
Abstract
Purpose:
Forgotten ureteral stents are associated with safety issues, increased cost, and medicolegal disputes. Tracking ureteral stents is cumbersome because of the variety in placement periods. We developed and validated an electronic medical record (EMR) system-based algorithm for monitoring patients with ureteral stent placements.
Materials and Methods:
The Stent Tracking Algorithm Registry (STAR) is automatically activated once the physician enters the stent placement or replacement billing code into the EMR billing system. At 120 days, an overdue notification is generated and sent to the attending physician through an EMR pop-up dashboard and e-mail. The model is automatically deactivated when the stent of the corresponding laterality is removed. To validate the feasibility of STAR, we performed a retrospective review of 2194 patients who received stent placements between November 2006 and September 2019.
Results:
Among 2194 patients, STAR retrospectively identified 354 (16.1%) patients suspected of harboring forgotten ureteral stents. A total of 12 (0.5%) patients actually had forgotten ureteral stents and were contacted for removal. A total of 124 (5.7%) patients were identified because of the omission of the stent removal billing code, whereas 209 (9.5%) patients were identified because of being lost to follow-up after referral to another health care facility or death. There were no cases in which STAR identified patients whose stents were removed or replaced at an appropriate time frame.
Conclusions:
STAR provides an efficient interface with which to prevent the occurrence of forgotten ureteral stents. This model can be integrated into any EMR system that utilizes coding algorithms.
Introduction
The introduction of ureteral stents to clinical urology has played a pivotal role in the treatment of various clinical conditions, including urolithiasis, ureteral injury, and ureteral stricture or obstruction. 1 Despite its value, tracking patients with ureteral stent placements and planning removal within a specific time frame has become a cumbersome task for urologists. 2 Prolonged stent placement, also referred to as forgotten ureteral stents, exposes the patient to various morbidities, including occlusion, encrustation, fragmentation, urinary tract infection, and renal failure. 3 In an era of prevalent ureteral stent use in urology, intervention radiology, and transplant surgery, ∼12% of all ureteral stents are forgotten. 3
Forgotten ureteral stents are associated with increased health care costs, medicolegal disputes, and most importantly, patient safety. Forgotten stents can result in severe encrustation, which may require invasive endourologic procedures and prolonged treatment periods. 4 Furthermore, mortality rate has been shown to be associated with infectious complications, such as sepsis and renal failure. In addition to morbidity, increased financial burden is another significant consequence. The cost of treatment for forgotten stents has been reported to be seven times higher than that for appropriately scheduled stent removal, because of the extra costs associated with additional imaging studies, intervention, and prolonged treatment. 5 Potential litigation and medicolegal disputes have also been a consistent source of postoperative negligence claims. In a U.K. study, 23 out of 168 postoperative negligence claims were associated with forgotten stents. 6 Altogether, these clearly illustrate the importance of monitoring patients after stent placement. Although patients are informed about scheduled removal or replacement, the attending physician is responsible for both the monitoring and removal of the stent.
A variety of tracking systems utilizing patient records and registries has been developed to prevent forgotten ureteral stents. However, none have been able to resolve this issue completely. To overcome the limited effectiveness of previously reported measures, we developed the Stent Tracking Algorithm Registry (STAR) model. We report our initial experience and validation of STAR, which may effectively be used to facilitate the prevention of forgotten stents.
Materials and Methods
Development of the STAR
STAR was developed to track patients with ureteral stent placements and to prevent failure of retrieval. The concept of the model was developed by a urologist (K.C.K.), and STAR was designed to be integrated into our institutional electronic medical records (EMRs) system by a bioinformatician (H.J.O.).
STAR is automatically activated once the physician enters the prescription code “stent placement, right (R) or left (L)” or “stent replacement right (R) or left (L)” into a specific patient's EMR billing system (Fig. 1). At our institution, ureteral stent replacement within 90 days is recommended to prevent encrustation and subsequent urinary tract infection. Once the system identifies stent placement or a replacement code, an overdue notice is sent to the attending physician at 120 days. If the prescription code “stent removal” of the corresponding laterality of the stent is entered before 120 days, STAR is automatically deactivated. If the prescription code “stent replacement” of the corresponding laterality of the stent is entered before 120 days, STAR is reactivated as of that day. Although 120 days is the default maximum stent placement period, the period can be modified at the discretion of each attending physician.
