
Abstract
Objectives:
To determine the safety and efficacy of flexible ureteroscopy in the treatment of transplant urolithiasis.
Materials and Methods:
We reviewed a single-center series of 2652 patients who underwent surgical treatment for nephrolithiasis at our institution from 2009 to the present day to identify all patients undergoing ureteroscopy for treatment of transplant lithiasis.
Results:
We identified 18 patients who underwent ureteroscopy for treatment of urolithiasis within the transplanted kidney or ureter. The majority of the procedures were performed using a retrograde approach with flexible ureteroscopy, with one patient undergoing antegrade ureteroscopy and two patients requiring semirigid ureteroscopy. Holmium:yttrium-aluminum-garnet laser lithotripsy was utilized in all but one case, which was performed using basket extraction. There were no intraoperative complications reported. Four patients had small stone fragments on postoperative imaging, three of which were observed. One patient required repeat ureteroscopy for persistent distal ureteral stone.
Conclusion:
Retrograde ureteroscopy is a feasible, safe, and effective intervention for the treatment of transplant lithiasis. Minimal intraoperative or postoperative complications were reported, and only one patient required additional intervention for residual stone burden.
Introduction
Although rare in renal transplant patients compared to the general population, obstructive urolithiasis poses significant risk to renal graft function given the presence of a solitary renal unit in this patient population. 1 –3 In addition, while patients from the general population with obstructing ureteral stones often present with a constellation of well-described clinical symptoms, including flank pain, urinary tract infection, and renal failure, the lack of renal and ureteral innervation after transplantation may lead to a delay in diagnosis due to the absence of flank pain and the immunosuppressed status of these patients places them at a higher risk of developing sepsis. 4 However, once the diagnosis of urolithiasis in a renal transplant patient is made, the subsequent management of this patient population and the long-term results are not as well described.
The current urolithiasis guidelines do not recommend a specific treatment strategy in kidney transplant recipients and options include an endourologic approach, extracorporeal shockwave lithotripsy (SWL), percutaneous nephrolithotomy (PCNL), and open surgical extraction. 5,6 For kidney transplant patients with a stone burden >1.5 cm, PCNL has been shown to be a safe and effective treatment modality. 7 –9 In the past, SWL has been favored over ureteroscopy for the treatment of urolithiasis <1.5 cm in kidney transplant patients given the perceived technical difficulties of retrograde endoscopic surgery. 10 –12 However, the continued advancement in endoscopic technology has made ureteroscopy more feasible. 13 –15 Toward this end, we report our experience with ureteroscopy for the treatment of urolithiasis in the transplant kidney and ureter.
Materials and Methods
We retrospectively reviewed the records of patients with urolithiasis from a single-center series of 2652 patients who underwent surgical treatment for nephrolithiasis at our institution from January 2009 through January 2018 to identify all patients requiring ureteroscopy for the treatment of transplant lithiasis. Patient demographics (Table 1), presenting symptoms, stone size and location, surgical technique, perioperative complications, and postoperative follow-up, including stone-free rate and intervention-free survival, were evaluated.
Patient Demographics and Stone Characteristics
F = female; M = male; URS = ureteroscopy.
Renal transplants were performed with the kidney transplanted into the right or the left iliac fossa. The majority of ureteral anastomoses (15 of the 18 patients) were created using the Lich-Gregoir technique. Of the remaining three patients, one patient had a ureteroureterostomy, one patient had a cutaneous ureterostomy, and one patient who underwent renal transplantation as a pediatric patient had the ureteral anastomosis created using the Politano-Leadbetter technique.
All ureteroscopic procedures were performed using a retrograde approach. In two cases, previously obtained antegrade access was used to aid in identification of the ureteral orifice (Fig. 1). Holmium:yttrium-aluminum-garnet laser lithotripsy was utilized in all but one case, which was performed using basket extraction. Flexible ureteroscopy was utilized in 16 patients of the 18 patients, while semirigid ureteroscopy was performed in 2 of the 18 patients. The average operative time was 76.44 minutes.
