
Abstract
Objective:
The aim is to assess the effectiveness of a biodegradable antireflux ureteral stent with heparin coating in a comparative study (BraidStent®-H) in an animal model for the treatment of iatrogenic ureteral perforation.
Materials and Methods:
A total of 24 female pigs underwent initial endoscopic, nephrosonographic, and contrast fluoroscopy assessment of the urinary tract. Afterward, unilateral iatrogenic perforation in proximal ureter model was performed. Then the animals were randomly assigned to Group-I, in which a double-pigtail stent was placed for 6 weeks, or Group-II, in which a BraidStent-H a biodegradable heparin-coated stent was placed. Follow-up assessments were performed at 1 and 6 weeks and 5 months.
Results:
In terms of therapeutic effectiveness, complete resolution was observed in 95.8% of Group-I animals and 87.5% in Group-II. No animals in Group-II showed vesicoureteral reflux (VUR) during the study; statistical significance was observed at 1 and 6 weeks versus Group-I. All stents in Group-II degraded without producing obstructive fragments and allowed distal ureteral peristalsis. Heparin coating was not efficient to reduce asymptomatic bacteriuria between groups. Pathologic assessment did not show any significance in the global score, but did in the “fibrosis in muscular layer” parameter, at the ureteral perforation healing area; Group-II showed higher healing quality.
Conclusions:
The biodegradable intraureteral BraidStent®-H is highly effective for the minimally invasive treatment of ureteral perforation, since it displays controlled and predictable degradation, avoiding the development of VUR as well as irritation of the bladder trigone. Unfortunately, heparin coating was not effective in avoiding stent-associated bacteriuria.
Introduction
Iatrogenic ureteral perforation (IUP) is a rare complication that is primarily related to gynecologic, colorectal, or pelvic surgery. However, increased endoscopic procedures at the upper urinary tract have also led to an increase in primary intraoperative complications, such as bleeding, false passage, ureteral perforation, and avulsion. 1 Regardless of its etiology, the treatment of ureteral perforation depends on perforation size, delays in diagnosis, and the volume of periureteral urinary collection. 2 For mild and moderate intraoperatively diagnosed ureteral perforations, endourologic techniques can be used, in the most favorable cases ureteral stenting alone. 3
Unfortunately, stents are not free from side effects; they affect >88% of patients, with pain affecting ∼92.2%. 4 However, ureteral stents for IUP treatment have been proved effective. The main causes of stent-related symptoms are vesicoureteral reflux (VUR) and bladder irritation caused by the distal curl of the stent. 5 Nevertheless, medicine is far from achieving the ideal ureteral stent. A biodegradable ureteral stent (BUS) has not yet been fully realized in surgical settings; hence, contemporary stents must always be removed. 6
Therefore, the aim of this comparative study was to assess the effectiveness of a BraidStent®-H, a new heparin-coated, biodegradable, antireflux ureteral stent for treating IUP. In previous experimental studies, BraidStent® has shown a controlled, predictable biodegradation rate in the porcine model, but with high asymptomatic bacteriuria rate, up to 41%. 7 Therefore, in this study, we evaluated a heparin coating to reduce bacterial adhesion and improve the characteristics of this BUS in an IUP model. 8
Materials and Methods
Twenty-four healthy female pigs were used in this study. The experimental protocol was approved by the Institutional Ethics Committee for Animal Research (European Commission-specific legislation).
Phase I
IUP model and stenting: blood and urine samples were collected to assess blood and biochemical parameters and to confirm urine sterility. Bacteriuria was estimated in all study phases by counting colony-forming units (CFU/mL) in vesical urine. A positive bacteriuria result was considered when the count was >105 CFU/mL. All study animals were administered prophylactic enrofloxacin on the previous day and 2 days after each study phase. Afterward, ultrasonography was performed to assess the degree of upper collecting system dilatation. 9 Urothelial alterations at the ureteral orifice and bladder trigone were endoscopically assessed and categorized according to the validated UOScore, that is, UO0 to UO3; the higher the score, the greater the urothelial injury. 7 Simulated voiding cystourethrography (SVCUG) was performed to evaluate VUR at baseline, at 1 and 6 weeks, and at a final follow-up of 5 months. 7 To perform SVCUG, a Foley catheter was inserted into the urinary bladder and filled. To simulate micturition, the bladder was manually compressed until the pressure reached 50 cm H2O for 60 seconds. 7
Then, excretory urography was implemented to assess upper urinary tract morphology and to evaluate ureteral peristalsis under fluoroscopic control (waves per minute). Finally, the internal lumen of the right proximal ureter was measured using retrograde ureteropyelography.
