
Abstract
Objective:
To share the technique of posteriorly augmented anastomotic ureteroplasty with lingual mucosal onlay grafts for long proximal ureteral strictures as well as our initial experience with the technique.
Methods:
From October 2018 to September 2019, 10 cases of robotic and laparoscopic posteriorly augmented anastomotic ureteroplasty with lingual mucosal onlay grafts for long proximal ureteral strictures were recruited from our database of Reconstruction of Urinary Tract: Technology, Epidemiology and Result (RECUTTER). The perioperative and follow-up data were recorded. Complete success was defined as the absence of clinical symptoms, relieved stenosis on imaging, and a stable estimated glomerular filtration rate without serious complications.
Results:
All surgeries were completed without serious complications. There were eight laparoscopic surgeries and two robotic surgeries. The median length of defect after posteriorly augmented anastomosis was 3 cm (range, 3–5 cm). The median length of the lingual mucosa graft was 4 cm (range, 3–5 cm). The median operative time was 237 minutes (range, 189–310 minutes). The median estimated blood loss was 40 mL (range, 10–100 mL). The median postoperative length of stay was 7.5 days (range, 5–22 days). The Double-J stent was removed median 3.5 months (range, 2–7 months) after the surgery. At the median follow-up of 11 months (range, 7–20 months), all patients achieved the successful criteria of treatment.
Conclusion:
The posteriorly augmented anastomotic ureteroplasty with lingual mucosal onlay grafts for long proximal ureteral strictures is a feasible and safe technique, which may be an option especially for strictures marginally longer than those that can be safely repaired via end-to-end anastomosis.
Introduction
Ureteral trauma accounts for ∼2.5% of urinary tract trauma. 1 Iatrogenic injury accounts for ∼80% of ureteral injuries. 2 Without reasonable treatment, ureteral injury can lead to ureteral stricture, hydronephrosis, and then renal function impairment. There are many techniques for the treatment of ureteral stricture, including ureteroureterostomy, ureteral reimplantation with psoas hitch, Boari flaps, transureteroureterostomy, autotransplantation, and ileal interposition grafts, all with their own limitations.
Up to now, the treatment of long proximal ureteral stricture has been challenging. The buccal mucosa and lingual mucosa have been used in onlay ureteroplasty for clinical proximal ureteral stricture, 3 –6 and the use of the buccal mucosa is accompanied by additional complications. 7,8 Furthermore, ureteral strictures with complete occlusion or massive scaring should be incised completely to avoid stricture recurrence. 9 Augmented anastomosis has been applied in urethral stricture first 3,4 and then in ureter stricture. 6,10 –13 To avoid more invasive treatment, we performed robotic and laparoscopic posteriorly augmented anastomotic ureteroplasty with lingual mucosal onlay grafts for long proximal ureteral strictures. As far as we know, the present series reports the most cases of posteriorly augmented anastomotic ureteroplasty with lingual mucosa onlay graft.
Materials and Methods
The study was approved by the ethics committee of Peking University First Hospital. From October 2018 to September 2019, 10 patients with proximal ureteral strictures not amenable to primary excision and anastomosis underwent robotic or laparoscopic posteriorly augmented anastomotic ureteroplasty with lingual mucosal onlay grafts and were recruited from our Reconstruction of Urinary Tract: Technology, Epidemiology and Result (RECUTTER) database (
Surgical technique
Patient position and port placement for transabdominal surgery
Under general anesthesia with nasal tracheal intubation, the patient was placed in the lateral decubitus position with the affected side facing upward. The general patient position and port placement are shown in Figure 1A (robotic) and B (laparoscopic) for the proximal ureteral strictures. In practice, these positions are dependent on the location of the stricture and the body shape of the patient.

Patient position and port placement.
Excision of the stricture and the posteriorly augmented anastomotic technique
After the colon was mobilized medially, the ureter was identified. Thickening of the scar around the proximal ureter often indicates the location of the stricture. It is necessary to completely expose the stricture and the healthy ureter about 2 cm superior and inferior to the stricture (Figs. 2A, 3A, and 4A), paying attention to retaining blood supply. Since the lumen was completely obliterated or full of pathologic scar tissue (Figs. 2B, 3B, and 4B), the segment should be removed (Figs. 2C, 3C, and 4C). The posteriorly augmented anastomotic technique, which was first coined by Turner-Warwick, 14 was performed. The ureteral ends were spatulated anteriorly and joined posteriorly (Figs. 2D, 3D, and 4D). The ruler was introduced into the body to measure the defect to determine the length of the lingual mucosa.

