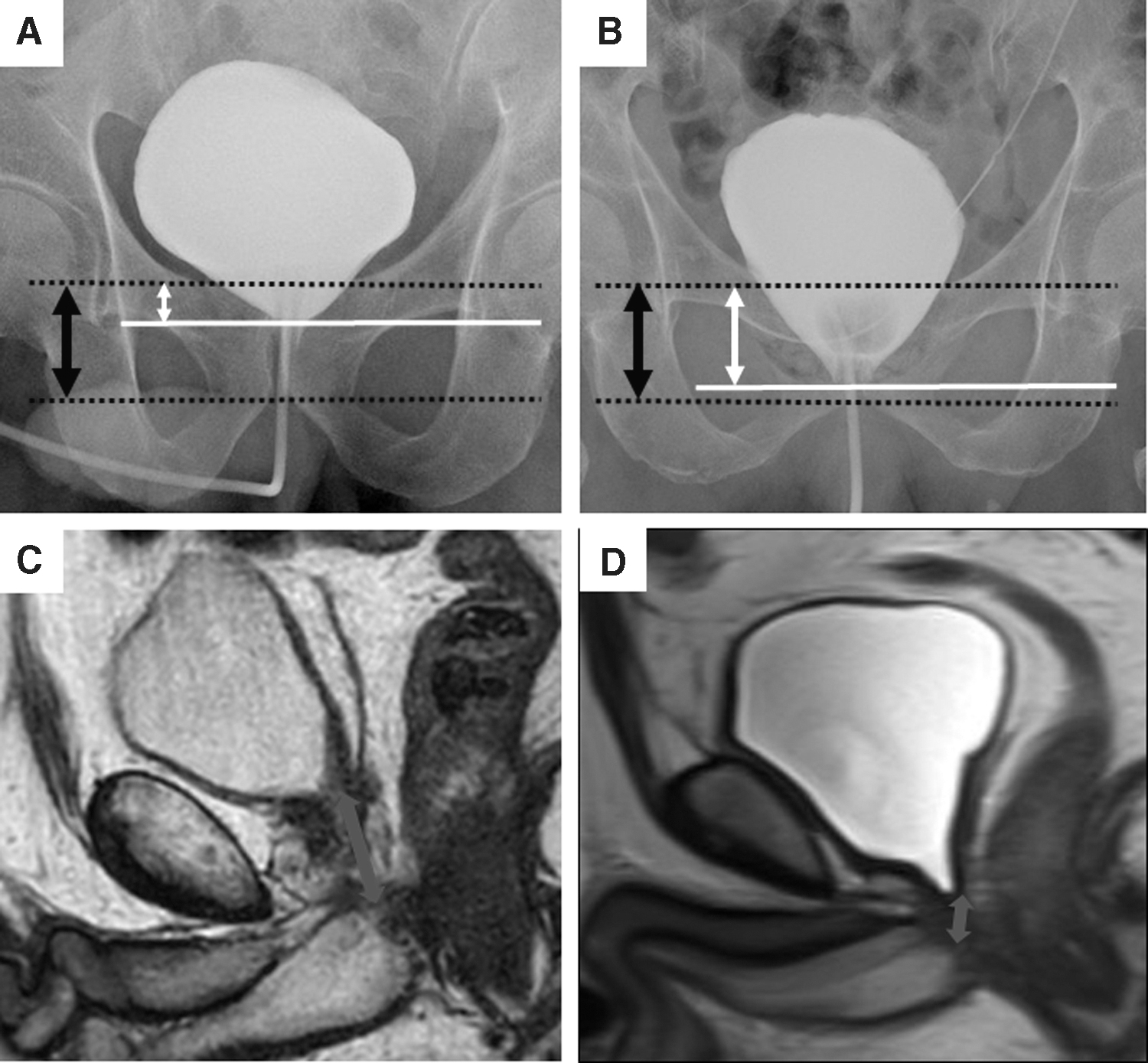
A cystogram was performed about 7 days after the surgery. As described by Olgin and colleagues, 8 the BNPS ratios were calculated from the cystograms by dividing the distance between the bladder neck and pubic symphysis by the total pubic symphysis height. Preoperative and postoperative MRI scans were performed for evaluating the pre- and postoperative pelvic oncological status and pelvic anatomical features for all patients. The patients agreed that this examination would be covered by their health insurance. The examination was performed between 3 and 6 months postoperatively. The MUL was computed as the distance from the bladder neck to the most proximal part of the bulbous urethra on the sagittal plane, as indicated in Figure 1.