The IUP model
This model was generated after visualizing the right ureteropelvic junction. A traumatic tip of the rigid guidewire was introduced through the working channel of the ureteroscope into the ureteral wall. The ureter was perforated, and the ureteroscope was pushed forward (semirigid Karl Storz® ureteroscope; 8/9.5 Charr, 43 cm long) until periureteral fat and retroperitoneal space were visualized. Model suitability was assessed by fluoroscopy and retroperitoneal contrast media extravasation. All lesions were classified according to the Post-Ureteroscopic Lesion Scale (PULS), which grades ureteral lesions after ureteroscopy. 10
Once the IUP model was generated, animals were randomly divided into two 12-animal groups. In Group-I, a 5F polymeric ureteral double pigtail stent was inserted during a 6-week period (Universa® Soft, 22 cm, Cook® Medical). In Group-II, a new self-retaining, antireflux, and biodegradable stent (BraidStent®-H) was inserted using the transurethral approach by sliding over a guide. BraidStent®-H is an intraureteral design: it has a proximal end with a 3 cm pigtail with an internal channel, a 9 cm long central section, a four-thread braided section, 3F in diameter, and a distal anchoring system with a rounded edge four-thread basket that is 2 cm long, and it is 36F when expanded. Two biodegradable copolymers of different degradation times were also used. This feature allowed the stent to remain in place for 3 to 6 weeks. The BraidStent®-H was designed to avoid passing through the ureterovesical junction (UVJ) to prevent bladder trigone irritation and VUR (Fig. 1). For BraidStent®-H, the ureteral healing area must be placed at the central section to avoid alterations due to proximal and distal anchoring systems, as occurs in conventional ureteral stents.

BraidStent®-H at the time of retrograde placement.
Heparin coating of the BraidStent®-H was performed using the dip coating technique. Stents were completely immersed in sodium heparin at a concentration of 5000 UI/mL and dried for 2 hours at 60°C. After this, each stent had a homogeneous 70 μm heparin coating. In our in vitro studies (heparin enzyme-linked immunosorbent assay) and microscopy studies, we observed that the heparin coating remained for 48 to 96 hours after BraidStent®-H urine immersion (Fig. 2).
