
Abstract
Introduction:
Supracostal access for percutaneous nephrolithotomy (PNL) has a known increased risk for thoracic complications (TCs). In this study, we perform a radiological review of preoperative and postoperative abdominal CT scans to assess the relationship of the upper pole of the kidney with surrounding landmarks to determine radiographic predictors of TCs.
Methods:
We performed a retrospective matched cohort comparison of patients who underwent supracostal PNL with and without TCs from 2012 to 2019. An experienced genitourinary (GU) radiologist reviewed pre- and postoperative CT scans to measure the craniocaudal distance between the upper renal pole and the most superior calix to the upper edge of the tip of the 12th rib, the costophrenic angle, and the posterior insertion of the diaphragm.
Results:
We identified 19 patients who developed TCs after undergoing PNL and compared their CT scans with 24 control patients without TCs. On a preoperative abdominal CT scan, the relationship of the upper edge of the renal parenchyma or upper pole calix with the superior edge of the tip of the 12th rib or costophrenic angle was not found to be predictive of TCs. On receiver operating characteristic analysis, diaphragmatic insertion of ≤2.5 cm below the upper edge of the renal parenchyma on sagittal and transverse views was predictive of TCs (p = 0.046). On postoperative CT scan, the percutaneous nephrostomy tract traversed the posterior insertion of the diaphragm in 80% of patients who had TCs compared with 20% of patients who had no TCs.
Conclusions:
The decreased distance between the posterior insertion of the diaphragm (medial and lateral arcuate ligaments) and the superior edge of the renal upper pole on preoperative CT scan was associated with TCs from supracostal puncture during PNL. Critical preoperative recognition of this anatomic relationship can help preoperative planning and patient counseling and may prevent or reduce TCs.
Introduction
Percutaneous nephrolithotomy (PNL) remains the surgical treatment of choice for complex stones, large stone burden (>2 cm), or stones with associated renal anomalies such as horseshoe kidneys or caliceal diverticula. Stone clearance is dependent upon obtaining optimal entry into the collecting system to directly access the stone. An upper caliceal entry can provide an optimal percutaneous tract that is parallel to the longitudinal axis of the kidney, providing ease of entry into the inferior calices, renal pelvis, and proximal ureter without excessive torque on the kidney. Upper pole access is particularly favorable in situations with complete staghorn stones, superior caliceal stones, complex inferior staghorn stones, and proximal ureteral stones. 1,2
In some cases, upper pole access can only be achieved with a supracostal (above the 12th or 11th rib) percutaneous puncture. The earliest series on supracostal access for PNL was published by Picus and colleagues in 1986, demonstrating a thoracic complication (TC) rate of 12%. 3 Since then, multiple studies have shown the efficacy of the supracostal approach with an excellent stone clearance rate, although demonstrating a higher risk of TCs, including pneumothorax, hydrothorax, hemothorax, and pleural effusion, compared with the traditional infracostal access. 1,2,4 –8
A systematic examination of cross-sectional renal imaging before surgery is essential for selecting the most strategic target for percutaneous access while minimizing the risk of thoracic cavity violation. While this standard practice is universally practiced by all endourologists, to our knowledge, there is no described strategic use of preoperative CT for studying the relationship of anatomic factors around the upper pole of the kidney to predict the risk of TCs when choosing supracostal access for PNL. In this study, we perform a radiological review of preoperative CT to determine the risk of TCs during supracostal percutaneous access by the assessment of the relationship between the upper pole of the kidney and surrounding landmarks.
