
Abstract
Objective:
Recent developments in minimally invasive approaches to radical prostatectomy (RP) for localized prostate cancer have improved oncological outcomes, but may also affect surgical scar cosmesis, an important component of survivorship and patient quality of life. Our aim was to evaluate surgical scar appearance based on operative approach to RP using a validated tool for evaluating psychosocial impact of scar appearance.
Methods:
Men between the ages of 45 and 80 were surveyed on an online crowdsourcing platform. Well-healed surgical scars after open, multiport (MP) robotic (transperitoneal and extraperitoneal), and single-port (SP) robotic RP were digitally rendered on stock photos to control for patient appearance. Respondents evaluated images using the SCAR-Q© psychosocial impact domain. Additionally, different RP scars were ranked by appearance and assigned 10-point appearance scores.
Results:
Two hundred thirty-four surveys were included for analysis (completion rate 84.2%). The median age was 54 (IQR: 49–61) and 35% (85/234) had previous abdominal surgery, of which 45% (38/85) was robotic or laparoscopic. SP scars had better psychosocial impact scores (median 100 out of 100 vs 69 and 58) than MP and open, respectively (both p < 0.001). SP scars were consistently ranked higher by appearance (median rank 1, IQR: 1–1) than MP (2, IQR: 2–3) and open (3, IQR: 3–4) (p < 0.001). SP without assistant port had the highest appearance score (median 9, IQR: 7–9) among all scars (p < 0.001).
Conclusion:
SP scars scored highest on psychosocial impact and were consistently ranked highest in appearance. These findings may be informative for optimizing both cosmetic appearance and quality of life for patients undergoing RP.
Introduction
Prostate cancer (PCa) is the most common solid organ malignancy among men in the United States, typically affecting men over the age of 50. 1 Radical prostatectomy (RP) is a standard of care, definitive treatment for localized PCa. 2 For patients with localized PCa, similar to other malignancies with definitive treatment options and favorable prognoses, patient quality of life and survivorship play an essential role in guiding treatment decision making. With the widespread adoption of robot-assisted RP (RARP), there has been considerable interest in comparing patient outcomes based on operative approach to better inform patient decision making and treatment selection. 3 –5 The recent introduction of a dedicated single-port (SP) platform has again revitalized the debate surrounding the comparative benefits and value of differing operative approaches, with the discussion now focused on comparing the standard, multiport (MP) RARP to SP RARP. 6,7 Early evidence has suggested that SP RARP has similar early oncologic and functional outcomes with an improvement in postoperative pain and hospital stay compared with MP. 8
While much of the debate about the comparative value of different minimally invasive robotic approaches to RP has centered on the oncologic, functional, and perioperative morbidity, 6,8,9 few have considered the potential psychosocial benefits to improved cosmetic outcomes, which may be an important consideration in patient survivorship and quality of life. To date, there have been few studies on the cosmetic benefits to more minimally invasive approaches to RP, 10 –12 and none that has evaluated cosmesis using patient-reported outcomes (PROs). As fewer ports and smaller incisions appear to have a beneficial relationship to perioperative morbidity and recovery, we hypothesize that a similar relationship exists with scar appearance and quality of life.
In contrast to perioperative outcomes, a comparative assessment of cosmetic appearance presents a number of challenges related to the subjectivity of cosmesis and variability in patient appearance. Furthermore, PCa patients may be biased by their personal experiences with surgical treatment selections and outcomes. To overcome these challenges, we utilized a medical illustrator to digitally render realistic surgical scar patterns on stock photos based on operative approach. Using the psychosocial impact domain of SCAR-Q©, a validated PROs instrument for surgical scars, and a commercial crowdsourcing platform, we compared the cosmetic and psychosocial benefits of different surgical approaches to RP.
