
Abstract
Purpose:
To investigate the clinical value of contrast-enhanced ultrasound (CEUS) in percutaneous nephrolithotomy (PCNL) for kidney stone patients without hydronephrosis.
Methods:
Patients with nondilated collecting system kidney stones who underwent PCNL between October 2018 and December 2019 at our hospital were enrolled in this study. Patients who met the inclusion criteria were randomized into two groups: a CEUS-guided PCNL group and a conventional ultrasound (US)-guided PCNL group. The operation results of the two groups were compared, including the number of attempts for effective puncture, duration to effective puncture, stone clearance rate, blood loss, postoperative complications, and hospital stay.
Results:
Fifty-six patients with a nondilated collecting system who underwent PCNL for 60 kidneys were included in this study, including 4 patients who underwent bilateral PCNL due to bilateral renal stones. There were 30 kidneys in each group. All patients successfully underwent PCNL. The CEUS-guided PCNL group had more accurate punctures, with a higher effective rate of one puncture and shorter puncture time. There was no statistically significant difference in stone clearance rate between the two groups. Four cases of double channels were established in the conventional US-guided PCNL group, while there was only one case in the CEUS-guided PCNL group. In the CEUS-guided PCNL group, most cases (96.7%, 29/30) had no or only mild complications, which were significantly better than the conventional US-guided PCNL group (76.7%, 23/30). The mean postoperative hemoglobin loss in the CEUS-guided PCNL group was 9.5 (range 1–25) g/L, which was significantly lower than 15.5 (range 5–52) g/L in the conventional US-guided PCNL group.
Conclusion:
The CEUS technique can improve visibility of the nondilated renal collecting system, facilitate selection of suitable calix, and identify renal calix fornix. It also benefits needle placement in patients with a nondilated collecting system.
Introduction
Percutaneous nephrolithotomy (PCNL) is considered the preferred treatment for patients with large (>20 mm) renal stones and staghorn stones due to the high stone clearance rate and low complications. 1 However, PCNL still has serious complications, such as surrounding organ damage and bleeding, which can make this technique difficult, especially during the puncture process. 2 Therefore, accurate puncture is the most important step in PCNL operation. 3
The traditional puncture guidance method is typically fluoroscopy guidance. Although fluoroscopy guidance allows accurate identification of the expected calix for puncture, the two-dimensional fluoroscopy image cannot show the three-dimensional relationship between the kidney collection system and the stone, cannot distinguish anterior and posterior groups of calices, and cannot show the surrounding organs. In addition, fluoroscopy poses the risk of radiation, which may increase long-term incidence of malignancy in exposed patients. 4,5
Ultrasound (US)-guided PCNL was reported as early as 1979. 6 In recent years, US guidance has experienced increasing popularity and is widely used in China, Europe, and India. 7 Its merit include a lower cost; no radiation; convenience; real-time, multidirectional, and multiangle exploration of renal structure; observation of the relationship between stones and the renal collecting system; and observation of the vessels and peripheral organs between puncture paths. US-guided PCNL is reported to result in more accurate puncture and less radiation exposure than fluoroscopy-guided PCNL. 8 However, US-guided PCNL is technically more challenging because many urologists are not familiar with renal ultrasonography. As a result, this technique has a long learning curve. 3 For a nondilated renal collecting system, US-guided PCNL is more challenging because the expected calix for puncture can be difficult to visualize. Thus, enhancing visibility of the nondilated renal collecting system will facilitate PCNL performance. Contrast-enhanced ultrasound (CEUS) was first reported by Armstrong et al. in 1982. 9 Subsequently, this technique has become widely used for intracavitary administration, such as that in the biliary tract, fallopian tube, ureter, and so on, to improve visibility of physiologic body cavities. 10 –12 Studies have shown that use of this technique in PCNL can improve visibility of nondilated collecting systems and facilitate effective puncture. 13
In our hospital, we used CEUS to guide PCNL and compared the outcomes with those of conventional US. The primary aim of this study is to investigate the clinical value of CEUS-guided PCNL in the treatment of patients with a nondilated collecting system.