Methods
The Institutional Review Board (IRB) for study design was submitted and approved prior to initiation of the study. After IRB approval was obtained, we performed a retrospective analysis of the Washington University School of Medicine urolithiasis database. We identified patients who underwent PNL through supracostal access from 2012 to 2019. Over the study period, our institution has performed 697 cases, of which 386 (55%) were supracostal access. Our cohort included the experience of three experienced endourologists, of which two (A.D.) utilized interventional radiology (IR) assistance with percutaneous access and one (R.V.) routinely obtained his own fluoroscopy-guided access. All operative reports and postoperative CT scans were reviewed to confirm supracostal access. A radiographic query utilizing key words, including “pleural effusion,” hemothorax,” “pneumothorax,” and “hydrothorax,” identified a cohort of patients who developed TCs as a result of supracostal access during PNL (Group 1). This cohort was compared with an unmatched control group (Group 2) who also underwent supracostal percutaneous access, but did not develop TCs during the same time period. Cases selected for the control group were based on most recent consecutive PNLs completed with supracostal access and without TCs and limited to patients who had preoperative and postoperative CT images available for review. We collected patient characteristics, including age, gender, and body mass index (BMI), stone characteristics, including volume and location, laterality, incidence of postoperative stone clearance, TCs, and whether any intervention (Clavien grade 3) was required for TCs. Estimated stone volume was calculated using an ellipsoid formula (stone volume = π*L*W*D* 0.167), with L being the length, W the width, and D the depth and stone diameter measured in the widest dimension. 9 If multiple stones were present, each stone volume was calculated independently and added to determine a total volume. Stone volume was not calculated for complete staghorn stones.
All the patients in this study cohort underwent PNL in the prone position under fluoroscopy-guided percutaneous access, utilizing the bullseye technique in AP and oblique views. Access by IR was performed with the same technique (prone position, fluoroscopic guidance, and bullseye technique) in the urology operating room before PNL. After administration of general anesthesia and securement of the airway, the patient was placed in the prone position with the legs abducted on a split-leg bed to allow for retrograde access if needed. Maneuvers were made to descend the kidney as low as possible