Materials and Methods
Surgical scar illustrations
After receiving Institutional Review Board acknowledgement, a medical illustrator rendered well-healed surgical scars on multiple different stock photos of men's abdomens for each surgical approach to RP, including open RP with and without staples, standard MP RARP for both extraperitoneal and transperitoneal approaches, and SP robot-assisted RP with and without an assistant port (Fig. 1). The illustrated scars were drawn with uniform thickness and color to control for scar characteristics. All MP robotic port-site scars were 8 mm in length, which included a 12 mm assistant port incision in the right lower quadrant. Transperitoneal MP scar patterns also included a second 5 mm assistant suction port. Transperitoneal MP RARP scar patterns were illustrated with a supraumbilical extraction site. Meanwhile, extraperitoneal MP and SP patterns were represented with periumbilical extraction scars as performed at our institution. The stock photos were selected to match the age-appropriate physical appearance of a PCa patient and included both Caucasian and African American men. To control for baseline patient appearance for all scar comparisons, each stock photo had every scar configuration from the multiple RP surgical approaches applied.
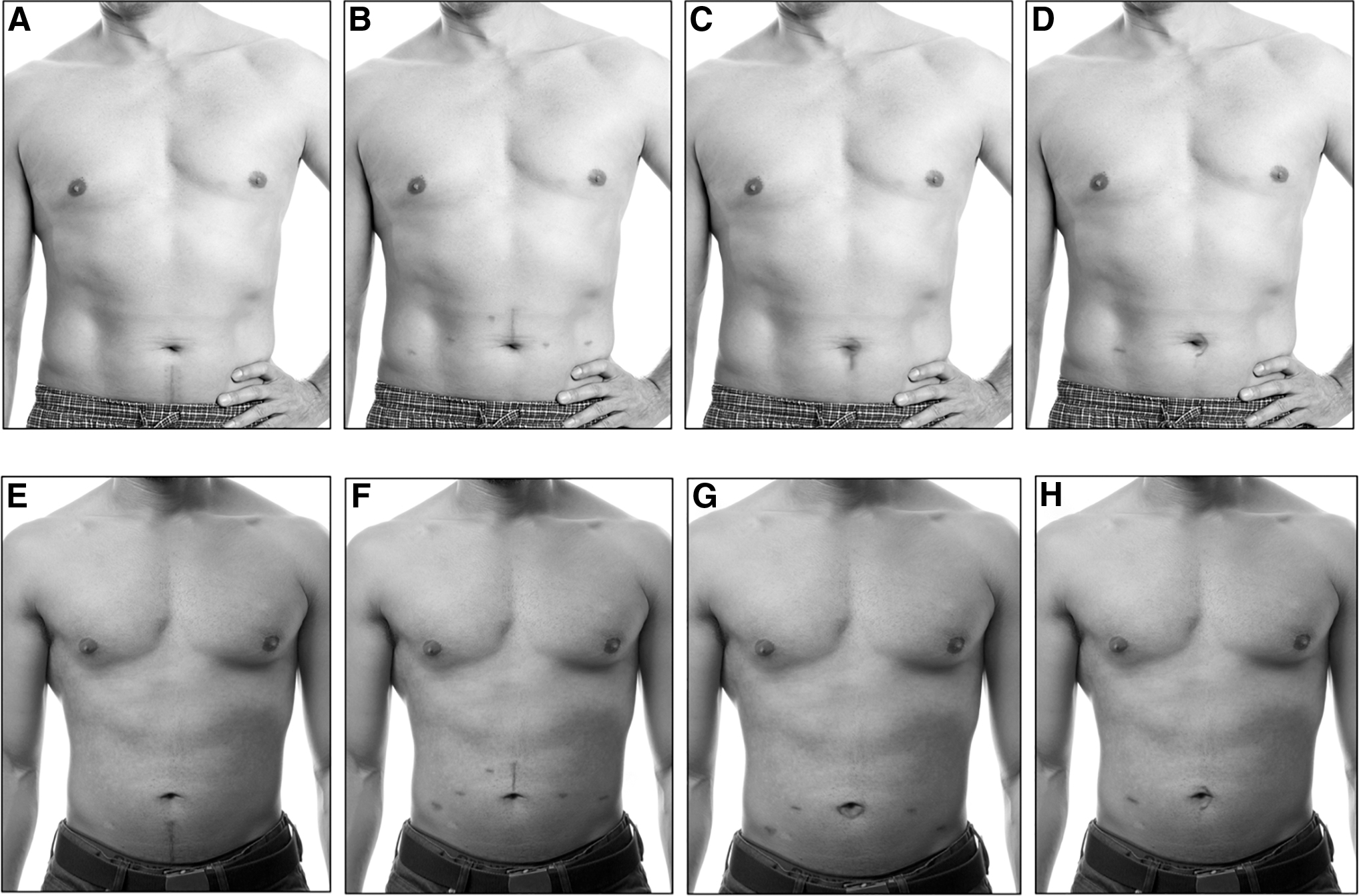
Scar illustrations provided to survey respondents. A medical illustrator digitally rendered well-healed surgical scars for different approaches to RP, including
Survey population
Given concerns about how personal experiences with treatment selection and outcomes might bias survey responses, we did not administer the survey to patients with PCa. Instead, our survey was administered to men between the ages of 45 and 80, to capture the age range in which men are typically diagnosed with PCa, through a commercially available crowdsourcing platform, Amazon Mechanical Turk (Amazon, Seattle, WA), which deploys paid workers to complete surveys and tasks. This approach was selected to maximize objectivity when comparing the relative value of different surgical scars. To ensure familiarity with the platform and reliability among survey respondents, participants needed to have completed a minimum of 500 previous tasks on Amazon Mechanical Turk and have an approval rating of over 97% based on response quality from prior tasks. All participants who had a personal history of PCa, including those who had undergone an RP, were excluded from analysis.
