
Abstract
Objective:
We evaluated the influence of percutaneous nephrolithotomy (PCNL) on the estimated glomerular filtration rate (eGFR) in patients with chronic kidney disease (CKD).
Materials and Methods:
Between September 2007 and April 2019, 280 patients with a preoperative eGFR level <90 mL/min/1.73 m2 and who underwent PCNL were retrospectively examined. The primary endpoint of this study was the effect of PCNL on eGFR levels in the 1st and 12th month after surgery in patients with CKD according to CKD stages. The secondary endpoint of this study was the identification of potential risk factors for deteriorated eGFRs.
Results:
The mean eGFR of patients was 48.7 ± 17 mL/min/1.73 m2 in the preoperative period, 54.7 ± 21 mL/min/1.73 m2 in the postoperative 1st month, and 59.1 ± 23.2 mL/min/1.73 m2 in the postoperative 12th month. It was determined that the increases in eGFRs in the postoperative 1st and 12th months were significant in all CKD stages (p < 0.005). Compared with preoperative values, the eGFR value was reduced in 61 (21.8%) patients in the 1st month and 49 (17.5%) patients in the 12th month. When these patients were compared with those in the stable eGFR and recovery group, multiaccess PCNL was an independent risk factor for renal function deterioration at the postoperative 1st and 12th month on multivariate analysis (odds ratios were 6.94 and 9.46, respectively).
Conclusion:
PCNL was found to have a positive effect on short- and long-term eGFRs in patients with CKD. However, multiaccess PCNL may have adversely affected eGFRs in both the short and long term.
Introduction
Kidney stone disease is observed in 1.7% to 18% of patients with chronic kidney disease (CKD) and in 3.2% of those who require hemodialysis. 1 The treatment for kidney stones varies according to the size and localization of stones, using many different methods, including shockwave lithotripsy, retrograde intrarenal surgery, percutaneous nephrolithotomy (PCNL), and laparoscopic/open stone removal. PCNL is the gold standard operative treatment for kidney stones 2 cm or greater. 2 In patients with CKD and kidney stones, the most important determinant in choosing an appropriate treatment is the effect of the operative intervention on renal function. Percutaneous intervention seems to be the most appropriate treatment option with minimal morbidity and mortality rates. 3 A significant increase in the estimated glomerular filtration rate (eGFR) after PCNL has been reported in patients with CKD (especially those with end-stage kidney disease). 3 –5 However, in another study, the authors reported that kidney deterioration was seen after kidney treatment and this was associated with a higher baseline preoperative serum creatinine level, proteinuria >300 mg/day on follow-up, renal cortical atrophy, stone burden >1500 mm2, recurrent urinary infection, and age <15 years. 6 However, there are only a limited number of long-term follow-up case studies of CKD patients after PCNL.
This study aimed to evaluate the short- and long-term changes in patients (across varying levels of kidney function) who underwent PCNL due to kidney stones.
Materials and Methods
Data from 2660 patients who underwent PCNL in our clinic between September 2007 and April 2019 were retrospectively evaluated, and 280 patients with preoperative eGFR levels <90 mL/min/1.73 m2 were included in the study. All steps of the study were planned and conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent on admittance to the hospital was obtained from all individuals who permitted the use of respective medical information in clinical studies. Ethics committee approval of the study was obtained from the ethics committee of the University of Cukurova (approval number–April 5, 2019; 87/53).
Before the procedure, the medical history of the patients was obtained and physical examination, urinalysis, urine culture, complete blood count, serum biochemistry, coagulation tests, and plain urinary radiography or ultrasonography were performed. All patients underwent noncontrast CT preoperatively to assess the anatomy of the kidney and the localization and size of the stone in terms of percutaneous access. Patients with an eGFR value of >90 mL/min/1.73 m2, those who underwent a secondary PCNL procedure, children (under 16 years of age), and with incomplete data were excluded from the study. Patients with a urinary tract infection were treated with appropriate antibiotics before the operation. In patients with renal obstruction, a percutaneous nephrostomy tube (single or multiple) or Double-J stents were placed before surgery, and PCNL was performed after the patient's serum creatinine level was stabilized. PCNL was performed as a standard by inserting the retrograde ureter catheter into the prone position and performing 24F to 26F dilatation.