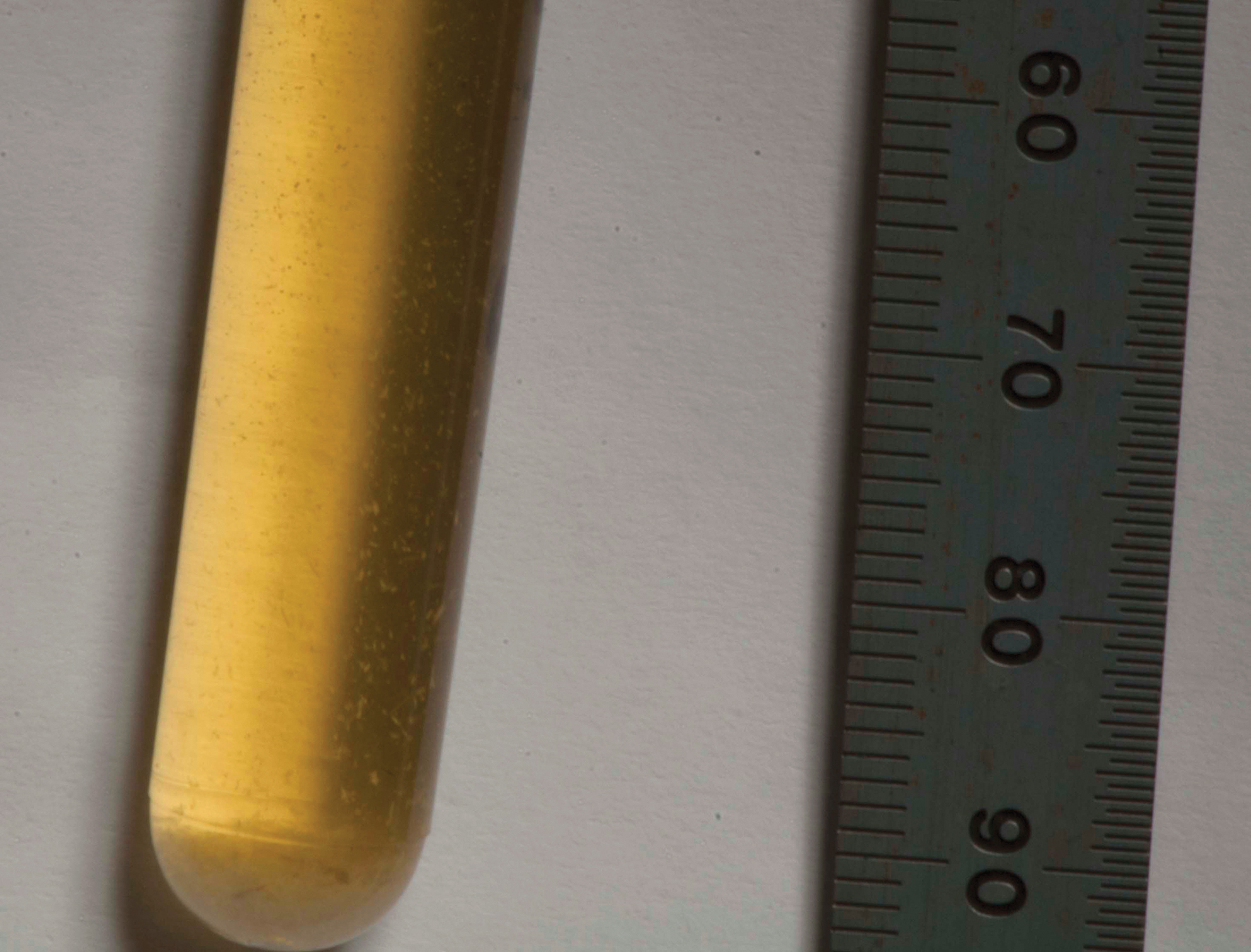
In vitro study in urine to assessment heparin release and stent degradation. BraidStent-H small fragments after 6 weeks. Color images are available online.
Phase II and III
Follow-up at 1 and 6 weeks: Phase III coincided with the removal of the ureteral stent in Group-I. The same diagnostic techniques used in Phase I were replicated at both follow-up times (Table 1). The assessment of bladder urine by optical microscopy allows for characterization of BraidStent®-H fragments.
Results Summary
p < 0.005.
PULS = Post-Ureteroscopic Lesion Scale; VUR = vesicoureteral reflux.
Phase IV
End-of-study assessment: the final follow-up was performed at 5 months and included ultrasonography, cystoscopy, ureteroscopy, and contrast fluoroscopy assessment. The experimental study element was completed by removing the urinary tract en bloc for pathologic study. Histologic slices were generated from the proximal ureter, the ureteral segment where the distal end of BraidStent®-H was placed, and ureteral orifices/bladder trigone. A validated healing score was used (0–3); the higher the score the greater the histologic damage to the ureteral or bladder wall 7 (Table 2).
Histologic Score
UVJ = ureterovesical junction.
Statistical analysis
To determine the sample size, a hypothesis contrast was performed, and a total of 12 animals per group were obtained (0.05 level of significance and statistical power of 90%). Quantitative variables are expressed as the mean ± standard deviation, and the normality study of these variables was carried out using the Shapiro-Wilk test. Variables that fit a normal distribution were compared using the Student's t-test for independent samples, while hypothesis testing between nonparametric variables was performed using the Mann–Whitney U-test. The evolution of quantitative variables throughout the phases of the study was evaluated by means of analysis of variance with repeated measurements. Categorical variables are expressed as percentages, and their comparison between groups was made by means of the chi-square test or the Fisher's exact test. The relationship between the categorical variables of the different phases was analyzed using the McNemar test.