Procedures of posteriorly augmented anastomosis with lingual mucosa onlay graft.

Procedures of laparoscopic posteriorly augmented anastomosis with lingual mucosa onlay graft.
Harvest of the lingual mucosal graft
The tongue was pulled out with a suture fixed at the tip of the tongue. The site of the harvesting graft was marked on the ventral surface of the tongue. The length was determined intraoperatively. To facilitate graft harvesting and minimize bleeding, diluted epinephrine (1:100,000) was injected submucosally. Then, the graft was thinned and shaped to an appropriate size with the submucosal muscle tissue removed carefully (Fig. 2E, G). The donor site was simultaneously sutured with 3-0 Vicryl.
Onlay fashion reconstruction of the ureter
A Double-J stent was placed across the defect to prevent misplacement of the suture into the posterior wall (Figs. 3E and 4E). The lingual mucosa graft was inserted into the abdominal cavity with laparoscopic noninvasive grasping forceps through an accessory port (12 mm) by the assistant and then sewn into the anterior defect of the ureter in an onlay fashion with the epithelium facing the ureteral lumen (Figs. 2F, 3F, and 4F). Suturing was performed in a running manner without tension.

Procedures of robotic posteriorly augmented anastomosis with lingual mucosa onlay graft.
Omentum wrap
The reconstructed ureter segment was wrapped with a well-vascularized pedicled omentum, and then, the omentum was fixed to the psoas muscle with a 3-0 absorbable suture. Finally, a drainage tube was placed near the anastomosis.
Postoperative treatment and follow-up
A liquid diet was initiated after the surgery and was advanced to a regular diet as tolerated. Postoperative estimated glomerular filtration rate (eGFR) and renal ultrasound results were obtained at 3, 6, and 12 months postoperatively. Ureteroscopy and pyelography were performed when the Double-J stent was removed. Patient demographics, perioperative data, and follow-up data were recorded. Complete success was defined as the absence of clinical symptoms, relief of obstruction radiologically, and a stable eGFR without serious complications.
Results
As shown in Table 1, there were nine males and one female with median age of 38 years (range, 27–52 years) and median body mass index of 25.4 kg/m2 (range, 20.5–32.7 kg/m2). Etiology of stricture consisted of holmium laser lithotripsy (7), ureteropelvic junction obstruction (1), laparoscopic ureterolithotomy (1), and rectal cancer surgery (1). All the 10 patients had proximal strictures in which 3 had failed ureteral reconstruction with 1 case of pyeloplasty and 2 cases of stricture segment excision and reanastomosis.
Patient Demographics, Perioperative Variables, and Follow-up Outcomes
BMI = body mass index; EBL = estimated blood loss; HLL = holmium laser lithotrity; LOD = length of defect; LOLMG = length of lingual mucosa graft; LS = laparoscopic; PLOS = postoperative length of stay; R = robotic; UPJO = ureteropelvic junction obstruction.
There were eight laparoscopic surgeries and two robotic surgeries. All surgeries were performed without serious intraoperative or postoperative complications. The median length of defect after posteriorly augmented anastomosis was 3 cm (range, 3–5 cm). The median length of the graft was 4 cm (range, 3–5 cm). The median operative time was 237 minutes (range, 189–310 minutes). The median estimated blood loss was 40 mL (range, 10–100 mL). The median postoperative length of stay was 7.5 days (range, 5–22 days). The Double-J stent was removed median 3.5 months (range, 2–7 months) after the surgery. About 3 months after the surgery, the Double-J stent was removed, and then, the ureteroscopy was performed. The lingual mucosa graft did not heal well under ureteroscopy in four patients, so that another Double-J stent was inserted and then removed about 3 months after ureteroscopy. Depending on specific circumstances, it could be a little earlier or later.