Survey design
Our survey consisted of three main parts that included the respondents' basic demographic information, a comparative assessment of scar appearance, and the psychosocial impact domain of the SCAR-Q questionnaire, a PROs instrument for surgical scars. The basic demographic information requested included prior history of PCa and RP, as well as information about any past abdominal surgeries that resulted in surgical scars. To assess the comparative cosmetic appearance of RP scars by operative approach, participants were asked to score SP with and without assistant ports, transperitoneal MP, and open RP scars based on appearance using a 10-point scale, with 10 as the best possible appearance. In addition, to avoid neutral responding bias, our survey also asked respondents to rank different combinations of surgical scars (open with and without staples, extraperitoneal MP, transperitoneal MP, and SP) from best to worst. Lastly, we evaluated the perceived psychosocial impact of the surgical scars using the SCAR-Q, a validated PRO instrument for evaluating the appearance and psychosocial impact of surgical scars. 13,14 The psychosocial domain score, which consists of five questions, was scaled up to a total score of 100 points using the conversion table provided in SCAR-Q, with 0 as “worst” and 100 as “best.” To avoid an order question bias, the questions were randomly ordered for each participant. Additionally, to ensure participants were reading and answering questions appropriately, attention check questions were deployed throughout the survey. Failure to appropriately answer any of the attention check questions resulted in exclusion from the study. Intuitive Surgical (Sunnyvale, CA) had no involvement in the design or execution of the study.
Statistical analyses
Respondent demographics were analyzed using basic descriptive statistics. SCAR-Q scores were compared using one-way analysis of variance (ANOVA) test; two-way ANOVA testing was also performed to evaluate the impact of respondent demographics on SCAR-Q scores. Scar ranking data were compared using Pearson's chi-squared test, with post hoc pairwise comparisons made using chi-square testing. In addition, we performed ordinal logistic regression to assess the association between personal characteristics of respondents and scar rankings. The overall 10-point appearance ratings for each scar was compared using Mann–Whitney U test with Bonferroni correction. A p < 0.05 was the cutoff for statistical significance. All statistical analyses were performed in R statistical software version 3.6.1.
Results
Survey responses
A total of 283 survey responses were collected with a successful completion rate of 84.2%. After excluding 7 responses from participants who were out of the designated age range, 7 from respondents with a previous history of PCa, and 37 surveys with incorrect answers to the attention check questions, we had 234 responses that met our inclusion criteria. The median age of respondents was 54 (IQR: 49–61). Among all respondents, 85 (35%) had previously undergone abdominal surgery, of which 38 (45%) were laparoscopic or robot-assisted surgeries. For men who had previously undergone abdominal surgery, the median satisfaction with their surgical scar was a 2 (IQR 2–3) out of 5, indicating “somewhat dissatisfied” (Table 1).