Results
Phase I
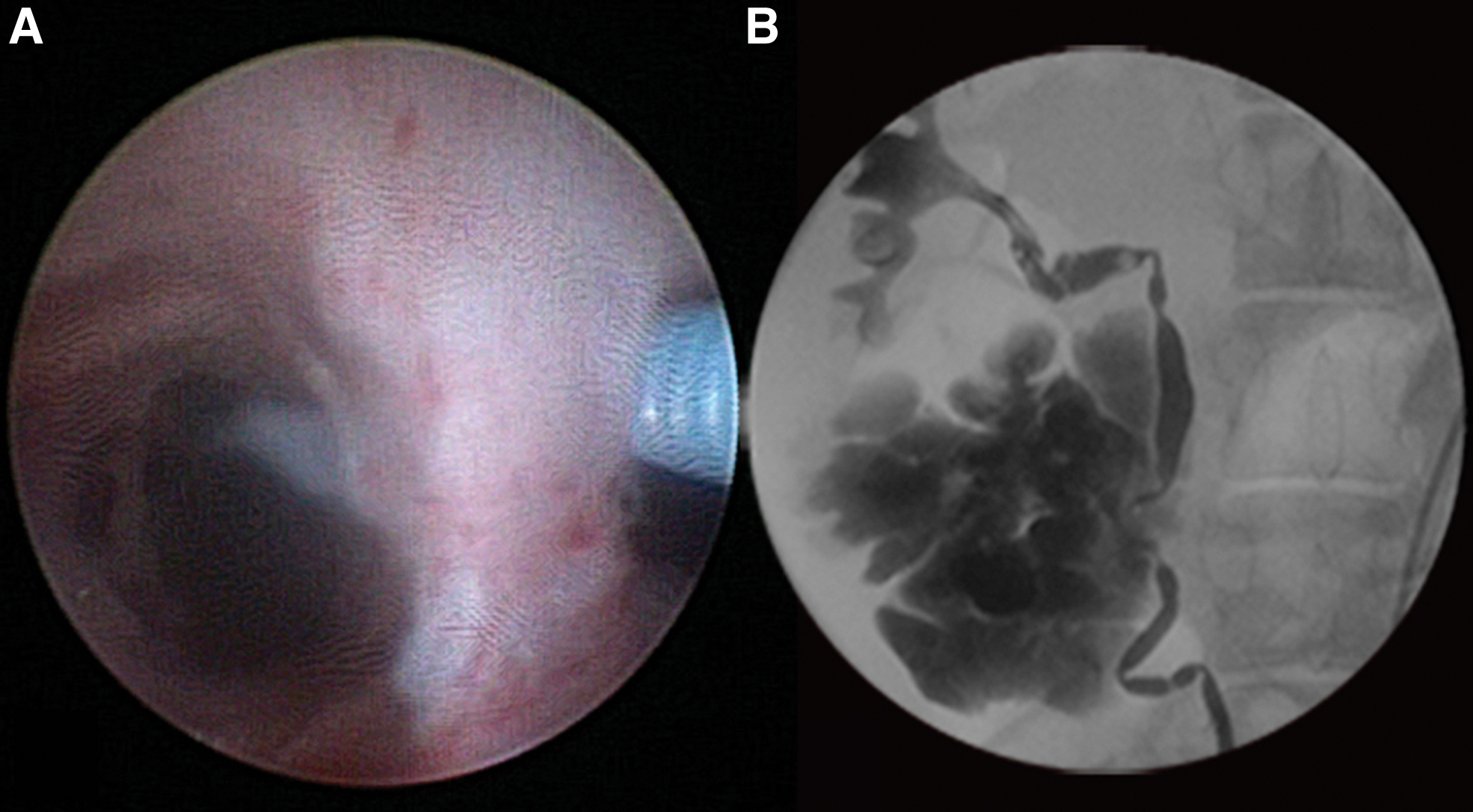
None of the animals showed alterations or bacteriuria in the urinary tract. The proximal ureteral perforation model was effectively performed and confirmed by contrast media extravasation in all animals (Fig. 3). PULS classification did not reveal any statistical significance between groups, and a PULS degree of 3 was observed in 71% of animals. Accidental perforation of the renal capsule and parenchyma occurred at the lower pole in one animal, with no pyelocaliceal system damage. No complications arose during stent placement in both groups (Table 1).
