
Abstract
Introduction:
To compare surgical, oncologic, functional outcomes and complication rate between intracorporeal neobladder (ICNB) and extracorporeal neobladder (ECNB) orthotopic ileal neobladder of robot-assisted radical cystectomy (RARC) in patients with nonmetastatic bladder carcinoma (BC).
Materials and Methods:
From 2014 to 2019, we prospectively collected and retrospectively analyzed 101 patients with nonmetastatic BC treated with RARC and ortothopic neobladder. Chi-squared test estimated differences in proportions of functional and oncologic outcomes. Multivariable logistic regression models (MLRMs) focused on overall, early (<30 days from discharge), and late complication rate (>30 days from discharge) in ICNB vs ECNB.
Results:
Of all patients, 57 (56.4%) ICNB and 44 (43.6%) ECNB patients were identified. At least one complication occurred in 75.4% vs 72.7% in ICNB vs ECNB, respectively (p = 0.9). In MLRMs, focusing on complication rate, there was no statistically significant difference between ICNB vs ECNB for overall (p = 0.8), early (p = 0.6), and late complications (p = 0.8). No statistically significant differences were recorded for tumor relapse rate, cancer-specific and other cause mortality. No positive surgical margins were recorded in both groups. Daytime and nighttime continence recovery were 89.4% vs 87.1% (p = 1.0) and 63.8% vs 51.6% (p = 1.0) for ICNB vs ECNB. Potency recovery was 59.1% vs 54.3% (p = 0.5) for ICNB vs ECNB.
Conclusions:
No statistically significant differences in complication rate (overall, early, or late) were identified, when ICNB and ECNB were compared. Similarly, no statistically significant difference was found in oncologic and functional outcomes.
Introduction
Recently, large interest on robot-assisted radical cystectomy (RARC) has risen from the urologic community. As a result, the rate of RARC has increased in the past decades. 1 Several studies compared intracorporeal urinary diversion (ICUD) and extracorporeal urinary diversion (ECUD). 2 –4 However, in those studies most of patients received an ileal conduit diversion after RARC and no specific analyses regarding neobladder reconfiguration were conducted. In consequence, contemporary literature recognizes a need to address whether an intracorporeal approach for neobladder reconfiguration offers advantages over extracorporeal approach.
There is also lack of studies comparing ICUD vs ECUD at RARC regarding continence and potency recovery. In particular, for both continence and potency recovery, most of the results reported in literature are retrieved from studies where only intracorporeal neobladder (ICNB) was performed. 5 –11 In consequence, contemporary literature recognizes a need to address whether an intracorporeal approach for neobladder reconfiguration offers advantages over extracorporeal approach also for continence and potency recovery.
To address these unmet needs, we investigated surgical and functional outcomes, and complication rate of patient with nonmetastatic bladder carcinoma (BC) treated with RARC and either ICNB or extracorporeal neobladder (ECNB) at our Institution (2014–2019). We hypothesized a difference in surgical outcomes, such as operative time, blood loss, hospitalization length, and catheter indwelling, when ICNB and ECNB at RARC were compared. Similarly, we postulated a difference in overall, early, and late complication rate, and in functional outcomes.
Materials and Methods
Definition of population and variables for analyses
From January 2014 to July 2019 we prospectively collected and retrospectively analyzed 101 patients with nonmetastatic BC treated with RARC and ortothopic ileal neobladder reconfiguration. Orthotopic neobladder shape was configured according to surgeon choice. Following our open radical cystectomy (ORC) experience, most ECNBs were configured according the Hautmann's technique 12 or according to the Vescica Ileale Padovana shape. 6 Regarding ICNB patients, most neobladders were configured according to the Vescica Ileale Padovana 6 or according to a modified Pyramid shape. 13
Main variable of interest consisted of urinary diversion: ICNB vs ECNB reconfiguration. Preoperative descriptive covariates consisted of age, body mass index (BMI), year of procedure interval (2014–2016 vs 2017–2019), clinical T-stage (Ta-Tis-T1 vs T2), and neoadjuvant chemotherapy status (administered vs not administered). Intraoperative covariates consisted of operative time (minutes), number of removed nodes, estimated blood loss (EBL), and intraoperative transfusion rate.