Lower urinary tract symptom evaluation
The postoperative international prostate symptom score (IPSS) and QOL indices were evaluated 1, 3, and 6 months after the surgery.
The daily urinary incontinence rate was calculated as the amount of urine at discharge per day (incontinent volume to pads/total urine volume). Furthermore, the postoperative continence status was evaluated 1, 3, 6, and 12 months after the surgery. Recovery of continence was defined as wearing zero or one safety pad per day.
Statistical analysis
All statistical analyses were performed by two authors (Y.O. and S.H.) using EZR for R. 14 All data were analyzed using descriptive statistics and were presented as percentages. Continuous variables were presented as medians and interquartile ranges. The Mann–Whitney U-test was used for analyzing continuous variables, while the chi-square test was used for comparing categorical variables. The Spearman's rank correlation coefficient was used for measuring the correlation between early continence recovery and perioperative variables. Kaplan–Meier curves and the log-rank test were used to compare the recovery of urinary continence during the follow-up period. Multivariate analyses were performed using a logistic regression model. The MUL cutoff predicting early continence recovery at 1 month and its predictive accuracy were determined by receiver operating characteristic (ROC) curve analysis. A p-value <0.05 was considered as statistically significant.
Results
Patient characteristics
The preoperative prostate-specific antigen level was higher in the CON-RARP group because RS-RARP cases were mainly at intermediate or lower risk according to the D'amico classification 15 ; however, this difference was not significant (p = 0.070; Table 1).
Patients’ Characteristics
BMI = body mass index; CON-RARP = conventional robot-assisted radical prostatectomy; IPSS = international prostate symptom score; IQR = interquartile ranges; MUL = membranous urethral length; PSA = prostate-specific antigen; QOL = quality of life; RS-RARP = retzius-sparing robot-assisted radical prostatectomy.
Surgical outcomes
There were no significant differences in the surgical time, postoperative hospital stay, and Clavien-Dindo grades 16 of perioperative complications between the two groups. Postoperative inguinal hernia did not develop in the RS-RARP group, while 3 cases (12%) of postoperative inguinal hernia were reported in the CON-RARP group; significant differences were not observed (p = 0.074). The anastomosis time was significantly longer in the RS-RARP group than in the CON-RARP group (p = 0.003). Similarly, the estimated blood loss was significantly greater in the RS-RARP group than in the CON-RARP group (p = 0.020). However, no patient required blood transfusion. The positive surgical margin (PSM) ratio of the pT2 cases was higher in the RS-RARP group than in the CON-RARP group; however, this difference was not significant (p = 0.150; Table 2).
Surgical Outcomes
Pelvic anatomical outcomes
The BNPS ratio was 0.304 (range: 0.209–0.408) in the RS-RARP group and 0.501 (range: 0.421–0.593) in the CON-RARP group (p < 0.001; Table 3). This indicated that the bladder neck remains in its original position in the RS-RARP group. The MUL was 13.9 mm (range: 12.2–16.5 mm) in the RS-RARP group and 10.1 mm (range: 9.1–11.7 mm) in the CON-RARP group, indicating that it was significantly longer in the former (p < 0.001). MRI findings revealed that the bladder in the RS-RARP group retained its original location, while in the CON-RARP group, it dropped to the pelvic floor (Fig. 1).
Continence Outcomes and Pelvic Anatomical Features
Daily incontinence rate at discharge = urinary incontinence amount at discharge per day divided by the total urine volume.
Continence status was defined as wearing no pads or using one safety pad per day.
BNPS = bladder neck to pubic symphysis.
Functional outcomes of continence recovery and urinary symptom
The daily urinary incontinence rate at discharge was significantly lower in the RS-RARP group than in the CON-RARP group (0.046 [range: 0.014–0.160] vs 0.357 [range: 0.139–0.616]; p < 0.001) (Table 3). The urinary continence (wearing one safety pad per day or none) rates 1, 3, 6, and 12 months after surgery were 80%, 92%, 96%, and 96%, respectively, in the RS-RARP group and 24%, 40%, 68%, and 84%, respectively, in the CON-RARP group (log-rank; p < 0.001) (Fig. 2). Patients who underwent RS-RARP could acquire significant urinary continence within 6 months after the surgery.