during supracostal access, including deep inspiration and suspension of breath by the anesthesiologist. All percutaneous tracts were radially dilated with a single dilating balloon, followed by insertion of a 24–30F Amplatz sheath. Some patients had no PCN tube placed after the procedure. All patients underwent a postoperative chest X-ray in the recovery room. All patients underwent a postoperative noncontrast CT scan of the abdomen on postoperative day 1.
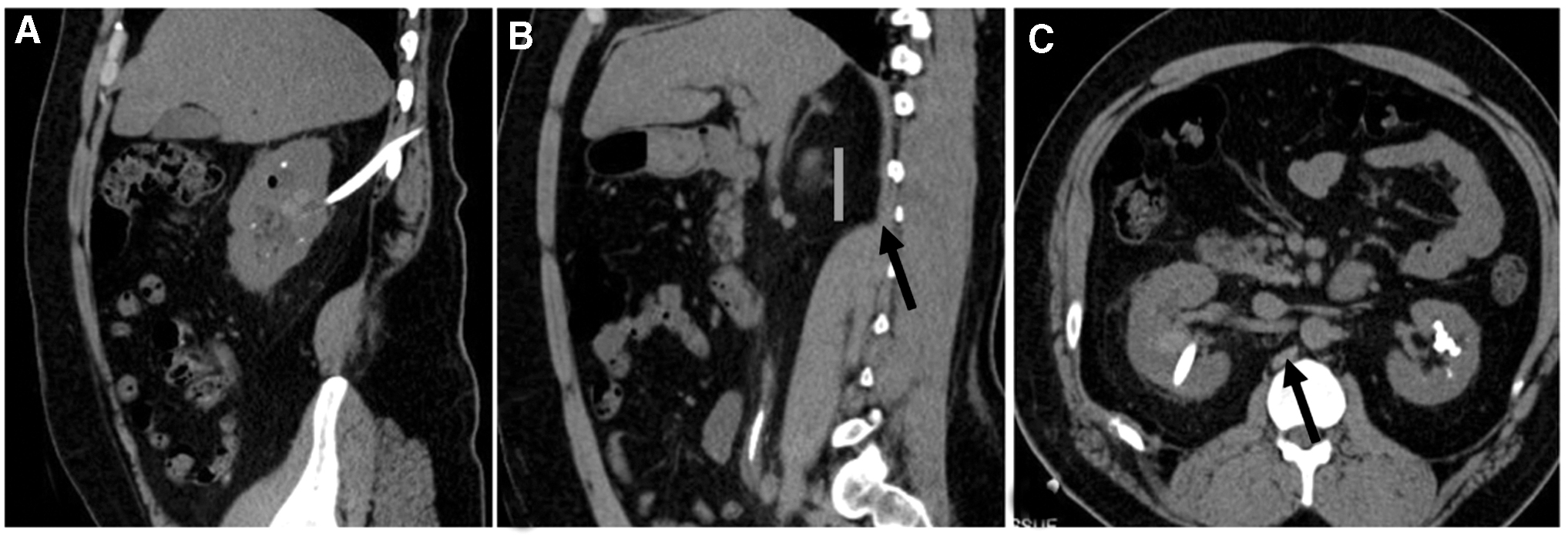
To standardize measurements and to mitigate interobserver variability of measured distance, a single experienced genitourinary radiologist (C.S.) reviewed both pre- and post-CT scans. We studied the CT scan for relative location of the upper pole of the kidney to relevant thoracic anatomic landmarks. Anatomic landmarks of interest reviewed on abdominal and pelvic CT included the craniocaudal distance (CCD) from the upper edge of the renal capsule to the upper edge of the tip of the 12th rib, the costophrenic angle, and the posterior insertion of the diaphragmatic leaf in the sagittal view. By convention, the upper edge of the renal capsule was set at zero and landmarks noted cranial to this reference point were set as positive measurements and landmarks caudal to the reference point were set as negative measurements. CCD was also determined between the most superior calix and the aforementioned three relevant anatomic landmarks. In the same manner, by convention, the most cephalad extent of the superior calix was set at zero and landmarks were measured relative to this reference point (− for caudal and + for cranial to the reference point). Measurements were performed in the sagittal and transverse orientations. Figures 1–3 show examples of such measurements. An experienced genitourinary radiologist (CS) reviewed the preoperative CT scans in the axial and sagittal planes of both groups to document CCD measurements. Postoperative CT scans were also reviewed for TCs, stone clearance, and nephrostomy tract position in relation to the anatomic factors described above. Stone clearance in our study was defined as the complete absence of or <2-mm stone fragments on the postprocedural CT scan.
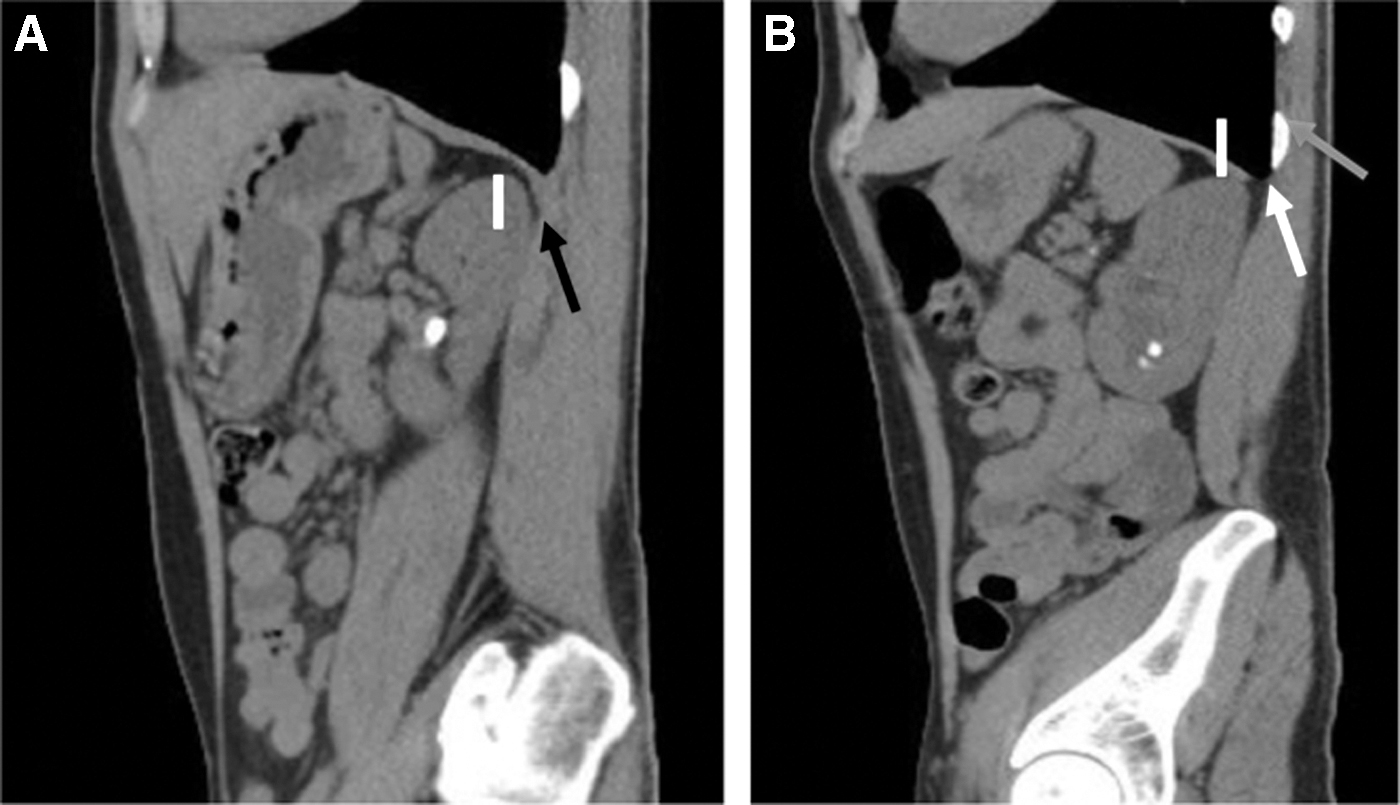
Representation of CCD measurement on sagittal CT. Patient with a TC following supracostal access.
Patient with no thoracic complication following supracostal access.

The Wilcoxon rank-sum test and Fisher's exact test were used to assess statistically significant differences between Group 1 and Group 2 for quantitative and qualitative variables, respectively. All analyses were performed using R, version 3.5.2. Statistical significance was set to p < 0.05.