Oncologic outcomes consisted of pT stage (T0, Ta-Tis-T1, T2, T3 or T4), pN stage (not nodal involvement vs nodal involvement), positive surgical margins (PSMs), and tumor relapse status. Functional outcomes consisted of continence (defined as number of daily pads used 0–1 vs >1) and potency (defined as an erection adequate to have sexual intercourse; erectile dysfunction [ED], not ED, or not ED with phosphodiesterase 5-inhibitor [PDE5i]) recovery. Postoperative covariates consisted of length of hospital stay (LOS) and days of bladder catheter indwelling (≤14 days or >14 days).
Main outcomes of interest consisted of overall, early (<30 days from discharge), and late complication (>30 days from discharge) rate. Within complications, we examined overall complications and specific complication subgroups. All complications were also classified according to the Clavien–Dindo complication scale. 14 All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Statistical analyses
First, estimated annual percentage change (EAPC) for neobladder reconfiguration at RARC, relative to open procedure, was tested with the least-squares linear regression.
Second, we analyzed the rates of ICNB and ECNB at RARC and tested for possible differences in pre-, intra-, and postoperative outcomes between the two groups. In this step, chi-squared, Wilcoxon, or Mann–Whitney tests estimated difference in proportions or medians.
Third, we tested the effect of neobladder reconfiguration (ICNB vs ECNB) on overall, early, and late complication rates. Specifically, multivariable logistic regression models (MLRMs), adjusted for year of operation, age, BMI, EBL, and operative time focused on overall complication rate in ICNB vs ECNB. Moreover, MLRMs adjusted