
Abstract
While percutaneous nephrolithotomy (PCNL) remains the treatment modality of choice for kidney stones larger than 2 cm, infectious complications are most common, ranging from 5% to 32%. We present here a novel technique for potentially improving collecting system sterility during PCNL and initial postoperative outcomes. Retrospective chart analysis data of our irrigation protocol were collected from our first 56 patients between February and July 2019. Traditional prone PCNL was performed in a standard manner using fluoroscopic guidance. Using a ureteral catheter that was placed cystoscopically, a renal pelvis urine culture was taken and subsequently 10 mL of betadine solution was instilled into the collecting system. Gentamicin in normal saline (80 mg/3 L) was utilized as the irrigant fluid for the first 6 L of irrigation. From this cohort, 57% patients were women and mean age was 60 ± 14 years. About 23% of patients were diabetic and 55% were hypertensive. Seventy percent of patients had stone burden >2 cm and no patients had stone burden <1 cm. Fifteen patients had positive urine cultures treated preoperatively, while four patients had contaminated cultures. All patients were treated with our antibiotic irrigation and betadine protocol regardless of preoperative cultures or antibiotics. Mean baseline creatinine level was 0.95 ± 0.41, with a mean change of 0.18 at postoperative day 1. Of the 15 (26%) of 56 patients with a systemic inflammatory response syndrome response (two of following four criteria: white blood cells <4 or >12; heart rate >90; hypothermia <96.8°F or hyperthermia >100.4°F; and respiratory rate >20), only six patients (11%) were febrile and two patients had positive blood cultures (3%). There were no adverse reactions to the betadine or antibiotic irrigation. We present here our initial experience of a new technique for renal pelvis sterilization and its safety and feasibility using intrarenal instillation of betadine and antibiotic irrigation. No Clinical Trial Registration number applicable.
Introduction
Over the last several decades, the incidence and prevalence of kidney stones have continued to rise across the world. 1 The increasing prevalence of metabolic syndrome, including hypertension, obesity, and diabetes, has been shown to be at least partially responsible for the rising incidence of nephrolithiasis. 2,3 As such, the rate of surgical management, particularly percutaneous nephrolithotomy (PCNL), has increased from 17 to 31 per million US adults. 4 However, with increase in the PCNL utilization rate, there has been an overall increase in the rate of major complications, from <6% in 2003 to >30% now in some series. 5 This rising complication rate may be partially attributed to the increasing number of comorbidities seen in patients with nephrolithiasis.
Infectious complications after PCNL are becoming increasingly common, with the rate of fever and urinary sepsis ranging from 5% to 32% 6,7 and the overall likelihood of infected urolithiasis cases in the United States rising from 15.5 to 27.6 per 100,000. 8 Endoscopic procedures, such as PCNL, require continuous irrigation of fluids to adequately visualize anatomical structures, evacuate stones, and prevent the formation of obscuring clots. Irrigation fluid has been shown to be especially critical in the formation of patient hypothermia and electrolyte imbalance that may result in consequent perturbations in blood indices, coagulability, and cardiac arrhythmia. 9,10
A contributing factor underlying the infectious complications observed may be the use of continuous irrigation solutions and resulting intrarenal pressures during PCNL, which may contribute to bacterial dissemination. 11,12 It has been shown that stone and pelvic urine cultures are better predictors of potential urosepsis than bladder urine. 13,14 Even in the setting of patients with sterile, baseline, midstream urine cultures, a higher rate of infectious complications when not placed on antibiotic prophylaxis has been observed, suggesting that the stone-laden upper urinary tract could be a potential infectious source. 15
Given this alarming increase in infectious complications, significant effort has been focused on understanding risk factors and designing solutions to sterilize the renal pelvis. Mariappan et al. had previously demonstrated that quinolone prophylaxis reduced the rate of urosepsis in healthy tube-naïve patients. 16 A larger systematic review confirmed that prophylactic antibiotics reduced the rate of positive renal pelvic and stone cultures as well as reduced the rate of postoperative sepsis when compared with a single dose before anesthesia. 17 There has been some effort in developing an antibiotic solution capable of being instilled into irrigation at the time of PCNL; however, there are insufficient data demonstrating a significant reduction in infectious complications after PCNL. Furthermore, there are no randomized studies that show that there is any benefit from these antibiotic solutions alone.
Based on the premise that renal pelvis urine and stone cultures are likely culprits in infectious complications during PCNL, we have developed a novel protocol that aims to not only sterilize the renal pelvis before percutaneous puncture but also utilize the antibiotic-laden irrigation solution during lithotripsy and stone removal. We report here our early results on the feasibility and safety of our technique in our first 56 patients.