Respondent Satisfaction with Previous Abdominal Surgery Scar
Appearance scores and ranking
The highest rated scar by appearance was SP without an assistant port, which had a median score of 9 (IQR: 7–9) out of 10 (Table 2). SP without assistant port, SP with an assistant port, and transperitoneal MP scars were all given scores higher than open RP (p < 0.001). SP without an assistant port had significantly higher appearance scores than SP with an assistant port (p = 0.04) (Fig. 2). When ranking the relative cosmesis of different scars, SP scars on average ranked the highest, followed by extraperitoneal MP, transperitoneal MP, and open RP scars (with or without staples) (p < 0.001) (Table 3). Comparing MP RARP approaches, extraperitoneal MP had a consistently higher appearance ranking than transperitoneal MP when compared with other scars (p < 0.001). The presence of scars from staples did not significantly affect the ranking of open scars relative to the robot-assisted scars (p = 0.9). In an ordinal logistic regression model, neither age (p = 0.9 for ≤60 vs >60 years), personal history of abdominal surgery (p = 0.9), or satisfaction with cosmetic outcome of previous abdominal surgery (p = 0.9) were associated with ranking of scars by appearance.

Ten-point appearance scale for different types of single-port scars. Patients were asked to rank scars on a scale of 1 (worst) to 10 (best) on appearance. There was a significant difference between single-port without assistant port and single-port with assistant port (p = 0.04).
Appearance Scores for Different Surgical Scars
Patients were asked to rank the appearance of each scar on a scale of 1 (worst) to 10 (best).
p < 0.001 using one-way ANOVA test.
Compared with open (with staples) using Wilcox rank-sum test with Bonferroni correction.
p = 0.04 when compared using Wilcox rank-sum with Bonferroni correction.
Ranking of Surgical Scars
p-Value of <0.001 for Pearson's chi-squared test. Individual pairwise comparisons were all p < 0.001.
SCAR-Q psychosocial impact scores
Among the three surgical approaches, SP robot-assisted RP had higher SCAR-Q psychosocial impact score of 100 (IQR: 77–100) than both MP (69, IQR: 58–77) and open scars (58, IQR: 45–77) (p < 0.001) (Fig. 3). This was true regardless of the age of respondents (p = 0.5 for ≤60 vs >60 years), personal history of abdominal surgery (p = 0.8), or satisfaction with the cosmetic outcome of previous abdominal surgery (p = 0.8).
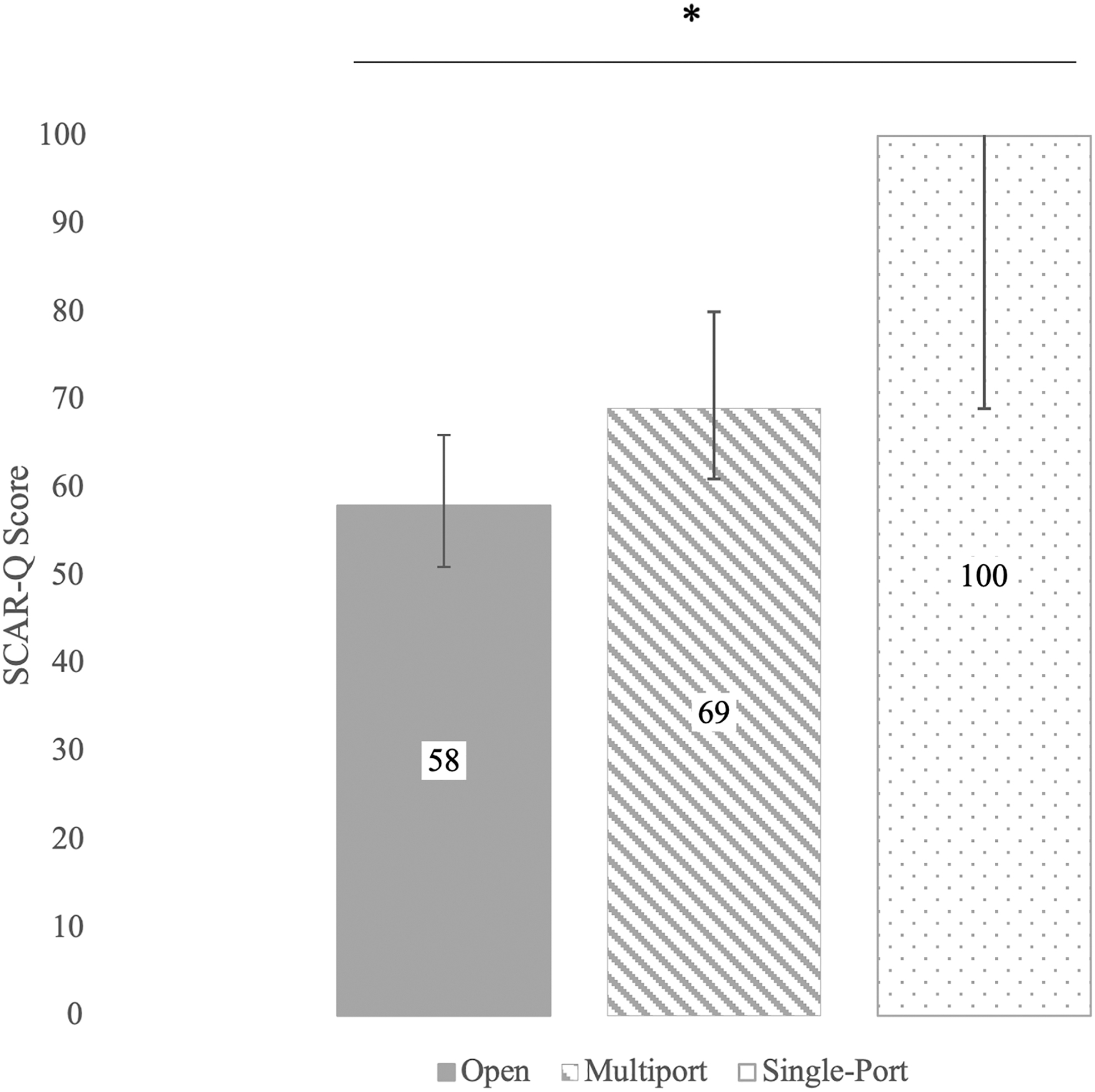
SCAR-Q© psychosocial domain scores for different surgical scars. SCAR-Q scores are presented on a scale of 0 (worst) to 100 (best). *p < 0.001.
Discussion