for year of operation, age, and BMI focused on early (<30 days from discharge) and late complication rate (>30 days from discharge) in ICNB vs ECNB. All statistical tests were two-sided with a level of significance set at p < 0.05. Analyses were performed using the R software environment (version 3.4.1) for statistical computing and graphics.
Results
Preoperative and intraoperative characteristics of the study population
Annual rates of RARC with neobladder reconfiguration (45.2%–85.7%; EAPC: +15.3%, 95% confidence interval = 9.7–21.5, p < 0.01) sharply increased over the study span, relative to open procedure (Fig. 1).
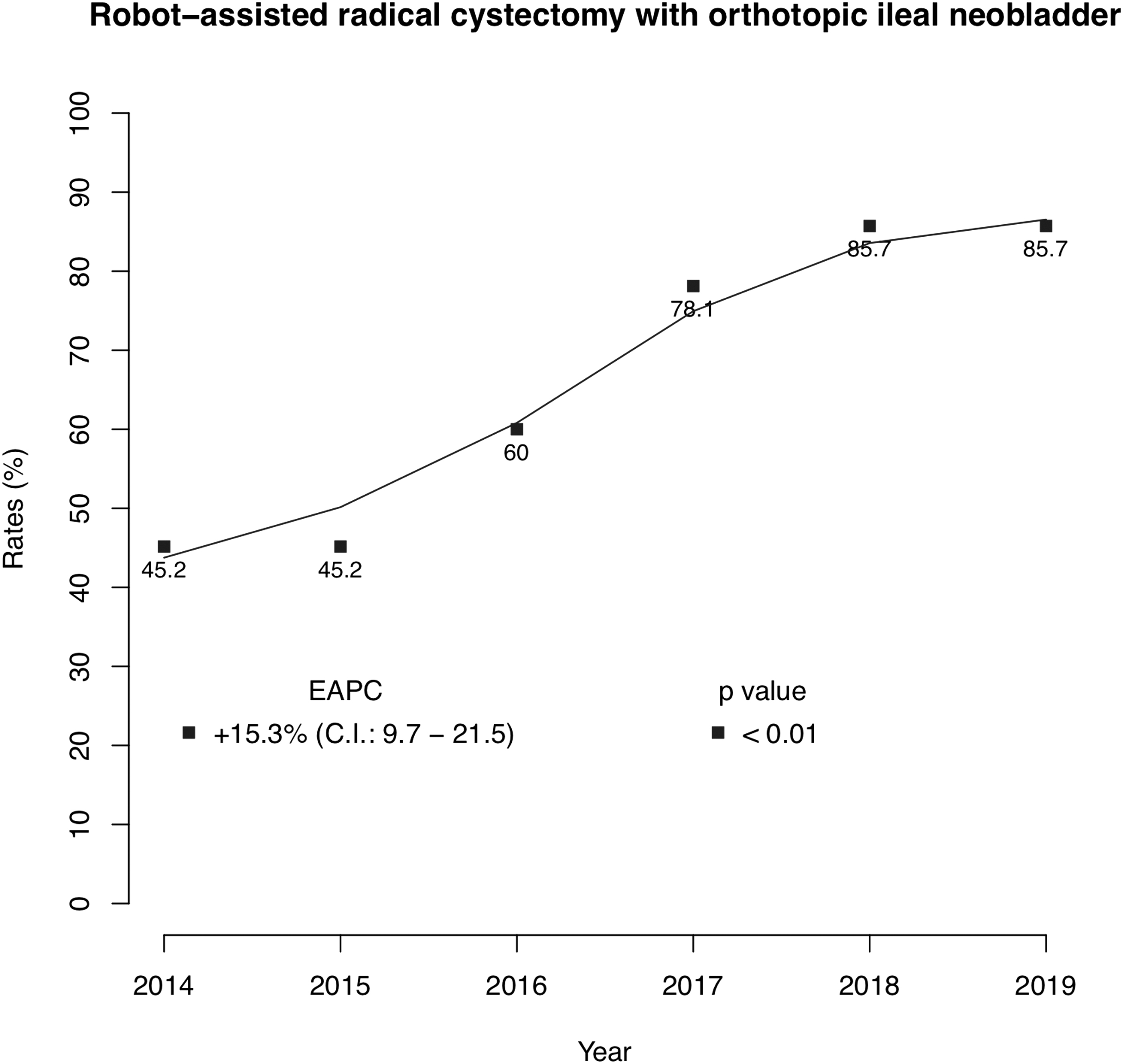
Trend of annual rate change of robot-assisted radical cystectomy with orthotopic ileal neobladder reconfiguration.
Of 101 RARC with neobladder reconfiguration, 57 (56.4%) ICNB and 44 (43.6%) ECNB patients were identified. Most ICNB were performed more contemporary (80.3% vs 27.3%; p < 0.01), relative to ECNB (Table 1). No preoperative differences between ICNB vs ECNB were identified for median age (60 vs 62 years; p = 0.2), BMI (26.9 vs 26.6; p = 0.9), and estimated glomerular filtration rate ([EGFR] 90.3 vs 84.6; p = 0.7). Similarly, no statistically significant difference was identified for clinical T stage (p = 0.1). Conversely, higher rate of neoadjuvant chemotherapy was recorded in ICNB group (49.1% vs 20.5%; p < 0.01).
Pre- and Intraoperative Outcomes of 101 Patients with Nonmetastatic Bladder Cancer Treated with Robot-Assisted Radical Cystectomy, Stratified According Ileal Ortothopic Neobladder Reconstruction: Intracorporeal vs Extracorporeal
CHT = chemotherapy; ECNB = extracorporeal neobladder; ICNB = intracorporeal neobladder; IQR = interquartile range.