Phase II
Using ultrasonography, perirenal fluid collection was observed in one animal from Group-I and three from Group-II. Ultrasound-guided percutaneous drainage was performed in one animal from Group II due to a large urinoma. Infected urine was confirmed. A small polypoid nonobstructive ureteral growth was observed in most animals from Group-II at the BraidStent®-H distal end when assessed by ureteroscopy. No Group-II stents had commenced macroscopic degradation, and their mechanical properties remained intact. In terms of preserving ureteral peristalsis, suppression of peristalsis was observed in all Group-I animals, and 50% of animals in Group-II kept distal ureter peristalsis, with statistical significance between groups. We also observed significant evolution of macroscopic tissue damage at the ureteral orifice and bladder trigone between groups, that is, increased lesions were observed in Group-I.
Phase III
Urothelial growth related to the distal end of the BraidStent®-H disappeared in all animals. Perirenal extravasation was not present in either group, and the large urinoma was completely resorbed. We observed no BraidStent®-H debris at the ureteral level; although multiple stent degradation nonobstructive small fragments were observed in the bladder, leading to cloudy urine. BUS fragments were assessed by optical microscopy. Asymptomatic bacteriuria rates between groups were not statistically significant; however, there was significance versus the previous phase within each group (Table 1).
Phase IV
The final follow-up revealed a statistical significance between groups in terms of the internal ureteral diameter at the IUP area versus basal data, thus proving a suitable healing scar contracture. All study animals recovered peristalsis throughout the ureter. Periureteral fibrosis was observed in two animals from Group-II and one from Group-I. This fibrosis fixed the proximal ureter at the retroperitoneal area where the IUP model was performed. The PULS degree and periureteral fibrosis appeared as independent variables, and we observed no relationship between PULS values and periureteral fibrosis. Significant differences in “muscular layer fibrosis” parameters were observed between groups after pathologic assessment of the proximal ureteral wall. Group-I showed greater tissue damage in this area. At the bladder trigone, we observed significant differences in urothelial wall inflammation, lamina propria fibrosis, and muscular layer fibrosis, with Group-I showing the greater damage (Table 2). No BraidStent®-H fragments were embedded in the ureteral wall or in the retroperitoneum, or granulomas associated with foreign bodies were in Group-II.
Finally, the effective rate of each group was estimated after assessment of nephrosonographic recovery, proximal ureteral internal diameter, urinoma, and retroperitoneal fibrosis absence. These effective rates were 95.8% and 87.5% for Groups-I and II, respectively, with no significance. Also, we observed no statistical significance between the PULS degree and the effectiveness of the technique or between the effectiveness and periureteral fibrosis at the end of the study.
Discussion
Ureteral perforation with traumatic or nontraumatic etiology is a rare lesion, but it is a severe complication, especially if diagnosis is delayed. 11 Ureteroscopy is one of the most common causes of iatrogenic ureteric trauma and is mainly associated with lithiasis treatment. Currently, ureteral perforation rate is 1.05% according to a recent CROES study. 12 EAU urologic trauma guidelines recommend immediate stent placement or urinary diversion for partial perforations. 13 Ureteral stenting with or without dilatation is also a good option for intraoperatively nondiagnosed ureteral lesions. 13 The ideal stenting duration is not known; however, Schoenthaler et al. established a range of 2 to 4 weeks and 3 to 6 weeks, respectively, whether the ureteral transection was larger or smaller than 50% of the ureter circumference. 10 Traxer et al. recommended that stents remain in situ for 3 to 6 weeks to ensure healing of the ureteral wall. 14
Unfortunately, ureteral stents are not free of complications and they are associated with the loss of quality of life in a high percentage of patients. 4 An obvious improvement in the present double-J ureteral stent design should be to reduce patient morbidity and to include biodegradation capability. BUS not only avoids a second removal surgery, thus reducing health costs, but it also prevents forgotten stent syndrome. 15 In this study, we assessed BraidStent®-H in our animal iatrogenic ureteral model. Apart from being biodegradable, this new design avoids morbidity traits associated with current ureteral stents, VUR, and stents in bladder trigone since the design is strictly intraureteral. 5 Our study confirmed statistically significant differences in macroscopic damage at bladder trigone and VUR between groups. Furthermore, pathologic assessment of UVJ-bladder trigone wall thickness revealed significant differences between groups; Group-I showed greater damage. Two recent clinical studies assessing intraureteral stents showed that they were associated with less pain and discomfort in patients when compared to standard stents. Thus, strictly intraureteral BraidStent®-H may show the same qualities in patients. 16,17
The BUS assessed was as effective as current ureteral stents for treating early diagnosed ureteral perforation. In three animals of Group-II, we found the appearance of urinoma, versus a single animal in Group-I. This potential weakness in efficacy between both groups is reflected in the overall effective rate, which was 95.8% and 87.5% for Groups-I and II, respectively, without statistical significance.