Results
We identified 19 patients who developed TCs after undergoing supracostal access for PNL (Group 1) and 24 patients in the control group (Group 2). Mean patient age was 49 (31–80) years vs 59 (18–68) years, respectively (p = 0.007). There were 10 males and 9 females in Group 1 and 13 males and 11 females in Group 2 (p = 1.00). Average BMI was 26.8 (18.5–36.3) kg/m2 and 31.9 (14–42.3) kg/m2 in Group 1 and Group 2, respectively (p = 0.02). Additional comparison of patient and stone characteristics between the two groups is displayed in Table 1. In 29 cases (67%), percutaneous access was obtained by the urologist, and in 14 cases (33%), it was obtained by IR. Supracostal access was obtained by the urologist in 5/19 (26%) patients in Group 1 and 24/24 (100%) patients in Group 2 (p = 0.001). Two patients in Group 1 had supra-11th rib access, while the remainder (42) had supra-12th rib access. Complete stone clearance, as determined by postoperative CT, was achieved in 57.9% of Group 1 and 50% of Group 2 on postoperative CT scan on postoperative day 1.
Patient-Specific and Stone Characteristics
BMI = body mass index; IR = interventional radiology; TC = thoracic complication.
In Group 1, 10 (52%) patients had normal chest X-rays taken in the immediate postprocedural period in the recovery room. All Group 2 patients had normal postprocedural chest X-rays in the recovery room. In Group 1, TCs identified on postoperative CT included pneumothorax (7), hemothorax (3), hydrothorax (8), and empyema (1). Of the TCs, 11 were on the right and 8 were on the left; 10/19 (52.6%) patients required a chest tube placement to address the TC. One patient (5.2%) required aspiration of a pleural effusion under local anesthesia without the need for chest tube placement. With regard to postoperative drainage, three patients had ureteral stents only, two patients had nephrostomy tubes (NTs) only, and 14 had both ureteral stents and NTs. All patients had a Foley urethral catheter, which was removed on postoperative day 1. The average length of postsurgical convalescence for Group 1 and Group 2 was 4.83 (standard deviation [SD] 3.09) days and 1.52 (SD 0.6) days, respectively (p = 0.0001). None of the 19 patients with TCs required ICU admission. One patient who was discharged on POD 1 without findings of TCs required readmission on POD 3 with acute chest pain. Imaging revealed a new pneumothorax that required placement of a chest tube. Group 1 had one (5.2%) Clavien-Dindo grade 3a complication and 10 (52.6%) Clavien-Dindo grade 3b complications. There were no grade 3 Clavien-Dindo complications in Group 2.