Longer median operative time was recorded in ICNB group (520 vs 455 minutes; p = 0.02), whereas no statistically significant difference was recorded for median EBL (400 vs 500 mL; p = 0.9) and for intraoperative transfusion rate (1.8% vs 11.4%; p = 0.1). A higher rate of median lymph nodes yield was identified in ICNB group (25 vs 18; p < 0.01).
Postoperative outcomes and complication rate
Similar median LOS was recorded in both groups (11 vs 12 days for ICNB and ECNB, respectively; p = 0.5; Table 2). In both ICNB and ECNB groups, higher rate of patients with a bladder catheter indwelling shorter or equal to 14 days was recorded (75.4% vs 72.7%; p = 0.9), relative to those who removed bladder catheter after the 14th postoperative day. Similar median EGFR after 3 months was recorded in both groups (69.0 vs 70.5; p = 0.3).
Postoperative Outcomes of 101 Patients with Nonmetastatic Bladder Cancer Treated with Robot-Assisted Radical Cystectomy, Stratified According Ileal Ortothopic Neobladder Reconstruction: Intracorporeal vs Extracorporeal
Of all patients, at least one complication occurred in 74.3%, 75.4% vs 72.7% in ICNB vs ECNB, respectively (p = 0.9; Table 2). Early complication occurred in 57.1% vs 59.1% of ICNB vs ECNB patients (p = 0.9), with overall 19.3% vs 20.5% of Clavien–Dindo grade 3; late complication occurred in 42.1% vs 36.4% (p = 0.6), respectively, with overall 28.1% vs 25.0% of Clavien–Dindo grades 3 or 4.
Fever was the most common early complication that occurred in 17.5% vs 15.9% of ICNB vs ECNB patients, respectively. Among early complications the highest mismatch in favor of ICNB was found for acute renal failure, relative to ECNB (0% vs 4.5%), whereas the highest mismatch in favor of ECNB was found for deep venous thrombus or pulmonary embolism, relative to ICNB (7.0% vs 2.3%). Hydronephrosis or ureteral stricture was the most common late complication that occurred, respectively, in 17.2% vs 18.2% of ICNB vs ECNB patients.
Among late complications the highest mismatch in favour of ICNB was found for infections, relative to ECNB (1.7% vs 6.9%), whereas the highest mismatch in favour of ECNB was found for cardiovascular event, relative to ICNB (1.7% vs 0%). Supplementary Table S1 summarizes the specific early and late complications occurred.
At MLRMs focusing on complication rate (Supplementary Table S2) adjusted for year of procedure interval, operative time, EBL, age, and BMI, there was no statistically significant difference between ICNB vs ECNB for overall (p = 0.8) complications. Similarly, at MLRMs focusing on complication rate adjusted for only year of operation interval, age, and BMI, there was no statistically significant difference between ICNB vs ECNB for both early (p = 0.6) and late complications (p = 0.8).
Oncologic and functional outcomes
No statistically significant differences (Table 3) were recorded for definitive pathologic T stage (p = 0.5) and N stage (p = 0.5), and for tumor relapse rate (12.3% vs 13.6% for ICNB vs ECNB, respectively; p = 1.0). No PSMs were recorded in both groups. After a median follow-up of 26 months (interquartile range = 16–42), overall five (4.9%) patients died owing to cancer specific mortality, three (5.3%) and two (4.5%) in ICNB and ECNB groups, respectively. Furthermore, four (4.0%) patients died because of other-cause mortality, one (1.8%) and three (6.8%) in ICNB and ECNB groups, respectively.
Oncologic and Functional Outcomes of 101 Patients with Non-Metastatic Bladder Cancer Treated with Robot-Assisted Radical Cystectomy, Stratified According Ileal Ortothopic Neobladder Reconstruction: Intracorporeal vs Extracorporeal
PDE5i = phosphodiesterase 5-inhibitor.
For those patients whose functional data could be retrieved, at 12 months of follow-up the daytime continence recovery was 89.4% vs 87.1% (p = 1.0) for ICNB vs ECNB, respectively (Table 3). The nighttime continence was 63.8% vs 51.6% (p = 1.0) for ICNB vs ECNB, respectively.
