
Abstract

W
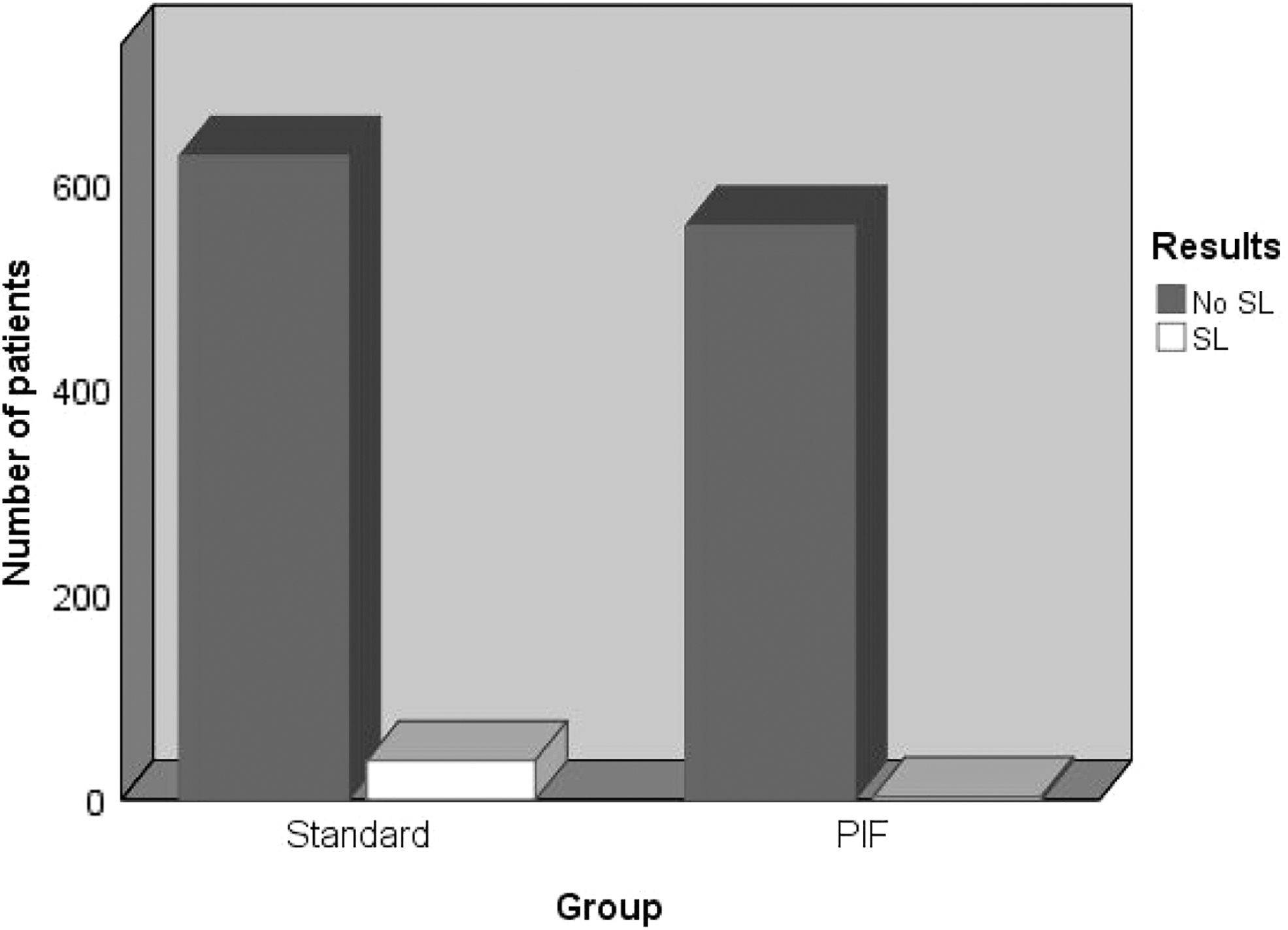
Now Lee and colleagues confirmed the positive effect of peritoneal interposition flap (PIF) first reported by Lebeis et al. Although the initial study on PIF reports reduction of SL rates from 11.6% in the standard to 0% in the intervention group, the most recent validation study reports reduction from 6% to 0%. 1,3 This is in line with results of PIF modifications studied by Stolzenburg and colleagues(four-point peritoneal flap fixation; 4.6% and 1%, respectively) and Dal Moro et al. (P.L.E.A.T.; 4.1% and 0.6%, respectively). 4,5 Thus, these four retrospective studies suggest a decisive impact of PIF on SL rates. 1,3 –5 By summarizing these four studies (1229 patients), 666 patients underwent standard treatment and 563 (45.8%) received PIF. The combined SL rates were aggregated 5.7% (n = 38) and 0.5% (n = 3), respectively (p < 0.001; Fig. 1). 1,3 –5 The result of the univariate analysis shows a risk reduction by 91% with PIF (OR: 0.089; 95% CI: 0.027–0.288, p < 0.001). Thus, PIF is the “hottest promise” beneath all procedures in reducing SLs in RARP with PLND. But it needs to be stated that these promising results have been derived from retrospective studies comparing PIF with “historical” controls. 1,3 –5 Retrospective studies generate hypotheses. Proof and establishing of PIF need randomized clinical trials (RCTs) with direct evidence.
We recently published such an RCT. 7 In this multicenter study, 232 patients were included between March and December 2017 and randomized to standard and PIF according to its first description by Lebeis and colleagues 3 Patients and medical staff providing postinterventional care and follow-up were blinded. All patient and cancer characteristics did not differ between the groups, a median of 16 lymph nodes were dissected (IQR 11–21). SLs occurred after 3 months postoperatively in 9.1% of the cases and did not differ between both groups (9.7% vs 8.3%, p = 0.820). There were no differences in the functional outcomes between the groups and no signs for increased perioperative morbidity in the PIF group. 7
Our RCT thus contradicts the results of Lee et al., and evidence of further RCTs is needed to judge the true value of PIF in the prevention of SLs.