Patients and Methods
This was a prospective, randomized single-center clinical study completed at the Second People's Hospital of Yichang. From October 2018 to December 2019, patients with nondilated collecting system kidney stones who required PCNL surgery were enrolled in this study. Patients who met the criteria described below were randomized into two groups: a CEUS-guided PCNL group and a conventional US-guided PCNL group. The inclusion criteria were as follows: (1) age 18 to 80; (2) kidney stones ≥2.0 cm in diameter; (3) a nondilated collecting system (defined as a kidney having no caliceal dilatation at US [i.e., grade 0/1 renal appearance on the four-grade system used to classify the degree of hydronephrosis with maximum 2–3 mm caliceal separation 14,15 ]); and (4) written informed consent for CEUS, surgery, and participation in this trial. Patients with horseshoe kidney, polycystic kidney, pelvic kidney, urosepsis, severe infection, severe coagulopathy, or severe cardiopulmonary insufficiencies were excluded.
Before operation, blood analysis, urine analysis, urine culture, renal function assessment, and coagulation profile test were performed in all patients. Preoperative US examination was performed in all patients to determine the degree of hydronephrosis. All patients were preoperatively examined by CT urography (CTU). Stone location and size, as well as its relationship to the renal collecting system, were assessed by CTU before surgery. Stone size was measured by the maximal diameter on the preoperative CTU.
Preoperatively, all patients signed informed consent for CEUS and surgery, and demographic data were obtained. All operations were performed by an associate chief physician specializing in urologic calculi with 5 years of experience performing US-guided PCNL. Before starting this study, this physician completed five cases of CEUS-guided PCNL under the guidance of a sonographer and had mastered this technique.
CEUS-guided PCNL
The US contrast agent was sulfur hexafluoride microbubbles (SonoVue; Bracco, Switzerland). First, 5 mL of 0.9% sodium chloride solution was injected into a bottle of sulfur hexafluoride microbubbles. The bottle was shaken for 20 seconds to make a dispersion solution. Next, 1 to 2 mL of dissolved US contrast agent was extracted and injected into a 50 mL injection syringe containing 50 mL 0.9% sodium chloride solution, which completed preparation of the contrast agent. The remaining US contrast agent was retained for use.
After general anesthesia and prophylactic use of antibiotics, each patient was placed in the lithotomy position. An open-ended 5F ureteral catheter was placed retrograde into the ipsilateral proximal ureter as much as 25 cm under ureteroscope guidance. The patient was then placed in the prone position.
We used a Mindray US machine (Mindray OMT-500, Shenzhen, China) to guide PCNL. The ultrasonic probe was a convex abdominal transducer (Mindray C5-1S). First, the renal collecting system was observed under conventional US to confirm the general area where the calix was presumed to puncture, and the probe was fixed in the general puncture area. We then switched to CEUS mode and slowly retrogradely injected the US contrast agent through the preplaced ureteral catheter until we could see the US contrast agent rapidly fill the entire collection system (including the undilated calix) (Fig. 1). The target calix for puncture was confirmed in all patients in CEUS mode. Since the image quality of the kidney and its surrounding tissues and needle in B-mode were superior to that in CEUS mode, we monitored the entire puncture process in B-mode (Fig. 2). Under B-mode guidance, we inserted an 18-gauge needle (Huasheng Medical, Suzhou, China) into the target calix. We then removed the needle core until we could see the US contrast agent flowing out of the needle, which confirmed that the needle entered the collection system (Fig. 3, Supplementary Video S1). Next, we inserted a guidewire (Huasheng Medical) into the renal collection system. Depending on the size of the stone, the working channel was dilated in a stepwise manner to 16F to 18F using fascial dilators with the help of the guidewire. A 12F nephroscope (Wolf, Germany) was used to observe the renal collection system, and the stones were disintegrated by Holmium laser (Lumenis 60W, Germany). We used US to examine stone clearance. If the stone location could not be reached using the nephroscope, another working channel was established with assistance of the nephroscope and US. After second confirmation that no stones remained, a 6F to 7F Double-J stent (Cook Medical, Bloomington, IN) was placed into the ureter. At the end of the operation, a nephrostomy tube was placed.

After retrograde injection of ultrasound contrast agent, ultrasound contrast agent showed the whole renal collecting system; Arrow: upper calix.