Potency recovery was 59.1% vs 54.3% (p = 0.5) for ICNB vs ECNB, respectively (Table 3). Particularly, potency recovery rate in ICNB group was 40.9% and 18.2%, respectively, with or without PDE5i, whereas potency recovery rate in ECNB group was 27.7% and 28.6%, respectively, with or without PDE5i.
Discussion
Contemporary literature recognizes a need to address whether an intracorporeal approach for neobladder reconfiguration offers advantages over extracorporeal approach. To address this unmet need, we investigated surgical and functional outcomes, as well as complication rate, of patients with nonmetastatic BC treated at our Institution. We hypothesized a difference in surgical outcomes, such as operative time, EBL, hospital stay, and catheter indwelling, when ICNB and ECNB at RARC are compared. Similarly, we postulated a difference in overall, early, and late complication rates, and functional outcomes.
We tested our hypotheses on our Institutional database, where data from 101 patients treated with either INCB or ECNB at RARC between 2014 and 2019 were prospectively collected and retrospectively analyzed, identifying several noteworthy findings.
First, annual rates of RARC with neobladder reconfiguration sharply increased from 45.2% to 85.7% over the study span, relative to open procedure. This trend is concordant with that reported by Gill and Cacciamani in US patients, where a 11-fold increase of RARC has been recorded from 2005 to 2015. 1 Moreover in our study, ICNB was more often performed more contemporary relative to ECNB. This finding validates previous results recorded in a large multi-institutional study, 2 where Hussein et al. 2 reported a sharp increase of ICUD at RARC from 2006 to 2014 in both Europe and North America. Taken together, these findings suggest a great effort of the international urologic community aiming at increasing the robot-assisted approach rate for the treatment of nonmetastatic BC, with particular attention to ICUD reconfiguration.
Second, no statistically significant difference was recorded for median EBL (400 vs 500 mL; p = 0.9). Despite the magnitude of EBL reported in our study similar to that previously reported (ranging from 300 to 500 mL for both ICUD and ECUD) 2 –4 in literature, ICUD EBL was significantly lower compared with ECUD. Moreover, previous studies reported lower transfusion rate for ICUD (5.0%–16.9%), relative to ECUD (8%–23.5%). 2 –4 In addition, in our study a trend toward a lower ICNB transfusion rate was identified (1.8% vs 11.4%; p = 0.1), relative to ECNB, although it was not statistically significant. Finally, we recorded a longer median operative time in ICNB group (520 vs 455 minutes; p = 0.02; Table 1). This finding differs from those recorded in previous studies, where ICUD was compared with ECUD. 2 –4 However, in those studies, most patients received an ileal conduit diversion after RARC and no specific analyses regarding neobladder reconfiguration were conducted.
In consequence, this might hamper any direct comparison between our results and those previously reported. Moreover, several studies reported ICUD associated with long operative time regardless the type of reservoir reconfigured. 10,15 –17 Nevertheless, it was also reported that increasing experience and standardization of the technique favor the operative time reduction. 10,18,19
Third, similar median LOS was recorded in both ICNB and ECNB groups (11 vs 12 days, respectively; p = 0.5). These findings are consistent with recent studies reporting results of patients who received ICNB at RARC (median LOS 8–17 days). 5,6,9,10 However, it is difficult to compare our results with ECNB series.
Similarly it is difficult to compare the bladder catheter-indwelling period with other series because data are very sparse or reported just in small series. In our study, almost three of four patients removed the bladder catheter at 14th postoperative day, in both ICNB and ECNB groups (75.4% vs 72.7% respectively; p = 0.9). In a recent study in which only ICNB at RARC was evaluated, 20 the median bladder catheter-indwelling period was 21 (19–22) days. In our clinical practice, the goal was to remove bladder catheter on the 14th postoperative day after the second negative urethrocystography. In consequence, we preferred to report the bladder catheter-indwelling period in percentage of patients who removed the catheter on the 14th day, and identified that high rate of patients in both ICNB and ECNB group reached the aimed goal.