Materials and Methods
Renal pelvis sterilization protocol
Given the rising rates of infectious complications of PCNL, this protocol was designed with the intent of creating a means to cost-effectively reduce the incidence of these infectious complications. The focus of the protocol was to quickly and efficiently sterilize the renal pelvis collecting system before percutaneous access and during lithotripsy. To best achieve renal pelvis sterilization, we utilized a standard povidone–iodine solution (betadine, 7.5% povidone–iodine surgical preparation) that is instilled using a simple 5F open-ended ureteral catheter. The povidone–iodine solution has not only demonstrated strong virucidal and bactericidal activity in concentrations, as high as 10%, but also utility in reducing prosthetic infections noted in the penile implant literature. 18,19
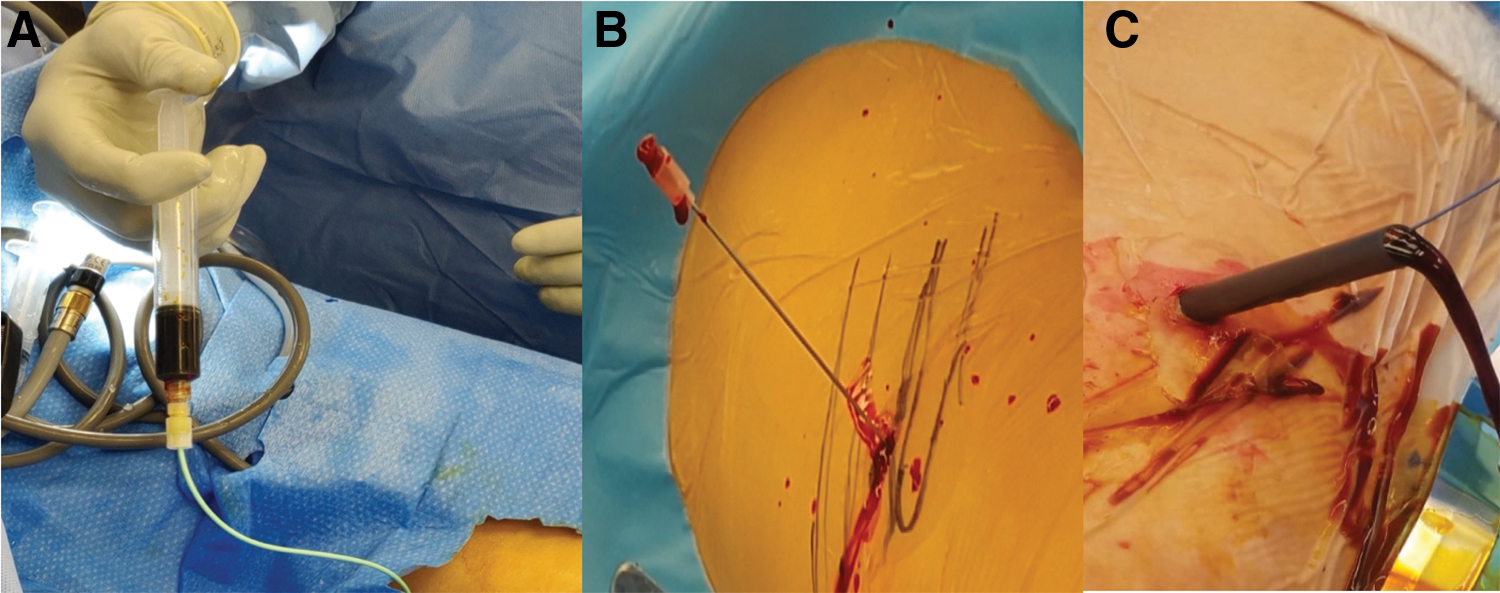
Similarly, a randomized controlled trial demonstrated that 2% instillation of povidone–iodine 2 min before cystoscopy reduced the rate of culture-positive urinary tract infection (UTI) from 22% to 7%. 20 This catheter was placed initially with flexible cystoscopy in the prone position and first used to obtain a sample of ipsilateral renal pelvis urine for culture (Fig. 1). After the culture was obtained, 10 mL of povidone–iodine was instilled gently into the renal pelvis to sterilize the cavity (Fig. 2A). Once complete, retrograde contrast instillation was utilized for pelvicaliceal anatomical delineation (Fig. 2B). For retrograde contrast instillation, the contrast solution was mixed with povidone–iodine solution in a 1:1 ratio, as opposed to saline, as is often customarily done.