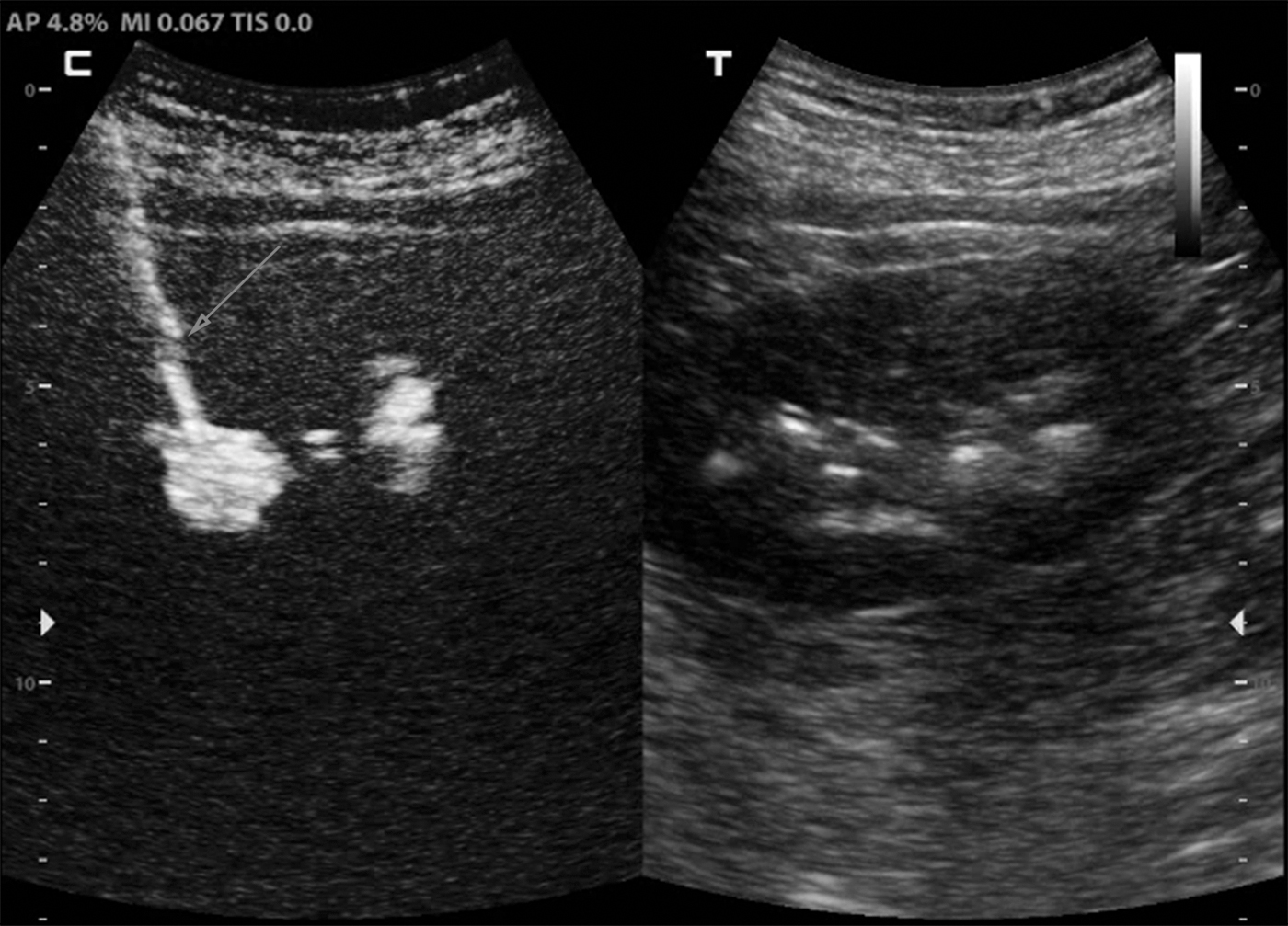
Since the image quality of needle in B-mode was superior to that in CEUS mode, we confirmed the target calix in CEUS mode and monitored the puncture process in conventional ultrasound mode; Arrow: needle. CEUS, contrast-enhanced ultrasound.
