
Abstract
Objective:
The objective is to compare robotic sacral colpopexy (RSC) utilizing autologous fascia lata with RSC with synthetic mesh in the treatment of pelvic organ prolapse (POP).
Methods:
We performed a prospective nonrandomized case comparison trial at a single institution. We compared RSC utilizing either synthetic mesh or autologous fascia lata in women with symptomatic POP, stages II through IV. The primary outcome was anatomic prolapse recurrence determined by the Pelvic Organ Prolapse Quantification (POP-Q) examination. Secondary outcomes included patient-reported outcomes such as the Urogenital Distress Inventory-6 (UDI-6) and Incontinence Impact Questionnaire-7 (IIQ-7). Complications were also recorded and categorized using the Clavien–Dindo (CD) system. The hypothesis is that autologous fascia lata would provide equivalent anatomic and patient-reported outcomes compared with mesh while eliminating mesh-related complications.
Results:
Sixty-four women underwent RSC with 19 (29.7%) receiving fascia lata graft. The overall operative time was greater in the fascia lata group with mean fascia lata harvest time of 24.8 ± 7.4 minutes. Intragroup comparisons of the fascia and mesh groups demonstrated significant improvement in pelvic measurements as well as patient-reported outcomes. Intergroup comparison demonstrated equivalent success rates at 12.1 ± 8.7 months follow-up. There was one apical failure in the fascia lata RSC group; however, the difference was not statistically significant (p = 0.30). Significant complications in the fascia lata harvest group included two CD-II and one CD-IIIb. In the mesh group there was one mesh erosion requiring surgical excision (CD-IIIb).
Conclusion:
This is the first comparison between RSC with autologous fascia lata and mesh. Short-term anatomic outcomes were similar with autologous fascia lata use without the risk of mesh erosion. Morbidity from graft harvest site was not trivial. These results emphasize the need for a randomized controlled trial.
Introduction
Pelvic floor disorders include a variety of clinical conditions including pelvic organ prolapse (POP), urinary incontinence, and fecal incontinence. 1 POP includes anterior vaginal prolapse, apical or uterine descent, and posterior vaginal prolapse. 1 POP is a common problem among the aging female population and its prevalence is steadily increasing. POP, when defined by symptoms, has a prevalence of 3% to 6%, but when based upon vaginal examination can be as prevalent as 50% in the female population. 2 It is predicted that the number of women with at least one pelvic floor disorder will increase from 28.1 million in 2010 to 43.8 million by 2050. 3
Sacral colpopexy is considered the most effective and durable treatment for advanced apical prolapse. 4 The goal is to resuspend the vagina to its anatomically correct position by securing the vaginal apex to the sacrum. This can be approached using a variety of techniques, including the use of either autologous tissue or mesh. Latini and Kreder were the first to report on autologous fascia lata. 5 Years later, robotic sacral colpopexy (RSC) has been established as a safe and effective approach. RSC has been shown to have similar long-term outcomes when compared with the open abdominal approach, with failure rates of 4.2% to 12% depending on how failure is defined. 6,7 Previous studies have demonstrated a longer operative time for RSC, but decreased length of stay and blood loss. 8 The number of RSC procedures has increased considerably in North America in recent years, making it the fastest growing approach for sacral colpopexy. 9
Mesh is considered the gold standard option for apical prolapse, with fewer reported failures than tissue-based repairs. 10 The main complications associated with mesh use include suture and mesh erosion. 11 With current Food and Drug Administration (FDA) warnings and patient safety concerns regarding vaginal mesh, patients and surgeons have a renewed interest in developing alternative mesh-free solutions. Autologous fascia RSC has been effective with minimal apical prolapse recurrences in the short term, within a small series. 12 To date, no comparison study has been published regarding the comparative efficacy and safety of mesh vs autologous fascia during RSC. We hope to fill a critical need in the literature, given the prevalence of POP and the rising popularity of RSC. 9
We present our recent experience with mesh and autologous fascia lata during RSC at a single institution by a single female pelvic medicine and reconstructive surgeon (FPMRS) fellowship trained surgeon. We report the operative and postoperative outcomes associated with mesh compared with autologous fascia lata. The hypothesis is that although the complications and operative times will likely differ, fascia lata will be noninferior to mesh and will avoid mesh-related complications.