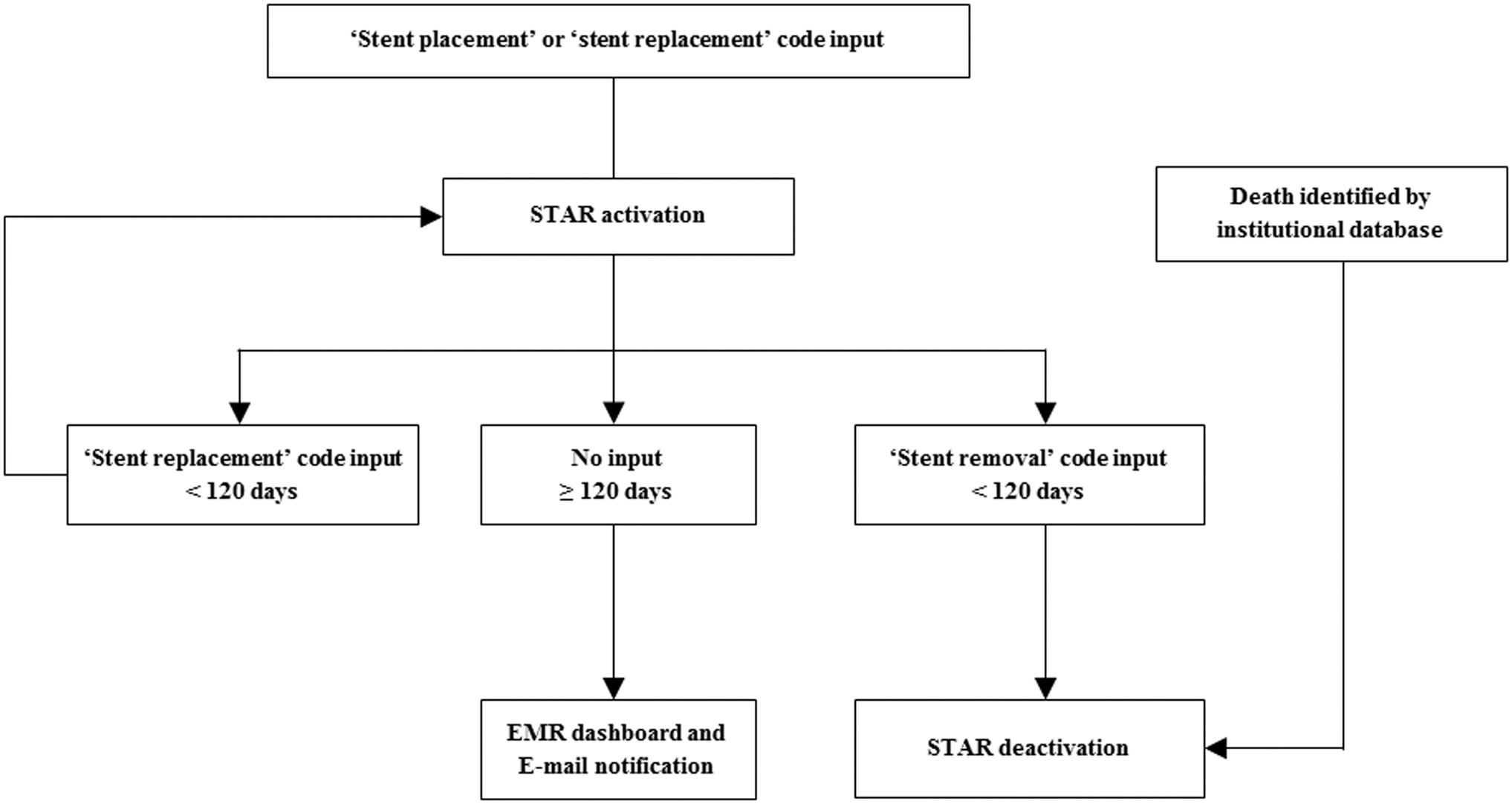
A flowchart of the algorithm implemented in the STAR. EMR = electronic medical record; STAR = Stent Tracking Algorithm Registry.
Validation of STAR
STAR was developed in September 2019. To evaluate the feasibility and validity of the system, a retrospective chart review was performed for 2194 consecutive patients who received primary ureteral stent placement or replacement at our institution between November 2006 and September 2019. Demographic variables included patient age, gender, stent laterality, survival status, indications for stent placement, and reasons why stents had been forgotten in patients identified by STAR. The definition of “identification” was the ability of STAR to identify patients with forgotten stents. Patient survival status was investigated based on the National Health Insurance Database or institutional medical records. This study was approved by our Institutional Ethics Committee (3-2019-0117).