Fourth, of all patients, in almost three four patients at least one complication occurred, 75.4% vs 72.7% in ICNB vs ECNB, respectively (p = 0.9). Early complication occurred in 57.1% vs 59.1% of ICNB vs ECNB patients (p = 0.9), with overall 19.3% vs 20.5% of high-grade complication; late complication occurred in 42.1% vs 36.4% (p = 0.6), respectively, with overall 28.1% vs 25.0% of high-grade complication. Moreover, at MLRMs, no statistically significant difference in complication rate was found between ICNB and ECNB. Regarding this topic no agreement has been found in literature.
Our findings are consistent with those reported by Lenfant and colleagues. 3 In their multi-institutional study, the authors found that rate of early (overall: 38.2% vs 47.3%, p = 0.4; high-grade: 9.5% vs 5.9% p = 0.5) and late (overall: 29.4% vs 18.9%, p = 0.2; high-grade: 12.2% vs 17.6% p = 0.5) complications did not significantly differ between ICUD and ECUD patients.
Conversely, in a large institutional series, Zhang and coworkers reported that ICUD was associated with lower early (overall: 37.5% vs 43.2%, p = 0.005; high grade: 10.0% vs 17.9% p = 0.002) and late (overall: 44.2% vs 48.3%, p = 0.04; high-grade: 16.9% vs 24.8% p = 0.015) complication rate, compared with ECUD. Moreover, on MLRMs, ICUD demonstrated reduced late major complication rate (odds ratio 0.58, p = 0.037). 4 On contrary, the International Robotic Cystectomy Consortium reported that ICUD patients experienced overall higher rate of complication (57% vs 43%, p < 0.01) and higher rate of high-grade complications (13% vs 10%, p = 0.02). 2 Nevertheless, a decreasing trend was described over time.
Despite the importance of these findings, as aforementioned in those studies, most patients received an ileal conduit diversion after RARC, relative to ortothopic neobladder, and no specific analyses regarding neobladder reconfiguration were conducted. This stratification might result particularly important considering the higher complexity of the neobladder reconfiguration and consequently the plausible higher rate of complication, relative to the ileal conduit diversion. In consequence, this unmet need hampers any direct comparison between our results and those previously reported and might justify the higher magnitude of complication rate of our results, when compared with these studies.
Conversely, when compared with recent studies focusing on ICNB our complication outcomes are similar. In these studies early complication rate varied from 21.4% to 44.4%, with 9.6%–17.8% of high-grade complication rate, whereas late complication rate varied from 21.4% to 77.8%, with 11.9%–35.5% of high-grade complication rate. 5,6,9,20
Taken together our findings showed similar LOS, EBL, and transfusion rate between ICNB and ECNB, and with those previously reported. On the contrary, RARC and ICNB still remain a longer surgical procedure compared with ECNB or ORC. Despite a high overall complication rate, no difference was found between ICNB and ECNB, and with the complication rate previously reported in studies that focused on ICNB at RARC.
Moreover, a minority of patients experienced a high-grade early or late complication, and the rate of high-grade complication was similar to that published in previous randomized trials that compared RARC and ORC (21%–22% for both approaches). 21,22 Finally, a decrease in EGFR after 3 months, relative to preoperative EGFR, was recorded in both groups. Despite a slightly higher decrease was recorded for ICNB group, no statistically significant difference was found between groups.
For those patients whose functional data could be retrieved, at 12 months of follow-up the daytime continence recovery, defined as the use of 0–1 pad, was 89.4% vs 87.1% (p = 1.0) for ICNB vs ECNB, respectively. The nighttime continence was 63.8% vs 51.6% (p = 1.0) for ICNB vs ECNB, respectively. It is difficult to compare functional results with those already existing in literature and to draw definitive conclusions. Functional outcomes might be influenced by patient characteristics, such as existing comorbidities and prior treatments, but also by surgeon experience, hospital volume, and technique adopted.