BraidStent®-H did not show evidence of any differences throughout the study versus the conventional ureteral stent regarding the dilatation degree of the upper urinary tract or the dilatation ability of the ureteral lumen at the iatrogenic area in the long term, after ureteral wall healing. Both groups show a significant increase in proximal ureteral internal diameter due to ureteral remodeling healing caused to healing by second intention and the intubation effect by means of ureteral stents. However, we observed significance when assessing “muscular layer fibrosis”; although there was no significance in proximal ureter histologic global scores between groups. This meant a reduced healing quality of muscular layers in Group I. We also observed statistical significance regarding maintaining peristalsis in the distal ureter between 1 and 6 weeks: 50% to 66.6% of animals in Group-II maintained peristalsis when compared with 0% to 16.6% animals in Group-I. Maintaining distal ureteral peristalsis reduces ureteral spasm, which is related to pain and is one of the causes of alpha 1-adrenoreceptor antagonist administration in stented patients. 18,19 Therefore, while awaiting future clinical studies, this leads us to believe that the use of these drugs could be avoided with strictly intraureteral stents such as BraidStent®. Since this stent design allows distal ureteral peristalsis and has no lower urinary tract symptoms associated with the bladder end of the stent, it makes relaxation of the ureteral and bladder trigone smooth muscle unnecessary.
On the contrary, the BraidStent®-H design ensures controlled and predictable biodegradation. This was due to two characteristics: its braided compositional design and the polymer/copolymer combination with different degradation rates. This design generated nonobstructive fragments, and it maintained its internal scaffolding until polymer hydrolysis, with the slowest degradation rate. These characteristics facilitated longer stenting times when compared to other BUS experimental studies. 20 Equally, BraidStent®-H also avoided large fragment dispersal, such as those observed by Jin et al. in their assessment of new gradient BUS. 21
Heparin has been used for ureteral stent coating and the prevention of bacterial adhesion and incrustation, with encouraging results. 8,22 Therefore, we coated the BraidStent® since it showed high asymptomatic bacteriuria rates in a previous study. 7 However, like other authors, we did not observe a significant reduction in urine contamination. 23 BraidStent®-H is designed so that heparin disappears in the urine in the first 48 to 96 hours; therefore, it does not affect stent degradation rates since heparin reduces the stent bacterial contamination that sometimes occurs due to bacteria entering at the time of ureteral placement by transurethral routes. 24 Nevertheless, the results were unsatisfactory since asymptomatic bacteriuria values of >30% rarely appear in contemporary clinical studies. 24,25 To understand these results, when evaluating any BUS, expelled stent fragments carry biofilm matrix on their surface. Consequently, the breakdown of the biofilm matrix allows the release of planktonic bacteria in urine, which potentially provide a source of increased bacteriuria in the laboratory.
Our study was limited by the use of an animal model, and, equally, it was not possible to gain insights into patient quality of life. In addition, instead of voiding cystourethrography, SVCUG was used to assess VUR. We cannot rule out that the nonobstructive urothelial hyperplasia growth appearing at the BraidStent-H distal end 1 week after placement and disappearing at 6 weeks caused acute renal colic between those two follow-ups. Similarly, it is difficult to state whether pH changes or ingested liquid quantities could modify BraidStent®-H degradation rates since the animals followed a controlled diet. One clear limitation of this stent design is that it is not suitable for lower ureter injuries.
Conclusions
The biodegradable intraureteral BraidStent®-H is highly effective for the minimally invasive treatment of ureteral perforation, since it displays controlled and predictable degradation and avoiding the development of VUR as well as irritation of the bladder trigone. Unfortunately, heparin coating was ineffective in avoiding stent-associated bacteriuria.
Footnotes
Acknowledgments
Special gratefulness to Fernanda Carrizosa for her generous support during the writing of this article and Paula Martín Rodríguez and María Pérez Vela for the BraidStent® illustrations.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study has been funded by Instituto de Salud Carlos III through the projects “PI13/02417” and “PI16/01707” (Cofunded by European Regional Development Fund “A way to make Europe”).