Kaplan–Meier curves showing the recovery of urinary continence in patients undergoing RS-RARP and CON-RARP.
While the IPSS did not differ significantly between the two groups within 6 months after the surgery, the urgency scores at 1 and 3 months were significantly lower in the RS-RARP group than in the CON-RARP group (p = 0.028 and 0.033, respectively). The QOL indices at 1 and 3 months were significantly better in the RS-RARP group than in the CON-RARP group (1 month: 4.0 vs 5.5 [p = 0.027]; 3 months: 3.5 vs 4.5 [p = 0.045]). However, there were no significant intergroup differences in the QOL index 6 months after the surgery (Table 4).
Assessment of the International Prostate Symptom Score and the Quality of Life Index
Pre = preoperative; SD = standard deviation.
Associations between perioperative factors and continence recovery
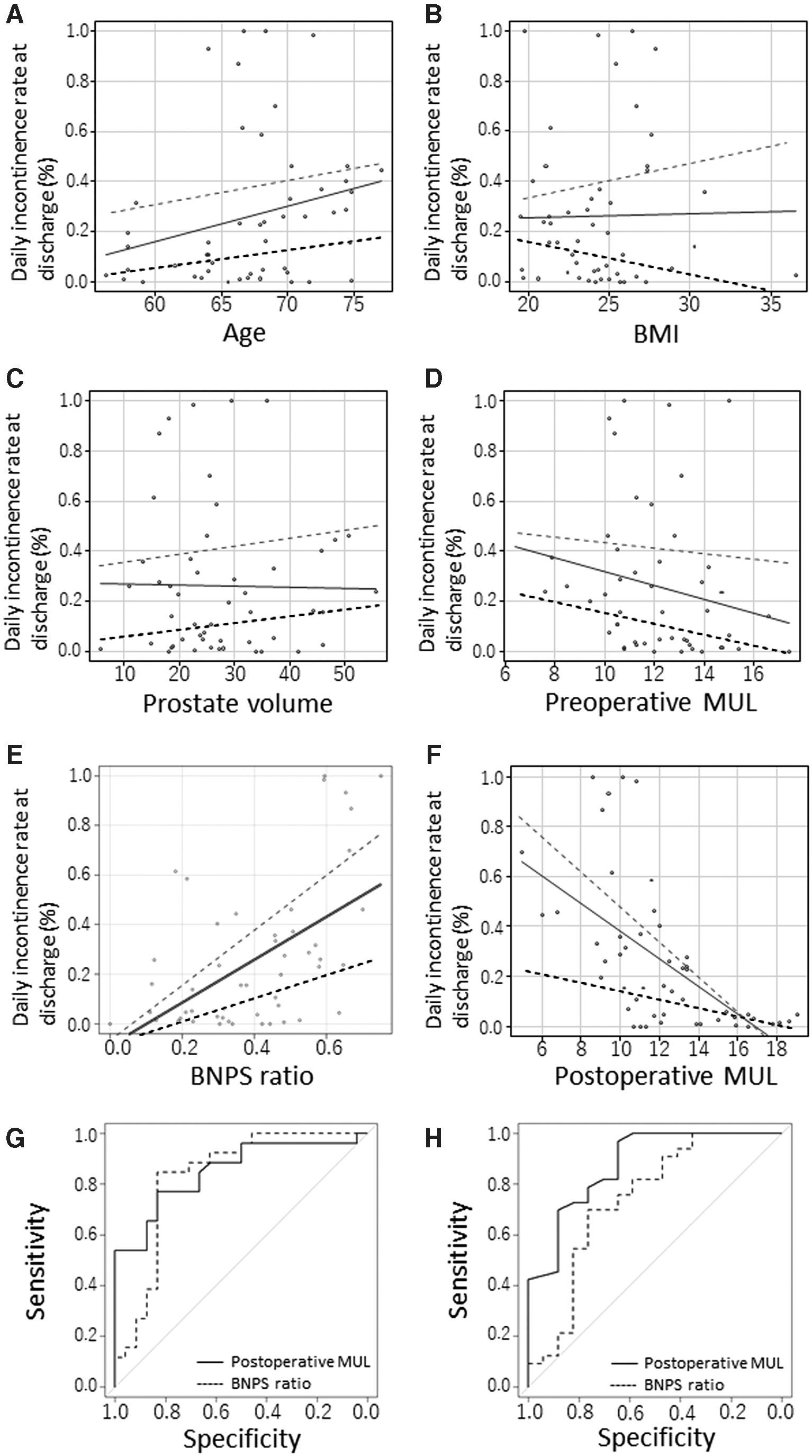
The correlation between urinary incontinence rate at discharge and the perioperative factors is shown in Figures 3A–F. In all cases, the age (r = 0.269; p = 0.059), BMI (r = 0.041; p = 0.779), and prostate volume (r = 0.035; p = 0.810) were not significantly associated with the daily incontinence rate at discharge. Conversely, the preoperative MUL (r = −0.293; p = 0.039), BNPS ratio (r = 0.489; p < 0.001), and postoperative MUL (r = −0.667; p < 0.001) were significantly associated with early postoperative continence recovery. In the RS-RARP group, the BMI (r = −0.456; p = 0.025), BNPS ratio (r = 0.429; p = 0.032), and postoperative MUL (r = −0.535; p = 0.006) were significantly associated with early continence recovery. In the CON-RARP group, the BNPS ratio (r = 0.503; p = 0.014) and postoperative MUL (r = −0.517; p = 0.011) were significantly associated with early continence recovery.
Multivariate analysis revealed that RS-RARP was an independent factor associated with postoperative continence recovery after 1 month (odds ratio [OR]: 12.7; p < 0.001) and 3 months (OR: 15.50; p = 0.003). Furthermore, a longer preoperative MUL had a significantly positive impact on continence recovery after 3 months. After 6 months from the surgery, RS-RARP and preoperative MUL positively impacted continence recovery; however, these impacts were not significant. Conversely, a higher BMI had a significantly negative impact on urinary continence 12 months after the surgery (OR: 0.665; p = 0.02; Table 5).
Multivariate Logistic Regression Analysis for Risk Factors Associated with Postoperative Continence
CI = confidence interval; OR, odds ratio.
