Abstract

H
More than 80% of people infected with COVID-19 infection are asymptomatic and could present to the urologists for complaints of urinary stone disease, prostatic enlargement, or tumors. Anesthetists, operation theater nurses, and surgeons can be exposed to the virus during surgical procedures that need intubation in such asymptomatic patients. Percutaneous nephrolithotomy (PCNL) is one such procedure that needs intubation, change in position from supine to prone for puncture, and again change in position for extubation. This process may lead to spread of the virus through air.
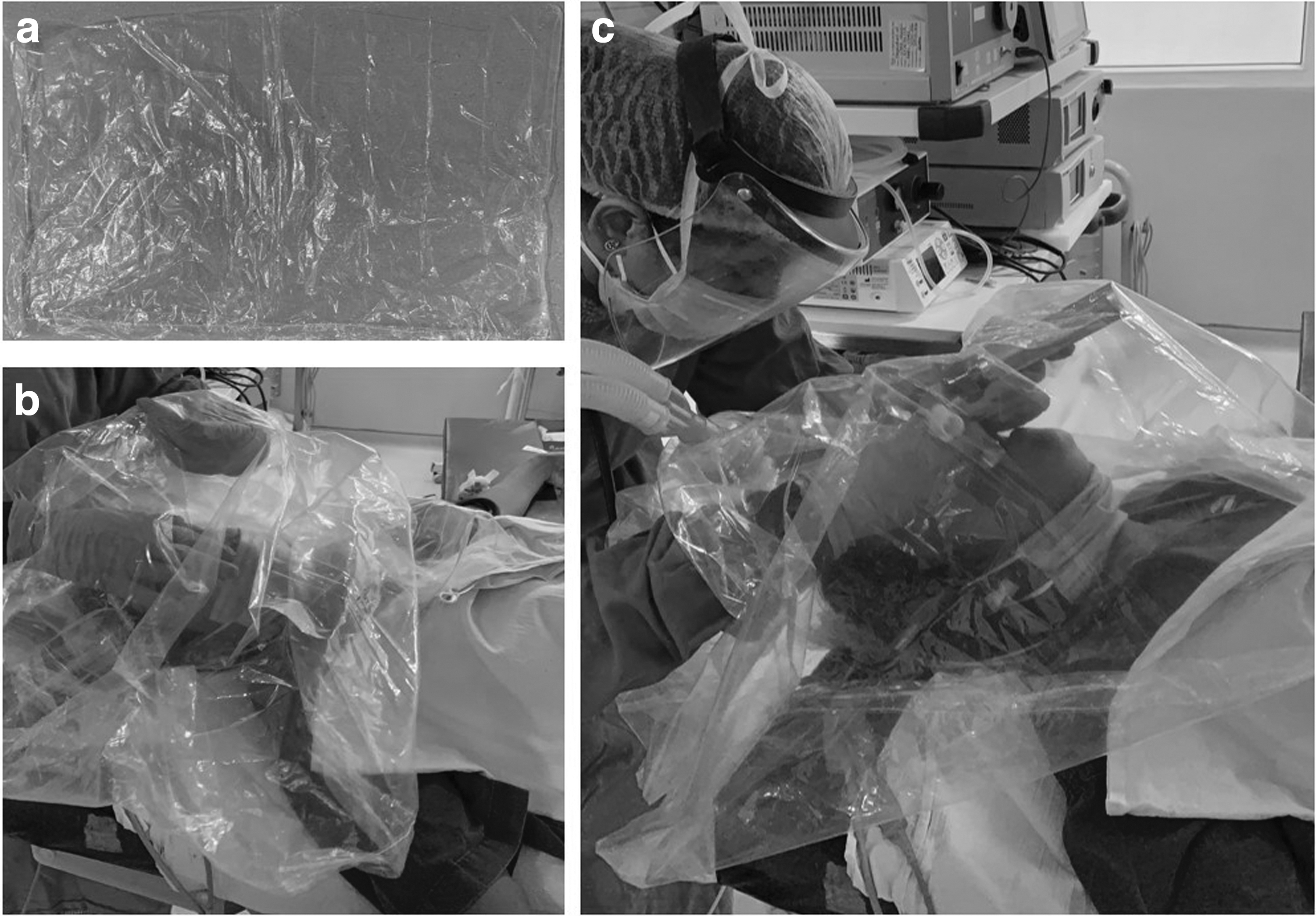
The sterile plastic drape used to cover the C-arm during the PCNL procedure was modified by our team to create a protective device (Fig. 1). Three small apertures were made at the midportion of the drape. Two of these apertures were used by the anesthetist to introduce his arms into the drape and the third one was used to guide the ventilator circuit. Adhesives were used to seal the apertures and make it leak proof. The drape was passed around the patients head and spread across the head end of the table. The laryngoscope, facemask, and the endotracheal tube were placed within the drape. After induction of anesthesia, the intubation procedure was performed, by observing the patient's airway through the transparent drape. The drape surrounded the patient's head and the tube, thus preventing spread of air droplets and aerosol contamination. The other end of the drape was tightened around the patient's neck. At the end of the procedure, the extubation process was carried out similarly within the two layers of the drape. This simple procedure using a sterile C-arm covering drape is cost-effective, safe, and efficient.