When comparing the preoperative CT scans between Groups 1 and 2, the CCDs from the upper edge of the renal capsule to the superior edge of the 12th rib and the pleura were not found to be predictive of TCs (p = 0.53 and p = 0.37, respectively). Between the two groups, there was also no difference in CCD between the upper pole calix to the 12th rib and the costophrenic angle (p = 0.41 and p = 0.18, respectively). Refer to Table 2 for complete craniocaudal distance between the two groups. On receiver operating characteristic (ROC) analysis, the posterior diaphragmatic insertion of 2.5 cm inferior to the upper edge of the renal capsule on sagittal and transverse views was predictive of TCs (p = 0.046) (Fig. 4). On postoperative CT, the percutaneous nephrostomy tract traversed the posterior insertion of the diaphragm in 80% of patients who had TCs compared with 20% of patients who had no TCs.
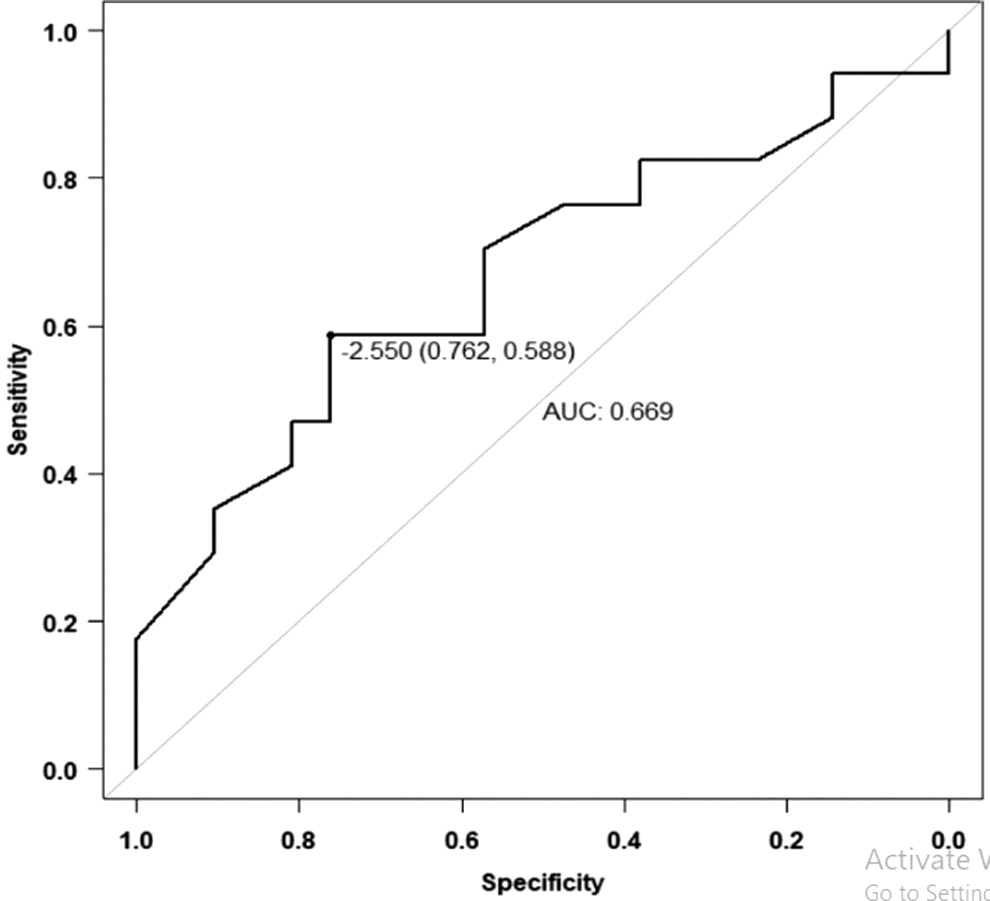
Receiver operating characteristic analysis of the CCD of posterior diaphragmatic insertion to the upper edge of the renal capsule in predicting TCs.