Statistical analysis
The demographic characteristics of patients were compared using descriptive statistics. Appropriate comparative tests, such as the Mann–Whitney U test and the Fisher's exact test, were used to compare continuous and categorical variables. Statistical analyses were performed using SPSS version 18 (SPSS Inc., Chicago, IL). All tests were two-tailed, with statistical significance set at p < 0.05.
Results
Validation of STAR
Among 2194 patients who received primary ureteral stent placement or replacement, 354 (354/2194; 16.1%) patients were identified by STAR as harboring forgotten ureteral stents. The demographics of these patients are shown in Table 1. The most common indication for stent placement was hydronephrosis induced by malignancy.
Demographics of Patients Screened by the Stent Tracking Algorithm Registry
Data are presented as the median (interquartile range) and n (%).
A total of 57 (57/354; 16.1%) patients had been referred and were followed at another health care facility. These patients were contacted to confirm stent replacement or removal. A total of 124 (124/354; 35.0%) patients were identified because of the physician's omission of the “stent removal” code input to the billing system. Medical records for these patients were reviewed to confirm that the stents had been removed. All incidences were caused by stent removal as a secondary procedure, as in percutaneous nephrolithotomy, in which stent removal is a part of the surgical procedure. A total of 152 (152/354; 42.9%) patients had been lost to follow-up because of death, mostly from nonurologic malignancies. Nine (9/354; 2.6%) patients were out of contact, presumably because of cancer-associated death, since the last medical records indicated advanced-stage malignancies. The remaining 12 (12/354; 3.4%) patients were unaware of the stent existence (Table 2). The median period from stent placement to retrieval was 23.0 (interquartile range: 16.0–36.5) months. Two patients had their stents placed after diagnostic ureteroscopy, whereas 10 patients had their stents placed for nonurologic malignancies. These patients were contacted, and stents were retrieved through outpatient-based cystoscopy. Urinary tract infections were managed with short-term oral antibiotics without subsequent complications.
Reasons for Patients Screened by the Stent Tracking Algorithm Registry
Data are presented as n (%).
An effective stent tracking system should not only accurately identify patients who harbor forgotten stents, but also disregard patients devoid of forgotten stents. A notable finding was that among 1840 (1840/2194; 83.9%) disregarded patients, there were no cases in which STAR failed to identify patients whose stents were not removed or replaced at an appropriate time frame.
Our institution experienced three cases of medicolegal disputes related to forgotten stents within the retrospective study period. Of note, all three patients were identified by STAR, indicating that the disputes were avoidable if our system had been developed and applied earlier.
Application of the STAR to clinical practice
STAR has been integrated into our institution's EMR system as of October 2019 and is currently in use as of July 2020. Since December 2020, we have experienced five cases in which STAR prospectively identified patients with forgotten stents. All patients had been lost to follow-up after stent placement for nonurologic malignancies. Three patients were contacted, and the stents were replaced through outpatient-based cystoscopy. Two patients were lost to follow-up because of death. STAR can be integrated into any EMR system that utilizes coding algorithms.
Discussion
The attending physician is responsible for both the monitoring and removal of ureteral stents, and multiple levels of patient safety protocols should be implemented to prevent forgotten stents. The use of an automated electronic system appears to be an efficient solution with which to manage stent placement and removal, since patient education and counseling or manual tracking systems have proven to be inadequate in the prevention of forgotten stents. Monga and colleagues reported that 10% of patients with forgotten stents fail to show up for scheduled stent retrieval, despite being educated by physicians. 7 Manual systems are ineffective since they require teamwork for double-checking and paperwork, and loss of patient records and archiving are also areas of concern. We determined that the most useful strategy for identifying and tracking patients with stent placements would be to utilize EMR-based billing systems, in which every patient is mandatorily registered after the procedure. To our knowledge, STAR is the first automated ureteral stent tracking system that fulfills the ultimate endpoint of complete screening for forgotten stents.
Various methods using both manual and automated systems have been utilized to reduce the incidence of forgotten stents. In earlier years, ureteral stent logbooks and tracking cards were introduced for monitoring. 8 However, human error and negligence were fundamental reasons for the failure of these manual systems. In a 5-year retrospective follow-up of patients monitored with stent tracking cards, 5.9% of patients were unaccounted for and lost to follow-up. 9 Furthermore, remote access to the registry was not possible. Because of the lack of practical usage and the advent of EMR systems, these manual systems were replaced by computerized systems.