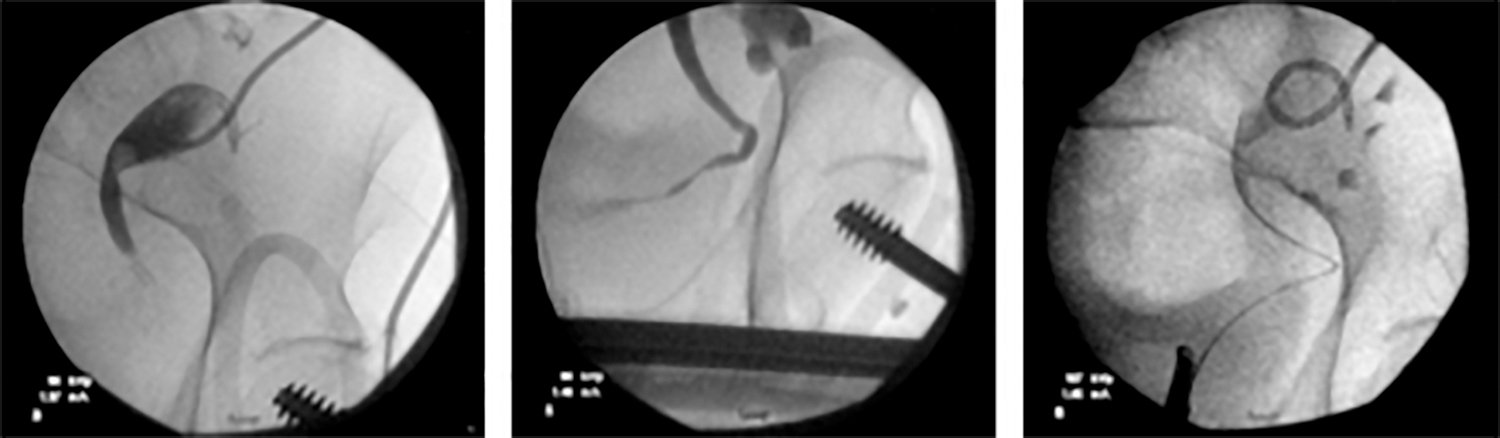
Fluoroscopic images illustrating the use of an antegrade nephrostogram to identify the ureteral orifice and allow for retrograde cannulation of the transplant ureteral orifice.
The procedure was started using rigid cystoscopy to advance a sensor wire into the transplant ureteral orifice. In two cases, the flexible cystoscope was utilized to provide better visualization of the ureteral orifice located at the dome of the bladder. If difficulty was encountered while placing the sensor wire at the ureteral orifice or advancing the wire past the ureteral stone, an angled glide wire was then used. Retrograde access was obtained in 16 of the 18 patients (89%) without the use of previously placed antegrade access. In 11% (n = 2) of patients, antegrade access was utilized. In one patient, difficulty was encountered (Boston Scientific, Marborough, MA) when attempting to identify the transplant ureteral orifice and an antegrade nephrostogram was performed. The identification of the location of the ureteral orifice on fluoroscopy, as well as the direct visualization of contrast effluxing from the ureteral orifice, allowed for optimization of the positioning of the cystoscope and thus aided in retrograde cannulation of the ureteral orifice using a sensor wire (Fig. 1). In another patient, a wire was placed antegrade before any attempts at retrograde access given the presence of a ureteroureterostomy. In both of these patients, antegrade access had been obtained preoperatively via placement of a nephrostomy tube for the presence of infected, obstructing ureteral stones. A 12/14F access sheath, with a length of either 28 or 35 cm, was used in 7 of the 18 patients (39%). A Double-J 6F ureteral stent was left in place in 16 of the 18 patients (89%). This study was approved by Internal Review Board (IRB no. 2014-0033).
Results
We identified 18 patients who underwent ureteroscopy for treatment of urolithiasis within the transplanted kidney or ureter over a 9 years period. The average age at presentation was 53.5 years old. Fifty-six percent of patients were female and 44% were male (Table 1). All patients had cross sectional imaging before intervention.
The total stone burden ranged from 3 to 14 mm (Table 1), with an average stone burden of ∼8.6 mm. Sixty-seven percent of patients had obstructing stones located within the ureter, while 33% of patients had stones located only within the kidney. The most common presenting symptom was infection, with 7 of the 18 patients (39%) presenting with either pyelonephritis or urinary tract infection. Of these seven patients presenting with both infection and obstructing ureteral stones, six underwent nephrostomy tube placement and one underwent transplant ureteral stent placement for emergent drainage before stone treatment. Other presenting symptoms included incidental finding on routine imaging (28%), hematuria (22%), acute kidney injury (5.6%), and pain (5.6%).