Materials and Methods
This study was approved by the institutional review board of Indiana University. A prospective nonrandomized case comparison trial was designed and conducted at a single institution between November 2017 and December 2019. Eligible patients included women undergoing RSC with or without concomitant supracervical hysterectomy and/or urethral sling. All patients who underwent RSC during the study period were analyzed. The technique has been previously described. 11,13
Patients were not randomized. The decision to use mesh vs autologous fascia lata was the result of an informed discussion and shared decision making between the physician and patient during preoperative counseling. The associated risks and benefits unique to each were described, including the FDA black box warnings (2008, 2011) regarding utilization of mesh as well as the risk of seroma, hematoma, thigh numbness, pain, muscle bulge, and deep vein thrombosis (DVT) associated with fascia lata. 14 The fascia was primarily harvested from the right lower extremity unless the patient had prior lower extremity surgery or specific laterality request.
Patient data were extracted from medical records and patient surveys. Data analyzed included preoperative demographics, operative timing, postoperative hospital stay, surgical complications, Pelvic Organ Prolapse Quantification (POP-Q) examination, and patient-reported outcomes including Urogenital Distress Inventory-6 (UDI-6) and Incontinence Impact Questionnaire-7 (IIQ-7). 15
POP-Q stage was defined according to standard criteria as defined by the International Continence Society and American Urogynecologic Society. 16 Recurrence was defined as >0 in any compartment on postoperative POP-Q examination (Aa, Ba, Ap, Bp). Recurrence at the apex was defined as ≥2 cm of apical descent as determined by point C relative to total vaginal length. Complications were categorized using the Clavien–Dindo (CD) classification system. 17
Harvest of the fascia lata graft
The surgical technique has been previously described. 18 A key element is to begin harvesting at least 5 cm cephalad and lateral to the patella after identifying Gerdy's Tubercle on the anterolateral aspect of the tibia, the point at which the tensor fascia lata coalesces into the iliotibial band. The longitudinal integrity of the ileotibial band must never be compromised making its identification crucial (Fig. 1). Using malleable retractors and blunt dissection, a sizeable graft can be harvested from a 4 cm incision. The graft can then be fashioned in a Y-configuration or sling using nonabsorbable 0-monofilament (Figs. 2 and 3).
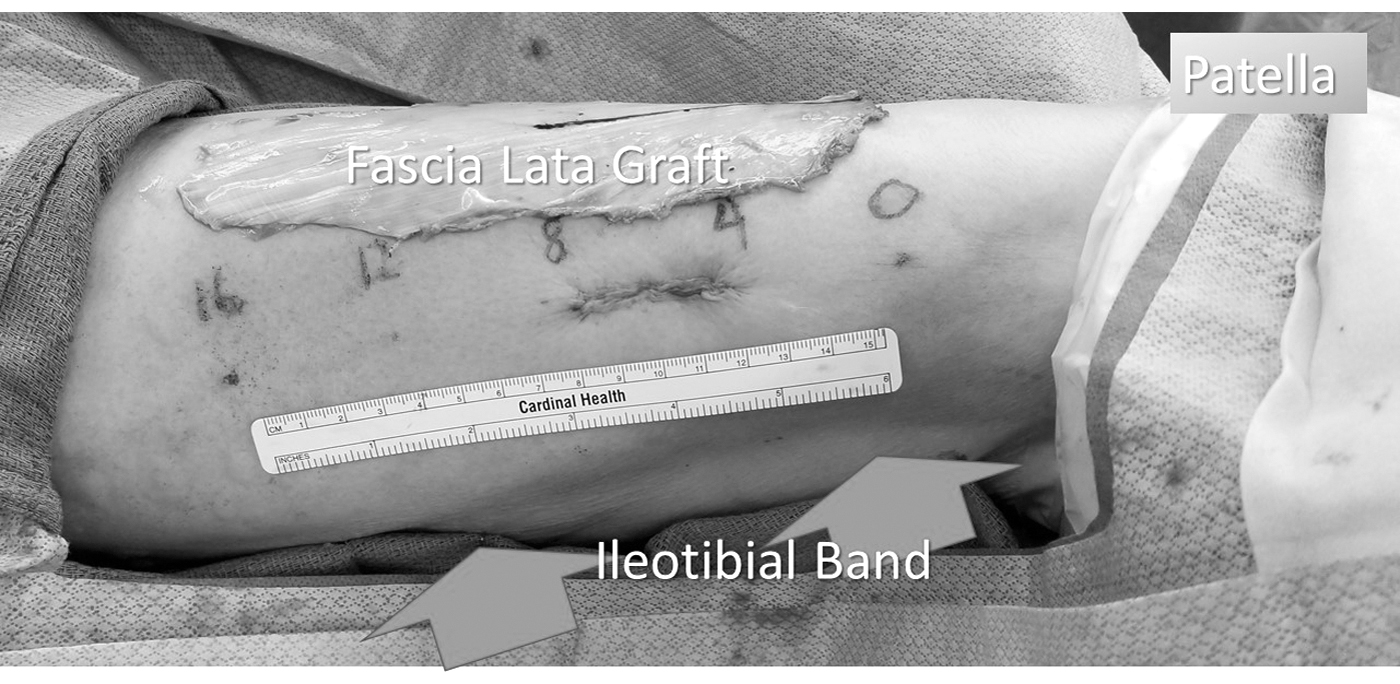
Sample harvest site and fascia lata graft. This figure shows a 16 cm fascia lata graft obtained through a 4 cm skin incision. The graft is harvested anterior to the iliotibial band.