The median follow-up duration was 11 months (range, 7–20 months). The follow-up data showed that symptoms and stenosis were relieved and that the eGFR was stable in all the 10 patients. Eight patients presented with lateral flank pain, in which one patient presented with fever, two patients were asymptomatic preoperatively while all the 10 patients were asymptomatic postoperatively at follow-up. The median eGFR was 77 mL/minute per 1.73 m2 (range, 29–120 mL/minute per 1.73 m2) preoperatively and 77.5 mL/minute per 1.73 m2 (range, 29–119 mL/minute per 1.73 m2) postoperatively at follow-up (p = 0.12). Compared with preoperative ureterography (Fig. 5A), the follow-up ureterography showed that stenosis was relieved (Fig. 5B) and anastomotic stoma healed well in ureteroscopy (Fig. 5C). Wound edema was observed at donor site of lingual mucosa graft 3 days after the surgery (Fig. 6A), and the wound healed well 3 months after the surgery (Fig. 6B). One patient developed numbness of tongue with no influence in daily life (Clavien–Dindo grade I). One patient developed abdominal incision infection responding well to dressing change and repeated upper urinary tract infection responding well to oral antibiotics (Clavien–Dindo grade II).

Preoperative and follow-up examination.
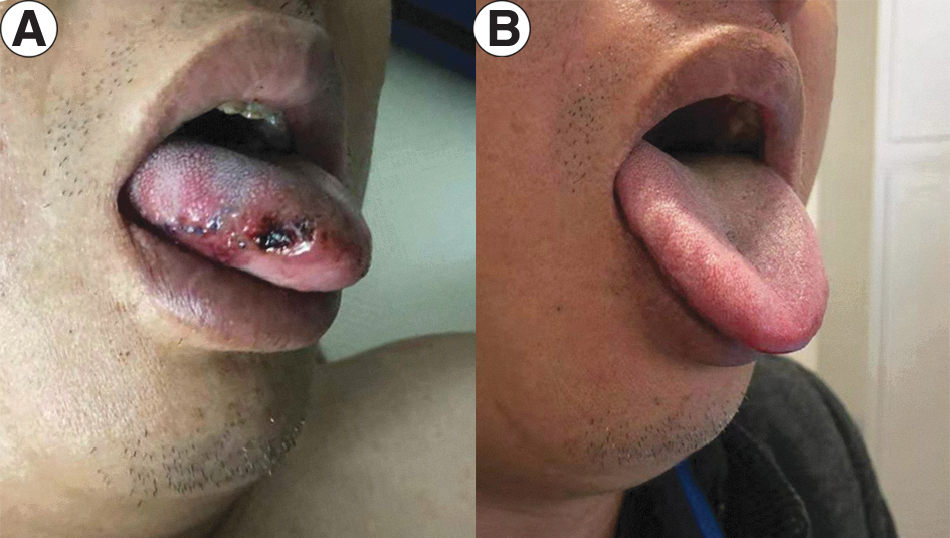
Donor site of lingual mucosa graft.
Discussion
There are many methods for the treatment of long proximal ureteral strictures. Transureteroureterostomy is an option, but the reported postoperative complication rate is 24%, the stenosis rate is 4%, and intervention or revision occurs in 10% of cases. 15 A long ureteral injury can be replaced using a segment of the intestines, but this approach is accompanied by a short-term complication rate of 42.9% and long-term morbidity rate of 23%. 16 In cases of extensive ureteral loss or multiple ureteral repair attempts, autotransplantation may be a choice. 17 Autotransplantation has excellent long-term results but is accompanied by high perioperative morbidity.
Buccal mucosa grafts are utilized in ureteroplasty. 3,4 However, there is a risk of donor site morbidities, including oral numbness (16%), mouth tightness (32%), 18 and salivary function changes. 19 In terms of urethroplasty, lingual mucosal graft is a good substitute with equally good results but lower donor site morbidity compared with buccal mucosal graft. 7 This is also true for complex hypospadias cases, and furthermore, lingual mucosal graft is easier to harvest than buccal mucosal graft. 8 What is more, neoplastic evolution of the lingual mucosa graft has not been reported in lingual mucosal graft urethroplasty according to a recent systematic review and meta-analysis. 20 Also, we have not seen neoplastic evolution in lingual mucosa graft ureteroplasty.
In 2015, lingual mucosal grafts were initially used in laparoscopic onlay ureteroplasty for clinical proximal ureteral injury. 5 In 2018, Beysens and colleagues 6 reported that robot-assisted laparoscopic ureteroplasty with lingual mucosa was feasible, effective, and minimally invasive for proximal ureteral strictures. Both studies showed that ureteroplasty with lingual mucosal grafts for the treatment of proximal ureteral strictures was safe and effective.