Due to the high disease incidence and favorable prognosis among men with localized PCa, there are more than 3 million PCa survivors in the United States today. 15 Similar to other malignancies, particularly those with effective options for definitive treatment, patient quality of life and survivorship play an essential role in PCa shared treatment decision making. 16,17 As the use of RARP continues to expand and new surgical approaches are introduced, the lifelong cosmetic implications related to scar appearance and quality of life have yet to be characterized. We report a comparative study evaluating RP surgical scar cosmetic preferences based on operative approach. Using a validated PRO instrument and comparative appearance measures, we found that SP scars had the best appearance and perceived psychosocial impact, ahead of both MP and open RP scars in men within the typical age range of PCa diagnosis. When directly comparing the appearance of scars from all approaches, respondents consistently ranked SP scars ahead of MP and open RP scars. Furthermore, we also identified more nuanced cosmetic preferences within the MP and SP approaches. For instance, extraperitoneal MP scars were ranked higher than transperitoneal MP scars. In addition, SP scars without an assistant port were assigned a higher appearance rating than SP with an assistant port. These findings suggest that reducing the number of port sites results in significant improvements in perceived cosmesis, which may have implications for improving patient treatment decision making and quality of life.
Cosmetic outcome is frequently mentioned in literature when discussing potential benefits of advances in minimally invasive technology, but has rarely been studied. 6,18 While assigning value to RARP has focused on assessing safety and oncologic outcomes, patient quality-of-life outcomes should achieve similar consideration. 3,8 For RP, this includes immediate postoperative symptoms, such as pain and convalescence, but also more lasting and permanent quality symptoms, including functional recovery and cosmesis. Surgical scar cosmesis matters to patients. In one study evaluating views on natural orifice transluminal endoscopic surgerynatural orifice transluminal endoscopic surgery among patients, participants strongly favored the concept of “scarless” surgery, even with the prospect of potential increases in surgical risk. 11 Interestingly, the study found that older individuals were willing to accept higher surgical risk for improved cosmesis compared with younger patients (20% vs 10% increased surgical risk), dispelling the widely held belief that cosmetic outcomes are less important to older patients. This was supported by our study, which found that all patients, regardless of age, preferred SP over MP and open RP surgical scars. While some early studies have suggested a cosmetic preference toward MP RP over open RP among patients and reported reductions in surgical scar size with more minimally invasive approaches, 10,12 no studies to date have performed quantifiable evaluations of scar appearance or patient-reported psychosocial outcomes.