Sample fascia harvest. Multiple fascial pieces can be obtained from a single incision and harvest of fascia lata. This demonstrates fascia configured for posterior (P), anterior (AN), sacral (S), and pubovaginal sling (TVT).

Y configuration. The fascia graft is configured into a Y configuration using 0-nonabsorbable monofilament. Two leaflets will be secured to the anterior and posterior vagina, while the segment labeled “S” will be secured to the sacrum.
Statistical analysis
Statistical comparisons were principally performed preoperatively and at the most recent postoperative visit for each patient using paired t-test. All statistical analyses were conducted with STATA SE version 16 (College Station, TX) as well as Microsoft Excel (Microsoft, Redmond, WA). Continuous variables were summarized using means and medians. Categorical variables were summarized using frequencies and percentages. Continuous variables were analyzed using two tailed t-test and categorical variables were analyzed using Fisher's exact test. A p-value <0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 64 women elected to undergo RSC from 2017 through 2019. Nineteen (29.7%) elected autologous fascia lata RSC and 45 (70.3%) chose mesh RSC. Baseline clinical characteristics were similar between the surgical groups and are summarized in Table 1. Women who elected to undergo fascia lata graft harvest tended to be younger (mean age 59.3 ± 12.9 years vs 67.9 ± 10.7 years, p = 0.01). Gravidity was 2.3 vs 3.3 (p = 0.03), parity was 2.1 vs 3.0 (p = 0.02), and the majority were by vaginal delivery (1.8 vs 2.9, p = 0.01). Women receiving autologous grafts were more likely to be diabetic (p = 0.01), but no difference was seen with regard to body mass index or smoking status. Women receiving autologous grafts were also more likely to receive concomitant fascia slings (p < 0.001), and those undergoing mesh sacral colpopexy were more likely to undergo mesh sling instead of fascia sling, but there were no significant differences between the two groups regarding other concomitant procedures including supracervical or total hysterectomy, anterior or posterior colporrhaphy, or enterocele repair. Pooled analysis of either concomitant mid-urethral or fascia sling in women receiving autologous grafts vs mesh demonstrated no difference.
Demographics, Baseline Pelvic Measurements, and Urinary Symptoms
Summarized by mean (range).
Summarized by mean (standard deviation).
Summarized by median (range).
BMI = body mass index; GH = genital hiatus; IIQ-7 = Incontinence Impact Questionnaire-7; NS = not significant; PB = perineal body; POP-Q = Pelvic Organ Prolapse Quantification; SUI/POP = stress urinary incontinence/pelvic organ prolapsed; TVL = total vaginal length; UDI-6 = Urogenital Distress Inventory-6.
Symptomatically, patients undergoing mesh vs fascia lata had no difference in preoperative frequency, urgency, or incontinence (Table 1). There were no significant differences in patient-reported UDI-6 and IIQ-7 surveys. Preoperatively, pelvic measurements according to POP-Q examination were similar in all categories as well as POP-Q stage. At the time of surgery, all patients had ≥2 cm apical descent with median POP-Q stage of 3 in both groups.