Needle entering the renal collection system is confirmed by the US contrast agent flowing out of the needle.
Conventional US-guided PCNL
The renal collecting system was dilated by retrograde injection of 0.9% sodium chloride solution. The target calix was identified, and the puncture process was monitored under conventional US. All other procedures were the same as for CEUS-guided PCNL.
Postoperative treatment
All patients underwent routine blood analysis on the first day after surgery to assess postoperative blood loss. Plain film of kidney, ureter, and bladder radiograph or CT was performed 3 to 5 days after surgery to determine whether there were any residual stones. In cases without residual stones, the nephrostomy tube was removed and the patient was discharged after 1 to 2 days of observation. The hospital stay was calculated from the day of surgery until the day of discharge. The Double-J stent was removed 1 month after surgery. All patients were followed up until the Double-J stent was removed. In patients with bilateral kidney stones, contralateral PCNL was performed 1 month after the first PCNL (Figs. 4 and 5).

A patient with bilateral partial staghorn stone with no renal calix dilation was treated with CEUS-guided PCNL. PCNL, percutaneous nephrolithotomy.

CT scan showed that the bilateral stones were completely cleared, and Double-J stent was placed in both ureters.
Data collection
All surgical data were recorded, including the number of attempts for effective puncture, the duration to effective puncture (defined as the time elapsed from observing the renal collection system until effective needle placement into the collecting system), operation time, number of percutaneous nephroscopic channels, hospital stay, blood loss, complications, and stone clearance rate. Stone clearance was defined as a residual stone burden ≤0.4 cm.
Statistical analyses
All statistical analyses were performed using SPSS 20.0 software. The normality of the data was tested using the Shapiro–Wilk test. Normal data are reported as the mean ± standard deviation, non-normal data are reported as the median and range, and categorical data are reported as frequencies and percentages. Data between the two patient groups were compared. The independent samples t-test was used to compare normal data, the Mann–Whitney U test was used to compare non-normal data, and the chi-square test was used to compare categorical data. p < 0.05 was considered statistically significant.
Results
Fifty-six patients who underwent PCNL for 60 kidneys with a nondilated collecting system were included in this study, including 4 patients who underwent bilateral PCNL due to bilateral renal stones. The CEUS-guided PCNL group and conventional US-guided PCNL group each contained 30 kidneys. Demographic and stone characteristics of the patients are presented in Table 1. As shown, the two groups did not significantly differ in terms of demographics or stone characteristics.
Demographic and Stone Characteristics of the Patients
CEUS = contrast-enhanced ultrasound; PCNL = percutaneous nephrolithotomy.
All patients successfully underwent PCNL. The CEUS-guided PCNL group showed quicker and more accurate puncture. The success rate of one puncture in the CEUS-guided PCNL group (80%, 24/30) was significantly higher than that in the conventional US-guided PCNL group (53.3%, 16/30). The duration to effective puncture in the CEUS-guided PCNL group (8.1 minutes, range 6.8–14.2) was significantly shorter than that in the conventional US-guided PCNL group (9.1 minutes, range 7.2–20.0). However, the difference in operation time between the two groups was not statistically significant (Table 2).
The Comparison of Intraoperative and Postoperative Data Between the Two Groups
The stone clearance rate in the CEUS-guided PCNL group was 86.7% (26/30), while that in the conventional US-guided PCNL group was 73.3% (22/30). A double channel was established in one case in the CEUS-guided PCNL group and in four cases in the conventional US-guided PCNL group. The average hospital stay of the CEUS-guided PCNL group (9 days, range 6–12) was shorter compared with the conventional US-guided PCNL group (10 days, range 7–23), and this difference was statistically significant. In the CEUS-guided PCNL group, the mean postoperative hemoglobin loss was 9.5 g/L (range 1–25), which was significantly lower compared with 15.5 g/L (range 5–52) in the conventional US-guided PCNL group (Table 2).
In the CEUS-guided PCNL group, four cases had residual stone, one case underwent second-look PCNL, and one case underwent extracorporeal shockwave lithotripsy. In the conventional US-guided PCNL group, eight cases had residual stone, three cases underwent second-look PCNL, and one case underwent flexible ureteroscopy (Table 2).