The buccal mucosa is suitable for ureteroplasty because of its thick epithelium, high content of elastic fibers, and rich vascularity due to the pan laminar plexus. Additionally, the buccal mucosa is compatible with wet environments resistant to infection and has good healing properties. The lingual mucosa shares these beneficial properties and is thin and easy to harvest, as the tongue can be pulled out with traction and with low perioperative and postoperative morbidity; thus, the lingual mucosa is a better alternative than the buccal mucosa. 21 Urethral biopsy of lingual mucosal graft after 3 months reveals the survival of grafted tissue with a nonkeratinizing, stratified lingual epithelium and the absence of pathologic alterations. 22 In our experience, lingual mucosal graft survived well 6 months after the surgery (Fig. 5C).
Turner-Warwick 14 first described the augmented anastomotic technique when the injury was marginally longer than that could be safely repaired. The technique consists of excision of the stricture, reanastomosis of the roof strip of the urethra, and the placement of a small flap or graft to augment the anastomosis. As shown in Table 2, Naude 10 reported the first case of augmented anastomosis with buccal mucosa graft in ureter injury in 1999. In 2015 and 2017, Zhao and colleagues and Lee and colleagues, respectively, reported the application of augmented anastomosis with buccal mucosa graft and summarized the cases in 2018. 11 –13 Then, Beysens and colleagues 6 reported the first case of augmented anastomosis with lingual mucosa graft. Therefore, we performed robotic and laparoscopic posteriorly augmented anastomotic ureteroplasty with lingual mucosal grafts for long proximal ureteral strictures. As far as we know, this article reports the most cases of posteriorly augmented anastomotic ureteroplasty with lingual mucosa onlay graft.
Outcomes of this Series Compared with Other Studies
Median (range) of the LOD after posteriorly augmented anastomosis.
UPJ = ureteropelvic junction.
The technique of posteriorly augmented anastomotic ureteroplasty with lingual mucosal onlay graft adapts the following principles: the importance of ensuring good vascular supply, the complete excision of pathologic lesions, good drainage, and a wide, spatulated, and tension-free mucosa-to-mucosa anastomosis. 9 This technique has several obvious advantages. First, complete excision of the pathologic segment is important to prevent stricture recurrence. 9 When the entire stricture cannot be excised, we advocate removing the worst portion. Second, posteriorly augmented anastomosis should be considered to reduce the anastomotic tension if end-to-end anastomosis could not be safely performed due to excessive anastomotic tension. Third, posteriorly augmented anastomosis could reduce the length of defect and then require less lingual mucosa. Certainly, it is hard to give a numeric value that will apply to all cases as to just how much of the stricture segment can be excised where a spatulated tension-free reconnection can be performed safely. This decision is influenced by ureteral elasticity and the extent of proximal and distal ureteral mobilization.
In general, tube buccal mucosal graft procedures for the management of penile strictures are associated with a very high rate of recurrence and should therefore be avoided, 23,24 and they are thought to be secondary due to the suboptimal vascularization of tubular grafts. The residual ureter plate preserves the blood supply to the graft, which is similar to nontransecting urethral reconstruction. 25 What is more, the tube mucosal graft procedure requires more mucosa compared with augmented anastomotic ureteroplasty with mucosal onlay graft. Therefore, we suggest an onlay fashion in ureteroplasty.
Furthermore, the holmium laser has been the optimum standard for URS and flexible nephroscopy currently. Postoperative ureteral stricture was 4.9% in holmium laser lithotripsy. 26 Holmium laser operations are surgical procedures that require experience and relevant endoscopic skills. The experience of the surgeon was the most important factor affecting the overall occurrence of complications. 27 To avoid or reduce holmium laser lithotrity-related ureteral stenosis, it is essential to improve endoscopic skills of the surgeon in endoscopic surgery.
The main limitations of the study lie in the small sample size and short follow-up time. A larger patient cohort and a longer follow-up duration are needed in future studies.
Conclusions
The use of posteriorly augmented anastomotic ureteroplasty with lingual mucosal onlay grafts for long proximal ureteral strictures is feasible and safe. The technique should be an option for long proximal ureteral strictures, especially for strictures marginally longer than those that can be safely repaired via end-to-end anastomosis.
Footnotes
Acknowledgments
The authors are grateful to all the colleagues who helped in the preparation of this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Scientific Research Seed Fund of Peking University First Hospital, 2018SF027.
Supplementary Material
Supplementary Video S1
Supplementary Video S2