Operative details
Operative details are outlined in Table 2. Eight of 19 (42.1%) patients underwent concomitant robotic supracervical hysterectomy in the fascia lata group compared with 16 of 45 (35.6%) patients in the mesh group (p = 0.78). The average operative time for RSC with fascia was 288 ± 39 minutes compared with 237 ± 31 minutes for mesh (p < 0.001). Harvesting fascia required a mean of 24.8 ± 7.4 minutes. There were six (31.6%) patients in the fascia group who underwent concomitant pubovaginal autologous sling and eight (17.8%) patients in the mesh group who underwent concomitant mid-urethral mesh sling. Both mesh and fascia were secured to the vaginal wall using a running delayed absorbable 2-0 monofilament suture with three nonabsorbable 0 monofilament sutures for sacral fixation (range 2–4) as described previously. 13 The average hospital stay for both groups was 1.0 ± 0.7 days. There was no difference between the two groups regarding estimated blood loss and postoperative urinary retention requiring a foley catheter. There were no patients requiring catheterization at the 1 month mark.
Operative Details
Summarized by mean (range).
Summarized by median (range).
POD1 = postoperative day 1.
For autologous fascia lata harvest, the average length of the graft was 18.3 ± 2.5 cm and width was 4.2 ± 1.4 cm (Fig. 1).
Postoperative outcomes
Intragroup outcomes demonstrated postoperative improvement on all clinical and patient-reported outcomes for fascia lata (Table 3) and mesh (Table 4). An intergroup comparison of clinical and patient-reported outcomes is displayed in Table 5. Overall patient-reported outcomes were similar between fascia lata and mesh. There was increased urinary frequency in the mesh group (p = 0.03) and increased de novo stress incontinence seen in the fascia lata group (p = 0.02). With regard to patient-reported outcomes, there was no difference seen on the UDI-6, but an increased total score in the fascia lata group on the IIQ-7 (p = 0.05). Anatomic outcomes were not significantly different between groups. The vast majority of patients in both groups exhibited POP-Q stage 2 or less (94.8% in fascia and 97.8% in mesh). One patient in the fascia lata group exhibited failure in both the anterior and apical compartments. The mesh group had five recurrences in the posterior compartment and one failure in the anterior compartment at a combined mean follow-up of 12.1 ± 8.2 months. The differences in recurrence were not statistically significant (Table 5).
Combined Outcomes for Fascia Lata
Summarized by mean (standard deviation).
Summarized by median (range).
Combined Outcomes for Mesh
Summarized by mean (standard deviation).
Summarized by median (range).
Postoperative Comparison Fascia Lata vs Mesh
Summarized by mean (standard deviation).
Summarized by median (range).
Postoperative complications
In the fascia lata group, one patient developed acute tubular necrosis that resolved with intravenous fluid resuscitation (CD-II), one developed unilateral hydronephrosis requiring ureteral stent and balloon dilation of the affected ureter that is resolved on follow-up ultrasound 3 months later (CD-IIIb), one hematoma at the harvest site requiring transfusion (CD-II), and one ipsilateral DVT (CD-II). In the mesh group, one mesh erosion was noted requiring vaginal mesh excision (CD-IIIb).
Morbidity from the harvest site is summarized in Table 6. Notably, this included swelling (10.5%), paresthesia that resolved (5.3%), paresthesia that remained unresolved (5.3%), hematoma (5.3%), and seroma (10.5%). Notably, there were no complaints of persistent pain and no wound infections.
Site-Specific Complications Associated with Fascia Lata Harvest
DVT = deep vein thrombosis.
Discussion
There is limited literature on autologous fascia lata sacral colpopexy, mostly consisting of small case series with short-term outcomes. 12,19 This is the first comparison to our knowledge between RSC with autologous fascia lata and mesh. Despite some noted limitations, this study demonstrates that RSC with autologous fascia lata has similar short-term anatomic outcomes to mesh for women with apical POP.
What remains unknown is the long-term durability of autologous fascia lata. Freeze-dried cadaveric fascia lata has previously demonstrated poor 12-month outcomes and poor 5-year outcomes with 62% success rate compared with 93% for mesh; however, that analysis was post hoc and included only 58 of 100 original subjects. 18,20 The hypothesis is that cadaveric fascia promotes an immune response that compromises the integrity of the tissue. It is possible that autologous fascia lata may prove more durable given that it does not promote the immune response.