The modified Clavien grading system was used to evaluate postoperative complications. 16,17 If the patient had multiple complications, only the complication of the highest grade was analyzed. Further endourologic intervention for residual stone, such as second-look PCNL, ureteroscopy, or shockwave lithotripsy, was not considered a complication. Postoperative complications were significantly reduced in the CEUS-guided PCNL group. In the CEUS-guided PCNL group, most patients (96.7%, 29/30) had no or only mild complications (grade 1), which was significantly better than the conventional US-guided PCNL group (76.7%, 23/30). The most common grade 1 complications were fever requiring antipyretics and bleeding requiring increased bladder flushing. There were six and seven cases of grade 1 complications, respectively, in the CEUS-guided PCNL group and conventional US-guided PCNL group. One case of infection requiring additional antibiotics in the CEUS-guided PCNL group, as well as two cases of infection requiring additional antibiotics, and two cases of hemorrhage requiring blood transfusion in the conventional US-guided PCNL group were defined as grade 2 complications. In the conventional US-guided PCNL group, one case underwent super-selective renal arterial embolization due to serious hemorrhage, one case underwent bladder clot removal, and one case underwent thoracic close drainage due to hemothorax. These three cases were recorded as grade 3 complications. Notably, there were no grade 3 complications in the CEUS-guided PCNL group (Table 3).
The Comparison of Complications Between the Two Groups
Discussion
The higher success rate of puncture and fewer complications in the CEUS-guided PCNL compared with the conventional US-guided PCNL highlight the advantages of this method. CEUS is of practical value as a new technique to guide PCNL in patients without hydronephrosis.
At present, CEUS is widely used for intracavitary administration. Chi et al. 18 reported the use of CEUS to evaluate ureteral patency following PCNL, and the results were mostly concordant with fluoroscopic findings. Cui et al. 19 introduced CEUS for guiding percutaneous nephrostomy (PCN) and concluded that CEUS may become a new technology to affirm needle placement during PCN. Subsequently, Usawachintachit et al. 13 introduced CEUS to assist in percutaneous renal puncture in the nondilated collecting system, finding that this technique improved visualization of the collecting system and facilitated needle placement in patients without hydronephrosis. However, a control group guided by conventional US is required to confirm these findings.
Sulfur hexafluoride microbubbles have good stability and few adverse effects in intravascular injection. Compared with iodinated contrast, US contrast has some obvious advantages. It has a short half-life (5–7 minutes), and multiple injections can be given during one study. Moreover, the microbubbles can be destroyed in the case of incorrect placement, and so no distracting blob of US contrast agent is left to interfere with the procedure.
US-guided PCNL has become increasingly utilized. In patients without hydronephrosis, US-guided PCNL has always been a challenge since targeting a nondilated calix is difficult due to poor visualization and the absence of distention, which complicates placement of the needle into the renal calix. 15 The success rate of US-guided PCN is reported to be 96% to 100% in kidneys with a dilated collecting system, but decreases to 80% in kidneys with a nondilated collecting system. 20 Degirmenci et al. 16 reported success rates of 96.4% and 82.7% for primary insertion of US-guided PCN for dilated and nondilated systems, respectively. Multivariate analysis showed that only the nondilated collecting system was a significant parameter affecting complication rates and that the overall incidence of complications increased sixfold in patients with a nondilated system compared with patients with a dilated system. 16 Usawachintachit et al. 21 prospectively included 96 patients with US-guided PCNL and achieved a lower success rate of 71.9%, as two-thirds of patients had no hydronephrosis. Thus, the ideal patients for US guidance are thought to be those with hydronephrosis. 21
Improving the visibility of the nondilated system will improve the puncture success rate and reduce complications. Many surgeons dilate the renal collecting system by retrograde injection of physiologic saline. 22 Intravenous diuretic agents are also used to dilate the renal collecting system. However, a study by Yagci et al. 14 suggested that dilatation only lasts 15 minutes and rapidly decreases to baseline after 30 minutes, and so needle placement should be completed in the appropriate timeframe. Artificial renal pelvic distention also increases intrapelvic pressure to some extent. Persistent high pressure in the renal collecting system can lead to lymphatic reflux of the renal pelvis and potentially lead to systemic absorption of fluid containing bacteria or endotoxins, increasing the risk of fever and infection. 23 With retrograde injection of US contrast agent, the whole renal collecting system is filled with microbubbles and can be clearly displayed at a small dose. This process does not cause obvious collecting system over distention.