The eGFR was calculated according to the CKD epidemiology with a formula based on the serum creatinine level of patients. We considered >20% increase in the eGFR as improvement, >20% decrease as deterioration, and changes within 20% as stationary renal function.
The primary endpoint of this study was that PCNL improved eGFR levels in the 1st and 12th month after surgery in patients with CKD according to CKD stages. The patients were divided into the following three groups according to CKD stage;
eGFR = 60 to 90 mL/min/1.73 m2, stage II CKD,
eGFR = 30 to 59 mL/min/1.73 m2, stage III CKD, and
eGFR <30 mL/min/1.73 m2, stage IV/V CKD.
The secondary endpoint of this study was the identification of potential risk factors for deteriorated eGFRs. According to eGFR levels in the 1st and 12th months, patients were divided into two groups: deteriorated and nondeteriorated (the stable eGFR or recovery). Age, body mass index, stone burden, number of access tracts, operative time, stone-free rate, fever, and blood transfusion were evaluated and compared between deteriorated and nondeteriorated (the stable eGFR or recovery) groups.
The stone size was based on the digitized surface area and was calculated as the sum of products with a maximum stone size on CT. The presence of residual stones was evaluated with a postoperative nephrostogram or abdominal ultrasonography. In cases of suspicious findings, noncontrast CT was performed. Fragments >3 mm were considered to be significant residue.
Statistical analyses
SPSS® program, version 20.0, was used for statistical analysis. The rate of vital variables was obtained for descriptive statistics. For quantitative variables, median (minimum–maximum) values were calculated for nonparametric test results and mean ± standard deviation values were calculated for parametric test results. Preoperative, intraoperative, and postoperative factors that may affect renal function were tested using univariate analyses (chi-square or independent sample t-test). Multivariate (logistic regression) analysis was used to identify risk factors for deterioration of renal function in short- and long-term follow-up using factors (stone burden and access) that yield significant results in univariate analyses. Statistical significance was accepted at p < 0.05.
Results
The mean age of 280 patients who underwent PCNL was 51.98 ± 15.94 years: 212 (75.7%) were men and 68 (24.2%) were women. When the distribution of cases was evaluated according to CKD stages, there were 82 (29.3%) patients in stage II, 151 (53.9%) in stage III, and 47 (16.8%) in stage IV/V. The preoperative eGFR level was calculated within 24 hours before surgery. The mean eGFR of patients was 48.7 ± 17 mL/min/1.73 m2 in the preoperative period, 54.7 ± 21 mL/min/1.73 m2 at the postoperative 1st month, and 59.1 ± 23.2 mL/min/1.73 m2 at the postoperative 12th month. There was an increase in the eGFR in CKD stages compared with the eGFR in the preoperative period. When the CKD stages were evaluated individually, it was determined that increases in eGFRs in the postoperative 1st and 12th months were significant (p = 0.01) and the clearance of kidney stones with PCNL had a positive effect on renal function (Table 1). According to the results obtained for the postoperative 12th month compared with preoperative values, the number of patients was reduced from 47 (16.8%) to 24 (8.6%) in the stage IV/V group and from 151 (53.9%) to 123 (43.9%) in the stage III group (p < 0.001); in the stage II group, there was an increase in the number of patients from 82 (29.3%) to 103 (36.8%) (p < 0.001) and the eGFR value of 30 (10.7%) patients increased to over 90 mL/min/1.73 m2 (Figs. 1 and 2).