This investigation aimed to capture both anatomic and patient-reported outcomes. There was a single anatomic failure within the fascia group with apical prolapse and anterior wall laxity, which will require surgical revision. There were no posterior recurrences in the fascia group, whereas the mesh group had five posterior failures and a single recurrent cystocele. The recurrent cystocele required revision with an anterior vaginal wall suspension. It is important to note that none of the patients received a concomitant anterior nor posterior repair at the time of SCP, a practice that some follow and that might decrease the compartment-specific failure rate. It is also important to note that in a small series like this, the concomitant pubovaginal sling might support the anterior vaginal wall more effectively than the mesh sling, and both might support better than no concomitant procedure, although slings are not intended to do this. The primary outcome was apical failure, which would not be influenced by concomitant procedures such as sling, anterior repair, posterior repair, or enterocele. The compartment-specific outcomes, as well as the patient-reported outcomes, will be influenced by an unbalanced application of these procedures. For this reason, Fisher's exact test was performed to detect bias that might suggest that one cohort received compartment-specific repairs more often than the other. Those results are given in Table 2.
Our findings are similar to those of Scott et al. who demonstrated no recurrent apical prolapse, but a 25% recurrence of anterior vaginal wall prolapse in 12 patients who underwent RSC with autologous fascia lata. 12 Alternatively, Latini and colleagues reported a 100% success rate without apical descent at 18 months in a group of 10 women who underwent open sacral colpopexy with autologous fascia lata. 5 This suggests that RSC with autologous fascia provides comparable tensile strength in the short term for apical fixation to synthetic alternatives. The success rates can be expected to decline with longer follow-up, and our intention is to follow the fascia cohort for 5 years and compare directly with the mesh cohort. Furthermore, the data described will be used for power calculations in the design of a prospective randomized controlled trial (RCT) to further explore the hypothesis.
The low rates of serious adverse events associated with both methods are consistent with prior clinical studies. 5 Our mesh exposure rate of 2.2% is comparable with the 1.5% to 8% noted in a recent review of 13 randomized clinical trials describing sacral colpopexy. 4 The single patient who suffered a mesh exposure event requested a revision, which was effective. The immediate morbidity of the fascia lata harvest site must be taken into careful consideration and discussed during preoperative counseling. Patients undergoing graft harvest are at risk for site-specific complications, including site swelling, numbness, hematoma, and seroma, which has been previously described. 12 The majority of these were self-limiting and typically resolved with expectant management. No patients demonstrated functional or ambulatory deficits as a result of graft harvest. There was a single incidence of harvest site hematoma requiring transfusion and one DVT requiring anticoagulation. The DVT is troublesome and all fascia lata harvest patients are now given prolonged venous thromboembolism prophylaxis similar to that in lower extremity orthopedic procedures. 21 Another patient required aspiration of a thigh seroma. However, postoperative seromas are usually small and resolve on their own and as such our group discourages intervention. These findings highlight the importance of preoperative counseling and raise the important question of how much harvest site morbidity is acceptable to avoid the risks of synthetic mesh.
Quality of life is integral to guiding treatment and evaluating the treatment outcomes of POP. This study captured patient-reported outcomes using the validated IIQ-7 and UDI-6 questionnaires that reflect urinary symptoms, pelvic discomfort, and quality-of-life measures related to POP. Both groups demonstrated significant improvement in patient-reported outcomes postoperatively. The fascia lata group reported higher IIQ-7 scores than the mesh group, which parallels an increase in de novo stress urinary incontinence (SUI) found in this group. However, none of the patients reporting new onset SUI have elected to proceed with sling placement, suggesting symptoms were mild.
Interestingly, women who elected to undergo fascial harvest tended to be younger. The reasoning behind this could be twofold. The younger population may be more concerned regarding the long-term risks of mesh including vaginal erosion and dyspareunia. They also may be more willing to try a new technique and expect a quick recovery despite the extra harvest site incision.
Weaknesses and limitations
This study has several weaknesses that should be mentioned. It is a single-surgeon single-institution case series that limits the generalizability of the findings. The numbers were small and the follow-up was relatively short at 12.1 months. The groups were not evenly matched, the fascia lata group was significantly younger and less parous than the mesh group. This can of course introduce bias. Despite a significant difference in age and parity between the two groups, the preoperative POP-Q measurements, UDI-6, and IIQ-7 responses were similar.
Conclusions
This is the first prospective comparison of RSC using autologous fascia lata with mesh. Fascia lata RSC appears to have comparable short-term success rates with mesh RSC and acceptable but higher than expected morbidity related to the graft site with increased operative time. The knowledge gained and questions raised underscore the need for a RCT. An instructive video describing the technique has been published and the technique is possible for any surgeon familiar with RSC to learn. 22
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.