Computerized applications and electronic reminders appear to be reliable and efficient, and the utilization of automated algorithms has shown the potential to reduce the incidence of forgotten stents. McCahy and Ramsden introduced the first automated system to track ureteral stents in 1991, which reduced the incidence of overdue stent removals from 3.6% to 1.1%. 10 Ather and colleagues reported a decrease in the rate of forgotten stents from 12.5% to 1.2% for a period of 1 year after the implementation of an electronic tracking system. 11 However, because of the necessity of manual data input and additional cost, the systems mentioned earlier had few advantages over their paper-based predecessors.
The first stent extraction reminder facility was introduced by Lynch et al., utilizing a system that created a case in a patient's electronic chart when the stent was placed. The strength of this system is that it requires the entry of the maximum stent life for each patient, and the system automatically sends e-mail notices to medical personnel when the maximum period is reached. 12 However, this system still required manual input to the registry, and because of the low data entry rate, only 61% of stents were tracked and quantified. To certify complete capture of placed ureteral stents, Baumgarten and colleagues configured a billing-based system. 13 This system was based on the International Classification of Diseases procedure code, and ureteral stent insertions were automatically identified with an 85% accuracy rate. After the system detected a ureteral stent, a reminder letter was directed to the patient and uploaded to the EMR. However, because of the billing system-based algorithm, incorrect captures of patients with nonureteral stents and the loss of patients within the lag time between stent placement and the generation of notification were noted as limitations. Moreover, patients who have not completed paying their bills were unaccounted for, since the billing system required an account to be closed. 13 As a result, this system failed to identify 15% of patients receiving stent placements.
Recent advancements and widespread use of smartphones have led to the integration of mobile internet technology into stent tracking systems. Sancaktutar and colleagues developed a registry that tracks ureteral stents and sends a text message reminder to both the patient and physician. 14 In their study, patients who were notified by the reminder system had shorter delays to stent removal than patients who were not notified. However, the short-term follow-up and delay periods, which were less than the commonly accepted maximum stent life, precluded the efficacy of this system to screen forgotten stents adequately. Moreover, the system was not usable for patients who lacked mobile phones. 14 Molina and colleagues explored the use of smartphone applications to prevent forgotten stents. 15 One patient (0.5%) in that study was lost to follow-up. This system showed the highest efficiency for stent removal compared with previous systems, but still required manual entry and review and was inapplicable to patients who were unfamiliar with smartphone applications.
There are unique strengths of STAR that are worth mentioning. First is that it is fully automated and convenient, being based on institutional EMR systems, in which the need for manual entry using dedicated staff and the possibility of negligence are minimal. Overall, the human factor is the main limitation in the monitoring of placed stents, in which any measure of manual entry and review may lead to a future case of forgotten stents. Since billing codes are mandatorily entered after a stent procedure, STAR is capable of fully archiving and screening every stent that has been placed or replaced. Our validation study revealed that there were no cases in which STAR-screened patients whose stents were removed or replaced at an appropriate time frame. Second, STAR can recognize and monitor stents according to each laterality. The billing codes for ureteral stent placement, replacement, and removal are categorized according to each laterality. Therefore, the STAR can separately screen overdue schedules for patients and facilitate individual stent tracking plans for bilateral ureteral stents that have been placed or replaced at different time points. Third, the maximum stent life can be modified at each attending physician's discretion. Currently, there is no consensus on the maximum placement time to avoid complications. Studies have suggested that 48% of stents may become encrusted within 3 months after placement, and that replacement should be performed every 2–4 months. 16,17 At our institution, ureteral stent replacement is generally recommended every 3 months. The default stent life for STAR is set to 120 days, so as not to screen all patients with delayed removal or replacement schedules within 1 month. However, this default period can be modified according to each attending physician's discretion. Fourth, the overdue notification, including information about a specific patient, can be sent by two pathways for maximum efficacy. At login to the EMR system, the attending physician may review a dashboard list of patients screened by STAR through a pop-up window. Information regarding each patient, the date of last placement or replacement, and the attending physician are shown in Figure 2. The EMR of each patient can be directly assessed from the dashboard to see the reason why a specific patient was screened. Also, if preferred, the overdue notification can be sent to the attending physician's institutional e-mail. Finally, STAR can be integrated into any EMR system that utilizes coding algorithms.