There were no intraoperative complications (Table 2). Flexible ureteroscopy was utilized in 16 patients of the 18 patients, while semirigid ureteroscopy was performed in 2 of the 18 patients. Of the two patients who underwent semirigid ureteroscopy, one had a transplant ureteral anastomosis created using the Lich-Gregoir technique and the other patient had a transplant ureteral anastomosis created using the Politano-Leadbetter technique. In both cases requiring semirigid ureteroscopy, it was utilized due to difficulty maintaining the flexible ureteroscope within the ureter due to the distal location of the stone near the ureteral orifice. In the six patients who had a nephrostomy tube placed preoperatively, four of the six patients had the nephrostomy tube removed intraoperatively or on postoperative day 1. In the remaining two patients, the nephrostomy tube was left capped for 1 week, at which point repeat imaging was obtained to confirm no residual stone burden and the nephrostomy tubes were subsequently removed.
Outcomes Based on Stone Location
There were two postoperative complications. One patient developed a urine leak from a nephrostomy tube tract after the nephrostomy tube was removed intraoperatively, requiring percutaneous drainage and replacement of the nephrostomy tube. One patient who presented with an impacted distal ureteral stone was found to have retained stone fragments due to distal ureteral stricture, requiring repeat ureteroscopy and ultimately ureteroneocystotomy (Table 2).
Following stone treatment, 11 (61%) of patients were stone free on imaging, 5 (28%) had small residual stone burden, and two patients had no postoperative imaging performed. Postoperative imaging consisted of ultrasound in nine patients, CT scan in three patients, abdominal X-ray in three patients, and both ultrasound and abdominal X-ray in one patient. Of the patients with residual stone burden, four patients were observed without subsequent stone events and one patient, as mentioned previously, required repeat ureteroscopy for persistent ureteral stones due to ureteral stricture preventing passage of the stone fragments. One patient who did not undergo postoperative imaging and was lost to follow-up ultimately moved out of state and underwent ureteroscopy for a small nonobstructing renal stone at an outside institution greater than 1 year after initial ureteroscopy.
Stone analysis was performed in five patients, with two stones composed of primarily calcium oxalate monohydrate, one stone composed of primary calcium phosphate carbonate, one composed of calcium oxalate monohydrate, calcium oxalate dihydrate and calcium phosphate carbonate, and one composed of organic material, magnesium ammonium phosphate, calcium oxalate monohydrate, and calcium phosphate carbonate.
Of the seven patients who presented with infection, all but one patient had resolution of their presenting infection at 1–2 months follow-up. One patient, diagnosed preoperatively with recurrent urinary tract infections, continued to experience recurrent urinary tract infections despite stone treatment.
There was no significant decrease in estimated glomerular filtration rate at 1 month or 1 year postoperatively. At most recent follow-up (12–138 months postoperatively) all renal transplants remained functional aside from one patient diagnosed with hepatorenal syndrome unrelated to their history of urolithiasis.
Discussion
Although the presence of urolithiasis is rare among transplant patients, with most series reporting an incidence of <1%, 1 –3 this disease can pose significant risk to renal graft function as well as sepsis in the setting of acute obstruction. The subsequent management of these stones may pose a challenge to the urologist, both due to the increased medical complexity of these patients as well as the anatomic location of the transplanted kidney and ureter. As in the general population, there are multiple management options available, including watchful waiting, SWL, flexible ureteroscopy or PCNL.
Watchful waiting has been utilized in the literature for stones <4–6 mm with no reported loss of allograft function or renal failure. 2,11,16 However, this method does require stringent clinical, radiologic, and laboratory follow-up as the majority of these patients are functioning with a solitary kidney, and unrecognized obstruction could lead to acute kidney injury in the short term and, if unrecognized over time, allograft failure. Given this need for stringent follow-up and the risk of damage to the renal transplant due to unrecognized obstruction, watchful waiting is not a management option commonly used at our institution.