Craniocaudal Distance Comparison Between Groups
SD = standard deviation.
Discussion
Performing a safe supracostal puncture for upper caliceal access is a valuable skill in the endourologist's armamentarium for treatment of complex renal stones.
In general, the superior pole of the kidney is shorter and provides the most direct entry into the collecting system as it is relatively more medial and posterior to the rest of the kidney. Upper pole access is also favored as the trajectory of access runs parallel to the longitudinal axis of the kidney, providing accessibility to all or majority of the calices and the proximal ureter without excessive torque of the access sheath. Utilizing supracostal puncture, studies have boasted high stone clearance rates of 82%–90%. 1,2,5,6
Despite the benefits with supracostal access, particularly the high stone clearance rate, a large collaborative international study (CROES) found that urologists tend to avoid supracostal puncture due to perceived pulmonary complications. 10 As expected, there is a predictive risk escalation of TCs with incrementally higher access. An early study published in the IR literature found that 11th–12th intercostal access conjures pulmonary complications as much as 30% of the time, whereas this risk exponentially rises to 25%–90% in patients with percutaneous access between the 10th and 11th intercostal space. 11 Comparing supracostal with infracostal access, Munver et al. found a significant majority (87.5%) of TCs in a tertiary stone center to occur with supracostal access. 4 Within the last two decades, large, experienced high-volume institutions have reported pulmonary complications ranging from 2.4% to 15% with supracostal access. 1,2,4 –7,12,13 In the same studies, Clavien grade 3 TCs, those requiring pleural drain or thoracentesis, occurred in the range of 1.8%–16% of cases.
Our analysis found the CCD from the superior edge of the renal capsule to the posterior diaphragmatic attachment to be the most reliable predictor of TCs. However, our study did not find the CCD from the superior edge of the renal capsule to the costophrenic angle to be predictive of TCs. Our hypothesis for this difference is that the pleural edge shifts with phases of respiration and thus the CCD to the renal capsule would fluctuate depending on the timing of the scan. The posterior attachment of the diaphragm, on the other hand, is a fixed anatomical structure and it remains independent of patient positioning or respiratory phase. We gather that the greater CCD (>2.5 cm) between the upper pole and the medial arcuate ligament of the diaphragm is protective of TCs as ventilatory inspiration and suspension of breath before puncture, as with our technique, provide a much greater caudal displacement of the upper pole of the kidney away from the pleural space, whereas a shorter CCD of the diaphragmatic attachment (<2.5 cm) will displace the kidney less and the risk of thoracic violation is higher with the needle access. The CCD from the superior aspect of the kidney to the inferior edge of the 12th rib was also not found to be a predictor of TCs. The diaphragm reflection attaches to the medial and inferior border of the 12th rib over the psoas major (medial arcuate ligament) and over the quadratus lumborum (lateral arcuate ligament) and thus supracostal access obtained lateral to the second half of the 12th rib, as in our technique, may avoid violation of the thoracic cavity. 1,5,14
Of note, the risk of pleural violation is, in theory, higher on the left due to the more cephalad positioning of the left kidney, although we did not find TCs to be dependent on laterality in our analysis. 11 Our study found lower BMI and decreasing age associated with TCs, but limitations to this analysis are a reflection of a small cohort. Further investigations on these patient factors are encouraged in the future.
On ROC analysis, our study finds that TCs were higher when the distance between the posterior attachment of the diaphragm and the upper edge of the kidney was 2.5 cm or less. Although this cutoff is only the statistical product of our analysis, the fundamental lesson is the significance of the diaphragmatic slip extending caudal to the superior edge of the kidney. In our experience, based on the above study, noting the relationship of the diaphragmatic insertion and the upper pole of the kidney on the axial and sagittal sections of the CT scan can estimate the risk of TCs in the majority of patients. In these patients, it is easy to determine whether supracostal access has a low or high chance of TCs. In some cases, we could predict that even a supra-11th rib access would have nearly zero risk of TCs (Fig. 3). In other cases, where TC risks are expected to be high, attempts should be made to lower the risk either by lower pole access, an infracostal approach, or maneuvers to descend the kidney.