Moreover, there is lack of data regarding stratification between ICUD vs ECUD at RARC and specific analyses comparing these two approaches regarding continence and potency recovery. However, our ICNB continence rate is comparable with that of previous studies that focused on neobladder reconfiguration at RARC. In these studies, continence rates for RARC with orthotopic neobladder reconfiguration ranged from 73.3% to 100% during the daytime and 51.4%–73.0% at nighttime. 5 –9 More difficult is to compare ECNB continence rate with previous studies because data are very sparse or retrieved from small series. Moreover, it is also difficult to compare ECNB continence rate with that reported in ORC series.
A large variability in fact was reported for continence rate after ORC, ranging from 18% to 92% at 12 months. 8 Difference in continence definition is the major culprit of this variability. Actually the most used definition of daytime and nighttime continence is the usage of 0–1 safety pad. When this definition was adopted at 12 months, male ORC showed ∼70% of daytime and 37% of nighttime continence rate. 23
In this study, potency recovery was 59.1% vs 54.3% (p = 0.5) for ICNB vs ECNB, respectively. Particularly, potency recovery rate in ICNB group was 40.9% and 18.2%, respectively, with or without PDE5i, whereas potency recovery rate in ECNB group was 27.7% and 28.6%, respectively, with or without PDE5i. As aforementioned for continence, also for potency recovery there is a large variability of definition. More often potency was defined as erection adequate for intercourse, with or without PDE5-i, or assessed through validated questionnaires, such as the International Index of Erectile Function score. In addition, some authors considered for potency recovery analyses only those patients who did not have preoperative ED. In consequence, a wide range of recovery rate at 12 months after nerve-sparing RARC was recorded, extending from 9% to 72.5%. 7 –11
Despite the novelty of our findings, important limitations need to be acknowledged. First, our data represent a retrospective analysis with high potential for selection biases. To maximally reduce biases, we relied on multivariable adjustment. However, it is highly possible that residual difference persisted according to variables that are unavailable in our database. Particularly surgical characteristics, such as difference in reconfiguration shape and learning curve, could impair intraoperative and postoperative outcomes. However, all surgeons involved were highly experienced in both ORC and robot-assisted urologic interventions. In consequence, this might have limited the impairment from surgical residual biases.
Furthermore, although our two groups demonstrated similar baseline characteristics (i.e., age, BMI, and tumor stage), biases from unassessed covariates, such as patient selection, preoperative functional and socioeconomic status, and social support, may have affected the quality of the results. Moreover, unknown confounding factors, such as anatomic differences or pathologist experience, may have generated anomalies in results, which for example might explain the unexpected difference in lymph node yield between groups. Regarding complication rate, although accessible outside records were reviewed, it is possible that some complications were missed from patients who were lost to follow-up.
Finally, quality-of-life assessments were not included because of lack of pre-intervention data from validated surveys. In consequence, our findings require prospective validation in future randomized trials.
Conclusions
RARC was a feasible approach for the treatment of nonmetastatic BC. Although the overall complication rate recorded was as high as 74.3%, approximately only one of five patients experienced a major early complication, whereas in one of four patients a major late complication occurred. Neither univariable nor multivariable analyses were able to find any statistically significant difference in complication rate (overall, early, or late), when ICNB and ECNB were compared. No statistically significant difference was found in continence and potency recovery between ICNB and ECNB reconfiguration.
Footnotes
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Author Disclosure Statement
Authors declare no conflicts of interest, including specific financial interests or relationships or affiliations relevant to the subject matter or materials discussed in the article.
Funding Information
This study did not receive direct funding. We acknowledge the Italian Ministry of Health for partial support with Ricerca Corrente and 5 × 1000 funds.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.