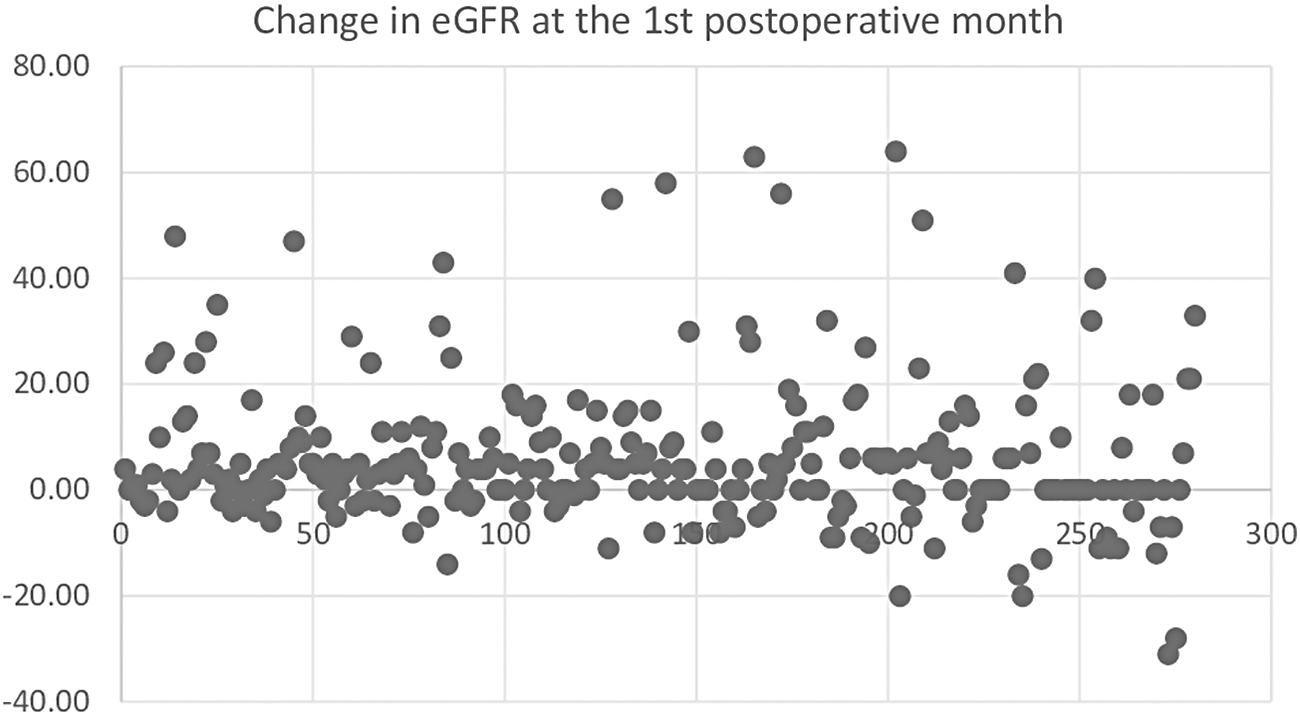
Change in eGFR at the 1st postoperative month. eGFR = estimated glomerular filtration rate.
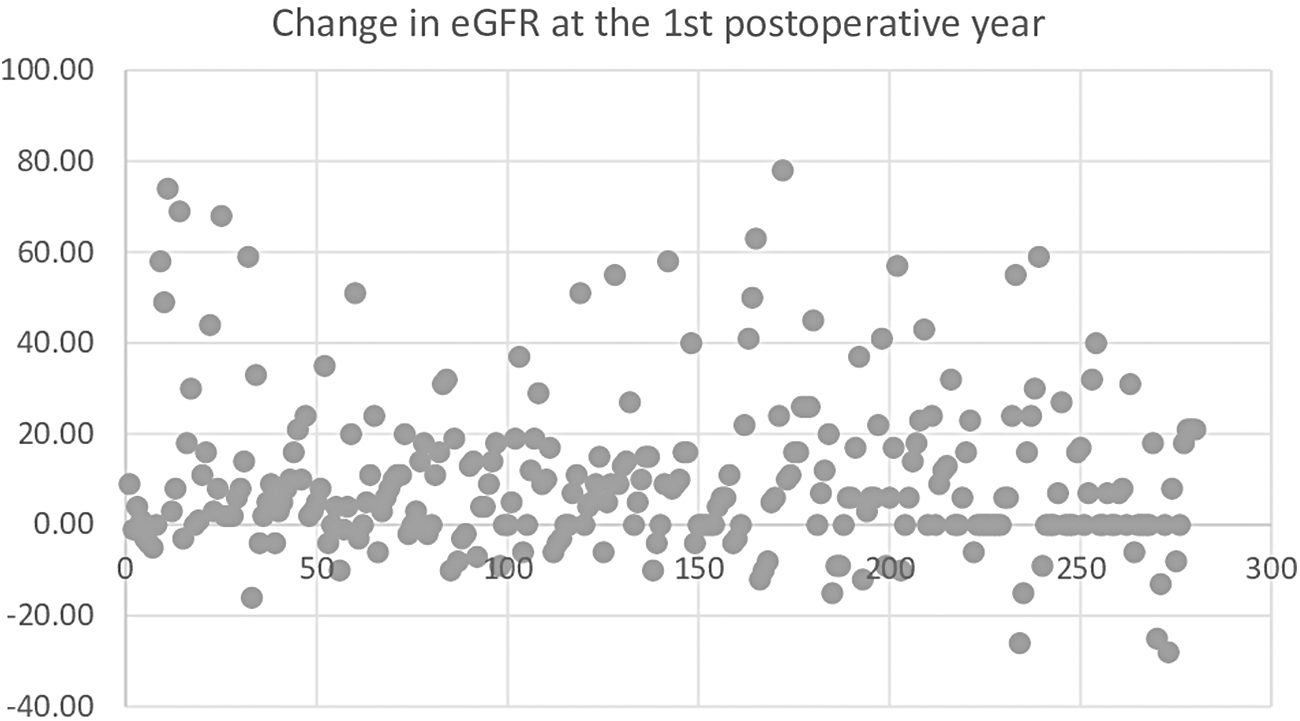
Change in eGFR at the 1st postoperative year.
Estimated Glomerular Filtration Rate Levels at the 1st and 12th Month after Surgery in Patients with Chronic Kidney Disease (CKD) According to CKD Stages
Bold type indicates statistically significant values.
mL/min/1.73 m2.
eGFR = estimated glomerular filtration rate.
Compared with preoperative values, the eGFR value was reduced in 61 (21.8%) patients in the 1st postoperative month and 49 (17.5%) patients in the 12th month. When these patients were compared with those in the stable eGFR or recovery group, the mean stone burden and multiaccess rates were found to be higher in the 1st and 12th month after surgery (p = 0.003, p = 0.003, p < 0.001, and p < 0.001, respectively) (Tables 2 and 3). The importance of stone burden on the eGFR has been demonstrated. Multiaccess PCNL was an independent risk factor for renal function deterioration at the 1st and 12th postoperative month on multivariate analysis (odds ratios were 6.94 and 9.46, respectively) (Table 4). Complications and management in patients who underwent PCNL are summarized in Table 5. Other than these parameters, the demographic and operative data were similar in all groups (Tables 2 and 3).
Analysis of Risk Factors for Deterioration of Renal Function After Percutaneous Nephrolithotomy in Patients with Chronic Kidney Disease at the Postoperative 1st Month
Bold type indicates statistically significant values.
Data are expressed as mean ± SD.
Stone free, fragments <3 mm were considered to be significant residue.
BMI = body mass index; CIRF = clinically insignificant residual fragment; DM = diabetes mellitus; HT = hypertension; SD = standard deviation; SF = stone free.
Analysis of Risk Factors for Deterioration of Renal Function After Percutaneous Nephrolithotomy in Patients with Chronic Kidney Disease at the Postoperative 12th Month
Bold type indicates statistically significant values.
Data are expressed as mean ± SD.
Stone free, fragments <3 mm were considered to be significant residue.
Univariate and Multivariate Analyses of Risk Factors for Deterioration of Kidney Function at Postoperative 1st and 12th Months
Bold values are statistically significant.
CI = confidence interval; OR = odds ratio.