Patients who developed TCs had an extended length of hospitalization of 3 days compared with patients without TCs. It is important, however, to note that not all patients require ancillary procedures for TCs. In our cohort, patients who were symptomatic, that is, with dyspnea, chest pain, or inflicted with oxygen desaturation, underwent chest tube placement, which amounted to 50% of our patients who developed TCs. None of the patients who had postoperative TCs required admission in the intensive care unit. Of note, 50% of patients who developed TCs had normal chest X-rays in the immediate recovery period. This may reflect the poor sensitivity of the CXR and/or highlight the fact that TCs can present in a delayed manner. One patient who was discharged on POD 1 without findings of TCs or symptoms presented to our emergency room with acute chest pain and was found to have a pneumothorax requiring chest tube placement. Thus, if the index of suspicion for TCs is high, close monitoring of symptoms with prolonged hospitalization is necessary.
Our stone clearance rates in both groups utilizing supracostal access were similar (57.9% vs 50%). We do note that our stone clearance rate is lower than some of the previously published supracostal reports (82%–90%). 1,2,5,6 This can be explained by early CT (POD 1), varying the imaging modality of detecting postoperative stone fragments, and disparate definitions of success rates of stone surgery in the literature. Some studies evaluate for residual stones utilizing postoperative KUB, which is limited by its sensitivity, while other studies use a larger measurement cutoff, that is, <4 mm, to determine the stone-free status. 1,2 In our study, each patient underwent an abdomen and pelvis CT on postoperative day 1 and complete stone clearance was defined as the complete absence of stones or the presence of a solitary punctate calcification (<1–2 mm). One patient in Group 1 and one patient in Group 2 had punctate calcifications, each with a solitary, 1-mm stone fragment identified on postprocedural CT.
Interestingly, urologist-obtained access in our single-center study had fewer TCs. This finding may be confounded by a recency bias as our endourologists now obtain a majority of upper pole access compared with the earlier stage of the study when interventional radiologists were more involved. The difference in complications between IR and urology access may be a statistical anomaly for this reason and conclusions should not be drawn on this matter. However, other comparative studies imply lower complication rates with urologist-obtained access due to better understanding of the risks of TCs and strategic surgical modifications to reduce the complication rate. A comparative study shows that urologists are more apt to perform supracostal access than IR, although there were no comparisons of TCs between the two groups. 15
We recognize the limitations of our study, including the retrospective review of our findings, as well as the small power of the study, limited by the low incidence of TCs (19 in a 7-year period). We also recognize that preoperative CT scans are generally performed in the supine position. Indeed anatomical shifts, including the relationship of the kidney with our measured structures, can vary when supracostal access is performed in the prone or Valdivia position with gel padding. 16 Our study did not utilize ultrasound-guided access, which (in some situations) can help visualize the diaphragm and pleural space during puncture. With the recent increased popularity and use of ultrasound-guided access, future work should be directed to determine whether this modality may mitigate the risk of TCs with supracostal access. Conceivably, in patients with ideal body weight, the diaphragm and pleura can be directly visualized on the ultrasound. Access can also be obtained in sync with the respiratory cycle under direct vision to avoid thoracic violation.
Conclusions
Decreased distance between the posterior insertion of the diaphragm (medial and lateral arcuate ligaments) and the superior edge of the renal upper pole on preoperative CT scan was associated with TCs from supracostal puncture during PNL, likely due to limited caudal displacement of the kidney with ventilatory inspiration and suspension of breath before puncture. A critical assessment of the anatomic relationship of the kidney with diaphragmatic insertion before surgery is important and may prevent or reduce TCs. Adaption of this practice is also useful for preoperative counseling and can help guide decision-making for pursuing the optimal point of percutaneous access to achieve stone clearance while decreasing pulmonary morbidities.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.