Our study showed a higher technical success rate and fewer complications in the CEUS-guided PCNL group. Retrograde US contrast injection can visualize the whole renal collecting system, which is similar to iodinated contrast images. The bright echoes of US contrast agent help to distinguish which calix is the most suitable for puncture. Among our patients, a double channel was established in one case in the CEUS-guided PCNL group and in four cases in the conventional US-guided PCNL group. We believe that first correct selection of the best calix for puncture can help to improve the stone clearance rate and avoid the establishment of double channels. In addition, the injection of US contrast agent is helpful for distinguishing the renal calix from peripelvic fat, which is beneficial for the identification of the renal calix fornix. This facilitates needle insertion from the renal calix fornix and improves the accuracy of puncture.
After effective puncture into the renal collecting system, we could clearly see the US contrast agent flowing into the needle. The angle between the needle and the axis of the calix to the calix neck was clearly observed to evaluate puncture quality before dilation.
Notably, retrograde injection of US contrast agent does not show renal cysts. Thus, CEUS provides a better method of distinguishing hydronephrosis from cysts. During the puncture process, CEUS can prevent the needle from entering a cyst.
Numerous clinical studies have demonstrated the safety of US contrast agent for intracavitary administration. In a large sample study, use of the second-generation US contrast agent SonoVue to diagnose vesicoureteral reflux resulted in no serious adverse events, and only a few minor incidents were reported. 12 In our study, none of the patients had any health problems associated with the use of US contrast agent.
There are several drawbacks to the use of US contrast in PCNL. First, since the image of the needle in B-mode is clearer than that in CEUS-mode, both B-mode and CEUS-mode should be turned on during the operation. We needed to identify the target calix in CEUS-mode and then monitor the puncture process in B-mode. Having only half of the images increases the challenge of observing the needle in B-mode. Given the experience of the surgeon performing the procedures in our study, this challenge did not have a significant impact on the puncture process. However, we do not know whether the use of CEUS by beginners is beneficial for the puncture process. To perform CEUS more successfully in PCNL, CEUS software needs to be improved so that the renal collecting system and needle can be clearly observed in one image. Alternatively, CEUS could be combined with a technology that can display the needle position, such as SonixGPS. 24 Second, retrograde US contrast injection may not be necessary for all patients. Conventional US-guided PCNL has been shown to be safe and easy to perform in patients with a dilated collecting system. 25 In addition, when the target calix was filled with stone, we could identify the target calix by the position of the stone. In this case, retrograde US contrast injection would not play a significant role.
There are several limitations of this study. First, as a single-center prospective clinical trial, the sample size was relatively small. A larger sample size may be required to demonstrate the clinical value of this technology. Second, patients were only followed up for 1 month after surgery. As a result, complications that require long-term follow-up, such as ureteral stricture, are not reported. Third, since the researchers were not blinded, bias may exist in the collection and analysis of clinical data. Finally, all procedures were performed by a surgeon specializing in urologic calculi experienced in percutaneous renal access in nondilated collecting systems. The clinical value of CEUS when used by less experienced surgeons is unclear.
To the best of our knowledge, this is the first study to prospectively compare CEUS with conventional US-guided PCNL in the nondilated collecting system. Our results support that CEUS can effectively improve puncture accuracy and reduce postoperative complications. CEUS may be a better approach for accurate puncture in PCNL in suitable patients.
Conclusions
During percutaneous renal puncture, retrograde US contrast injection can improve the visibility of the renal collecting system without hydronephrosis, facilitate selection of the suitable calix, and help identify the renal calix fornix. It also benefits needle placement in patients with a nondilated collecting system.
Ethical Statement
This study has been approved by our institutional review board (IRB) and has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Footnotes
Acknowledgment
All authors thank gao xiaozhan, chief physician of the department of ultrasound, for his guidance on contrast-enhanced ultrasound technology.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Video SV1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.