Complications of Percutaneous Nephrolithotomy in Chronic Kidney Disease Groups
Discussion
Kidney stone disease is a risk factor for CKD, and the incidence of renal dysfunction or the need for renal replacement therapy in this patient group is approximately twice that of the general population. 1,7 Included in the etiology of renal failure in patients with kidney stones are renal obstruction, urinary tract infections, frequent surgical interventions, and concomitant diseases. 8 –10 The duration of stone disease, presence of multiple procedures, and stone recurrence have been shown to have a negative effect on renal function. 11 Therefore, management of kidney stone disease in patients with CKD plays an important role in improving renal function and preventing the need for renal replacement therapy. PCNL has been safely applied for a long time in the treatment of patients with comorbid conditions, such as CKD, as well as treatment of kidney stones >2 cm. 4 However, there are insufficient data in the literature about the long-term effects of PCNL, especially in CKD. In this study, we evaluated patients with different stages of CKD and who underwent PCNL for kidney stones. There was a significant increase in eGFRs in the 1st and 12th postoperative months in all CKD stages, and clearance of kidney stones with PCNL had a positive impact on renal function. However, compared with preoperative values, the eGFR value was reduced in 61 (21.8%) patients in the 1st postoperative month and 49 (17.5%) patients in the 1st year. When these patients were compared with those in the stable eGFR or increased eGFR group, the most important factor was multiaccess PCNL.
In 1980, Witherow and Wickham reported a significant increase in the mean creatinine clearance after nephrolithotomy was performed due to stone disease in patients with CKD. 11 Furthermore, laboratory and clinical studies have shown that percutaneous procedures do not cause significant damage to functional nephrons. 5,12,13 Bilen and colleagues evaluated 185 patients with a preoperative eGFR of <60 mL/min/1.73 m2 and found a significant increase in the GFR after PCNL in patients with CKD (especially those with end-stage renal disease). 3 Similarly, Canes and colleagues reported a protective effect of PCNL on the renal function of solitary kidneys. 14
Kuzgunbay and colleagues 15 assessed 19 patients who had preoperative serum creatinine values >1.4 mg/dL and who underwent PCNL due to kidney stones and showed improvement in or stabilization of renal function after PCNL in most patients presenting with kidney stone disease and renal failure. In addition, the authors suggested that patients with a solitary kidney and those with comorbidities, such as diabetes and atherosclerosis, might be at greater risk of renal function deterioration. 15 In another study, Agrawal and colleagues published their PCNL experience with 78 patients who had calculus nephropathy and advanced renal insufficiency and concluded that the percutaneous endourological approach was the most promising method for this patient group. 16 However, 11 patients had the same renal function or deterioration. They concluded that patients with severe azotemia, pyonephrosis, and reduced parenchymal thickness were unlikely to show improvements in renal function. 16 Kukreja and colleagues 6 presented data on progression of renal function in 84 CKD patients with renal stones after PCNL. The patients in the study were classified as improved, stabilized, or deteriorated depending upon the percentage variation in follow-up serum creatinine levels. The factors predicting deterioration in renal function were proteinuria (>300 mg/day), atrophic cortex (<5 mm), recurrent urinary tract infection, stone bulk (>1500 mm2), and pediatric age group. 6 Ozden and colleagues found that diabetes mellitus was an independent predictive factor of renal function impairment. 17
In patients with CKD, PCNL provides a high stone-free rate. 3,18 Kurien and colleagues reported that they achieved a high stone-free rate (83.7%) in 91 patients with CKD. 4 Similarly, Etemadian and colleagues calculated a high stone-free rate of 83.3% in CKD patients. 19 In the current study, we divided the patients into three groups according to the CKD stage and found high and similar stone-free rates in all groups (p = 0.56, 0.4, and 0.67 for groups 1, 2, and 3, respectively). The limitations of the current study include its retrospective nature and the fact that multiple surgeons performed the PCNL procedures. We did not have sufficient follow-up data to evaluate the predictive factors affecting the deterioration of renal function.
Conclusion
PCNL was found to have a positive effect on short- and long-term eGFRs in patients with CKD. However, multiaccess PCNL may have adversely affected eGFRs in both the short and long term.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
No funding was received for this article.