Our study demonstrated a quantifiably superior cosmetic appearance with fewer port sites, both numerically and in rank ordering. SP scars were cosmetically better than MP and the addition of an assistant port with both SP and MP scars (transperitoneal vs extraperitoneal) conferred worse cosmetic scores. Therefore, these findings suggest that the number of port sites may affect patient perceptions of cosmetic appearance. Also, in the case of SP RARP, adopting a pure SP approach through the use of a gel port may result in improved scar appearance compared with SP RARP performed with an assistant port.
In an effort to capture the quality-of-life impact that surgical scars may have on patients, the SCAR-Q was developed which, among other domains, addresses the psychosocial impact in the form of a validated PRO. To facilitate the delivery of high-value, patient-centered health care, there is a growing emphasis on applying PROs in routine clinical practice. 19 –21 Therefore, it is prudent to employ PROs in the research setting to investigate clinically relevant information that may help inform patient treatment decision making and counseling. Using the SCAR-Q psychosocial domain, our study identified a clear perceived psychosocial benefit to more minimally invasive approaches to RP, with the greatest benefit identified with SP. In the setting of cancer survivorship, considering the high rates of mental illness and body image concerns in survivors, these findings highlight the potential for improved cosmesis to positively impact PCa patient quality of life. 22 –24
As with any step in the evolution of the minimally invasive RP, the most important consideration is whether the additive value justifies the associated investment in training and cost. Early series have identified that SP RARP has equivalent early oncologic outcomes with a potential improvement in perioperative recovery and pain relative to MP, 8,9 a similar pattern identified when MP RP was introduced relative to open RP. 3,25 –28 While it remains uncertain whether the benefits of SP justify the cost, there appears to be a general correlation between a reduced surgical scar burden and postoperative pain and convalescence adding to a growing body of evidence demonstrating the potential benefits of further minimizing minimally invasive approaches to RP.
There are several noteworthy limitations to our study, which may affect its generalizability. First, as with any survey study, our study was susceptible to the many forms of response bias despite our best efforts to minimize these influences. Also, because respondents were only able to judge the surgical scars using a digital image, other important features of scars such as physical symptoms and tactile sensation were not able to be assessed and limits the approximation of the scar's psychosocial impact. Notably, we excluded those who had a personal history of PCa. While this may limit the relevance to the PCa population, we felt that having a PCa diagnosis, particularly one which was managed with RP, would introduce additional bias to the survey responses. As was done with prior works investigating cosmesis in RP, 12 we believed that the most impartial judges of cosmesis and perceived psychosocial impact would be men who have not been influenced by their own treatment and diagnosis. Future studies may prospectively attempt to answer this question in the PCa patient population. Additionally, while our intention was to control for all variables to allow for comparisons between approaches to be made, we did not account for variations in scar healing and also did not represent all body types in our illustrations, which may affect the participant's perceptions and attitudes toward the scar.
Conclusions
Among a sample of men in the typical age range of PCa patients, SP robot-assisted RP scars had superior cosmetic appearance and perceived psychosocial impact using the SCAR-Q-validated questionnaire. Furthermore, SP robot-assisted RP scars were consistently rated higher than extraperitoneal MP robot-assisted scars, which in turn were ranked higher than both transperitoneal MP and open RP scars. The addition of an assistant port to MP and SP was associated with worse cosmesis. These findings suggest that more minimally invasive approaches to RP may have a quantifiable and meaningful difference in perceived cosmetic and psychosocial outcomes, which may have implications for directing patient treatment decision making and improving PCa survivors' quality of life.
Footnotes
Acknowledgments
The SCAR-Q is a copyrighted patient-reported outcome instrument owned by Memorial Sloan-Kettering Cancer Center (New York City, NY) and McMaster University (Hamilton, Canada) and was used with permission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by an unrestricted educational grant from Intuitive Surgical, Inc. (Sunnyvale, CA) to study robotic surgical outcomes.