ROC curve analysis revealed that a postoperative MUL of 12.1 mm and a BNPS ratio of 0.421 with an area under the curve (AUC) of 0.852 (95% confidence interval [CI]: 0.745–0.959) and 0.832 (95% CI: 0707–0.956), respectively, were the optimal cutoff values predictive of continence recovery at 1 month; there were no significant differences in the predictive accuracy between the two groups (p = 0.808; Fig. 3G). A postoperative MUL of 10.1 mm and a BNPS ratio of 0.443 with an AUC of 0.878 (95% CI: 0.774–0.981) and 0.742 (95% CI: 0.578–0.905), respectively, were the optimal cutoff values predictive of continence recovery at 3 months. Though the postoperative MUL had a higher predictive accuracy than the BNPS ratio, this difference was not significant (p = 0.164; Fig. 3H). Multivariate analysis also revealed that RS-RARP (OR: 23.6; p < 0.001) and prostate volume (OR: 0.926; p = 0.049) were the independent predictors for a longer MUL (≧12.1 mm; Table 6).
Multivariate Logistic Regression Analysis for Factors Associated with a Long Membranous Urethral Length (≧12.1 mm)
Discussion
Immediately after introducing the RS-RARP technique, we succeeded in achieving early continence recovery compared with the conventional approach; suppressing the descent of the bladder and maintaining a long MUL may contribute to this recovery. Urinary incontinence is often a problem within 3 months after RARP. 17,18 According to Dalela, 71% of the men who underwent RS-RARP were continent within 1 week after catheter removal. 12 In this study, the daily urinary incontinence rate at discharge was measured to evaluate early continence recovery; at 4.6%, the RS-RARP group had a better rate than the 35.7% of the CON-RARP group. Furthermore, we obtained satisfactory continence recovery rates of 80% and 92%, 1 and 3 months after the surgery, respectively. Furthermore, though we included the initial 25 consecutive RS-RARP cases, our data were not inferior to that of a previous study by Menon and colleagues, which observed that 83% and 95% of the men who underwent RS-RARP used one or no pads in the first and third month after the surgery, respectively. 12,19
Conversely, the incidence of PSM in the pT2 cases of the RS-RARP group was 29.2% and higher than that of the pT2 cases of the CON-RARP group. Regarding the learning curve of RS-RARP, Galfano and colleagues reported that the PSM incidence in the initial 100 cases was 32%, while in the next 100 patients, it was 19%. 11 Therefore, there is room for improvement in our technique. Surgical margin status is a known predictor of biochemical recurrence and PCa-specific mortality 20,21 ; therefore, indications for RS-RARP need to be discussed carefully.