Percutaneous treatment of calculi located within the transplant kidney was first described in 1985 by Hulbert et al. 17 Today, PCNL is typically performed for stones >1.5 cm and has proven to be safe and effective for patients with large stone burden. 7 –9 As such, at our institution, PCNL is performed in patients presenting with stone burden greater than 1.5 cm, and ureteroscopy is reserved for patients with a stone burden less than 1.5 cm. Additional refinements in technique have been described, including minimally invasive PCNL, which utilizes a smaller tract to decrease the risk of bleeding and tearing of the renal cortex. 18 An additional option for antegrade management of urolithiasis includes antegrade ureteroscopy without dilation, particularly in patients with a nephrostomy tube placed before ureteroscopy.
In the past, there has been a trend toward the use extracorporeal shockwave therapy for the treatment of both ureteral and renal stones with stone burden less than 1.5 cm to avoid the perceived difficulties of accessing the transplanted kidney system via a retrograde approach. 10 –12 However, there are limitations associated with SWL. There may be difficulty locating the stones within the kidney or ureter fluoroscopically given the location of the transplanted kidney over the pelvis, which may also lead to shockwave attenuation and decreased efficacy. Based on the location of the stone, patients may have to be placed in the prone position during the procedure, which is associated with a variety of complications. 19 Patients may require multiple sessions of SWL or additional procedures if residual fragments or steinstrasse are present. In addition, they require stringent follow-up as passing fragments may lead to obstruction of the ureter. In a retrospective review performed by Challacombe and colleagues, 13 patients underwent SWL with 8 patients requiring multiple sessions and 2 patients requiring ureteroscopy after failure of SWL. 10 Yuan and coworkers identified five patients who underwent SWL, with four requiring multiple sessions and one requiring flexible ureteroscopy for retained stone fragments. 9 There is also the possibility of parenchymal injury or subcapsular hematoma with SWL, putting the allograft function at risk.
We report the largest single-center experience of the use of ureteroscopy for the treatment of transplant lithiasis. Previously, Del Pizzo et al. reported the feasibility of ureteroscopic intervention in renal allograft ureters, including four patients with obstructive ureteral calculii. 20 Verrier and colleagues reported their experience performing ureteroscopy on five patients with ureteral stones with a 60% stone-free rate. 2 However, two patients ultimately required open intervention with ureteral resection and ureteroureteral anastomosis after failure of endourologic techniques. Hyams and colleagues reported their experience with 12 patients treated exclusively with ureteroscopic intervention, 7 via a retrograde approach, and 5 via an antegrade approach, with 11 of 12 patients stone free on postoperative imaging. 13 Branchereau and coworkers performed a retrospective review of 95 patients with transplant lithiasis from 11 renal transplantation centers across Europe. 16 Ureteroscopy was performed in 26% of patients with stone measure 6–24 mm in diameter with no graft loss or deaths observed at a mean follow-up of 72 months. Surgical techniques, stone-free rates, complications, and need for additional intervention were not reported. Most recently, Sarier et al. reported the use of minimally invasive surgical treatment of allograft lithiasis in 22 patients, including cystolitholapaxy, flexible and semirigid ureteroscopy, and PCNL, with no major postoperative complications and a stone-free rate of 89%. 15
There are some limitations to our study. Stone analysis data were only reported in 5 out of 18 patients. In addition, follow-up imaging mainly comprised plain film and renal ultrasound, with a limited number of patients undergoing CT scan postoperatively to evaluate stone-free status.
In our experience, retrograde access to the transplanted ureter and kidney was attained without the need for antegrade access in 89% of cases with no intraoperative complications reported. In addition, 16 of 18 patients in our series required only one procedure for treatment of their urolithiasis with an 89% intervention-free survival. One patient required repeat ureteroscopy due to distal ureteral stricture limiting the passage of stone fragments and one patient underwent ureteroscopy for a small nonobstructing renal stone at an outside institution greater than 1 year after initial ureteroscopy.
Conclusions
While ureteroscopic intervention has not been favored over SWL in the past given the perceived technical difficulties associated with retrograde access in the kidney transplant population, we contend that retrograde ureteroscopy is a feasible, safe, and effective intervention for the treatment of transplant lithiasis. Minimal intraoperative or postoperative complications were reported and the majority of patients remained intervention free following stone treatment, making endourology the new gold standard for the management of transplant urolithiasis <1.5 cm.
Footnotes
Author Disclosure Statement
S.Y.N. is a consultant for Boston Scientific. The remaining authors have no competing financial interests to disclose.
Funding Information
No funding was received.