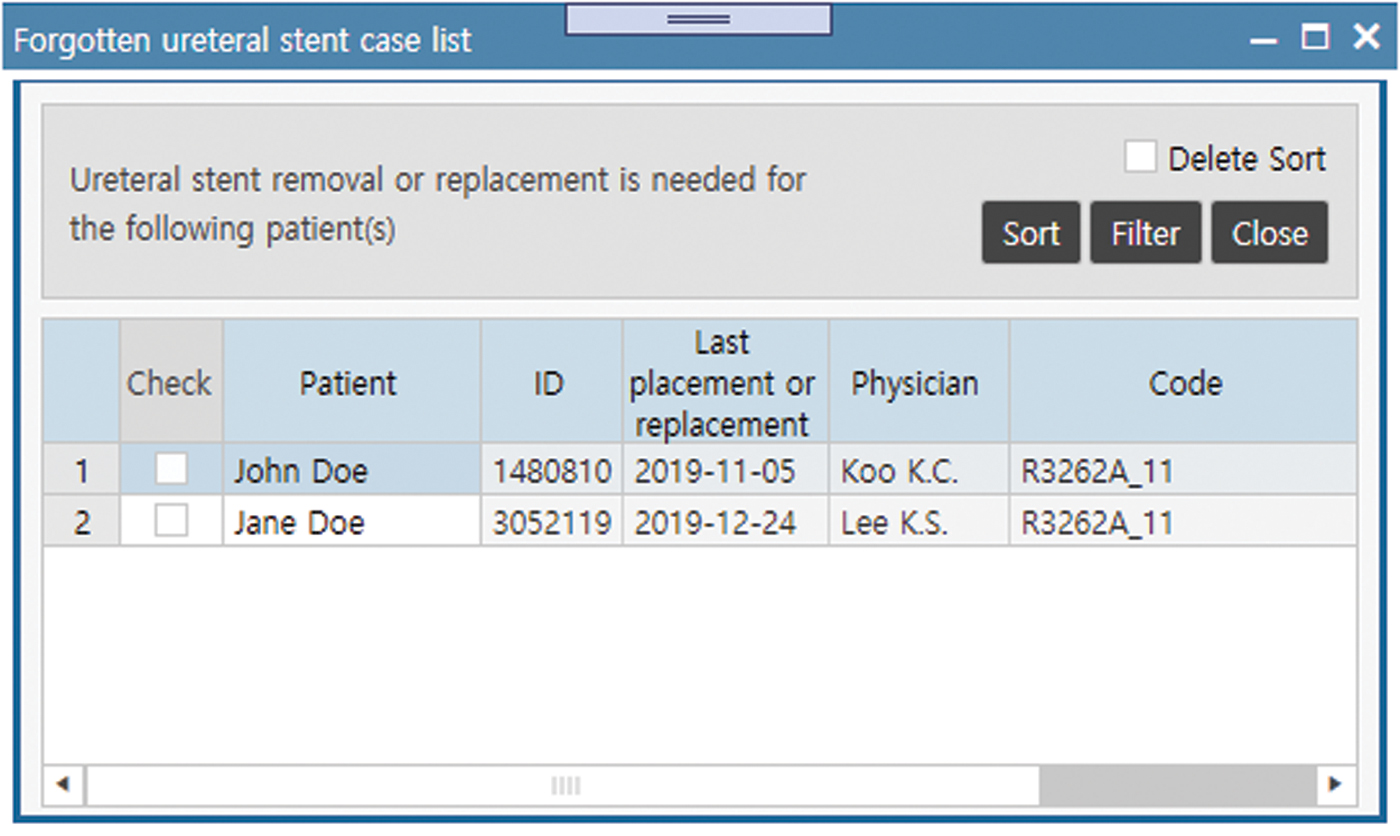
Snapshot of the pop-up window in the electronic medical record system, indicating patients identified by STAR. Color images are available online.
There are limitations to STAR that need to be overcome. As our results have shown, the algorithm cannot be automatically deactivated in patients lost to follow-up because of deaths outside of our institution and in those who are referred to another health care facility. However, we believe overscreening by the system and subsequent manual deactivation would better guarantee the prevention of forgotten stents. Nevertheless, updated versions of STAR could include integration with the National Health Insurance Database to capture documented deaths for automatic deactivation. Finally, a subset of patients without forgotten stents was identified because of the physician's omission of the “stent removal” code input to the billing system. To overcome this limitation, the algorithm may need to be linked to each specific stent that is placed for a certain patient.
Conclusions
STAR was developed and validated to offer a proficient means with which to enhance patient safety and to prevent medicolegal complications associated with forgotten ureteral stents. This system has the potential for widespread use since it can be integrated into any EMR system that utilizes coding algorithms. Our results indicate that reliable electronic tracking systems can be applied in any clinical field to guarantee safe patient follow-up.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a faculty research grant of Yonsei University College of Medicine (6-2019-0171).