To our knowledge, only few reports have evaluated RS-RARP patients using the IPSS and QOL index questionnaires. 12,22 Furthermore, our report is the first to focus on each score in the IPSS questionnaire in RS-RARP patients. This study indicated that the QOL indices in the RS-RARP group were significantly better than in the CON-RARP group within 3 months after the surgery. Among all IPSSs, only the urgency scores, 1 and 3 months postoperatively, underwent a greater significant decrease in the RS-RARP group than in the CON-RARP group. The improved QOL index in the RS-RARP group within 3 months may be attributed to the early recovery of continent and urgency symptoms.
Several factors contribute to early continence recovery after RARP. Among biological and preoperative factors, an older age, higher BMI, larger prostate volume, shorter preoperative MUL, and severe IPSS were reported to negatively impact early continence recovery. 7,23,24 In this study, age tended to be associated with the daily incontinence rate at discharge; however, there were no significant differences. The small sample size and presence of younger patients in the RS-RARP group may limit the evaluation of the association between the surgical method and continence recovery. With respect to the BMI, CON-RARP had a negative impact; however, RS-RARP had a positive impact on early continence recovery, leading to no negative impact in all cases. We do not know the precise reasons, but the BMI may not affect the incontinence after RS-RARP.
A meta-analysis reported that a longer preoperative MUL greatly correlated to an early overall postoperative urinary continence recovery. 25 In this study, the preoperative MUL, BNPS ratio, and postoperative MUL were significantly associated with early postoperative continence recovery. Furthermore, preoperative MUL tended to positively impact the overall continence recovery, with a significantly positive effect observed 3 months after the surgery. Conversely, RS-RARP was the most positive prognostic factor of continence recovery at discharge and 1 and 3 months after the surgery. The choice of surgical methods (RS- or CON-RARP) might only influence early continence recovery within 3 months.
The BNPS ratio 8,10,26 and postoperative MUL 9,27 were also reported to be the predictors of early continence recovery. Olgin and colleagues stated that 3 months after the surgery, continent and incontinent patients had mean BNPS ratios of 0.39 and 0.49, respectively. 8 In our study, the median BNPS ratio in patients who experienced RS-RARP was 0.304, which appears lower than the ratios reported previously. 28 Haga and colleagues showed that a postoperative MUL >17 mm, as measured on a postoperative cystogram, may be a predictor of early urinary continence recovery after CON-RARP. 9 In this study, the postoperative MUL, measured using MRI, had a higher predictive accuracy than the BNPS ratio for continence recovery at 3 months postoperatively. Multivariate analysis also revealed that RS-RARP and prostate volume were the independent factors for a longer MUL (≧12.1 mm). RS-RARP preserves the retzius space, which suppresses the descent of the bladder. This may lead to a longer MUL and promotion of postoperative continence recovery.
This study had certain methodological limitations. First, owing to its retrospective design, the small sample size may limit the evaluation of the association between the surgical method and continence recovery. Second, we did not evaluate the effect of the nerves-paring step on the postoperative continence because we had not actively intended to perform nerve-sparing surgery. Third, this was a single-institution study. Finally, the PSM in the RS-RARP cases was not favorable; this may be because our cases included the initial consecutive patients in our institution. However, regarding continence recovery, our data are as relevant as that of previous reports.
Conclusions
RS-RARP resulted in an early continence recovery and a better urgency score in the IPSS questionnaire by suppressing the descent of the bladder and maintaining a long MUL. RS-RARP may contribute to a better QOL recovery, despite its gentle learning curve in cancer control.
Footnotes
Acknowledgments
We would like to thank Ms. M. Noda for secretarial assistance. The authors would like to thank Editage for the English language review.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.