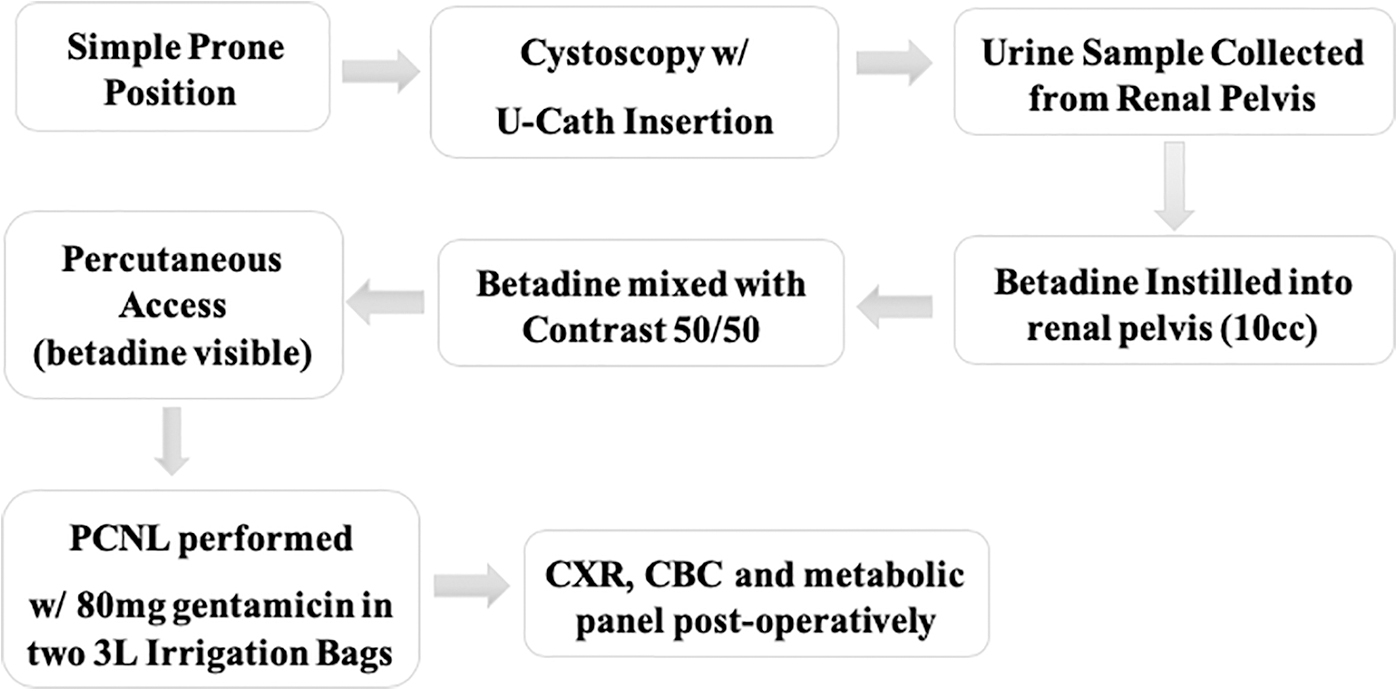
Antibiotic irrigation and povidone–iodine sterilization protocol schema during the pilot study.
Antibiotic irrigation protocol
Percutaneous renal access was obtained in a standard manner using fluoroscopy, with confirmation of collecting system access with betadine-tinged urine using a needle trocar (Fig. 2). Upon 30F sheath placement and entry into the collecting system with the rigid nephroscope, antibiotic irrigation was utilized. Given the utility of aminoglycosides against urinary flora, published utility as an irrigation solution with low systemic absorption, 21 and recommendations noted from the American Urological Association Best Practice Statement 22 during percutaneous renal surgery, gentamicin was selected for irrigation solution preparation. Gentamicin, 80 mg, was diluted in a 3-L irrigation bag of normal saline, resulting in a concentration of 26.7 mg/L.
Given the concept of the technique of pelvis sterilization, 6 L of antibiotic-laden irrigation solution was considered to be adequate before transitioning to standard saline irrigation, but could feasibly be extended for longer cases. Patients generally received first-generation cephalosporin for antibiotics perioperatively unless the patient had a history of previous UTIs, wherein alternative antibiotics targeted at speciated organisms were selected. At our institution, most patients after standard PCNL are admitted at least for overnight observation. As such, postoperative laboratory work and chest X-ray are performed both immediately upon arrival into the recovery room and the following morning.
Patient selection and outcomes
At our tertiary care center, two fellowship-trained endourologists (Z.O. and D.H.), each having performed over 200 PCNLs per year, were selected for the study. Starting in February 2019, we began using this modified technique for all consecutive PCNLs in adult patients (>18 years old). Patients with previously placed nephrostomy tubes and Double-J ureteral stents were included as part of our initial pilot population. The focus of the study was on efficacy and safety of this technique in the first 4 months until July 2019, which were evaluated using retrospective chart review. Institutional Review Board approval for this study was obtained, 20-0072.
Data and statistical analysis
Baseline demographic statistics were collected from the initial cohort of patients, including gender; age; common surgical comorbidities, including diagnoses of diabetes mellitus, hypertension, and hyperlipidemia; prior hospitalization within 90 days; and smoking status. Preoperative surgical data regarding stone size and number, preoperative urine culture status, and whether a preoperative ureteral stent or nephrostomy tube was present were collected. Intraoperative outcomes collected included renal pelvis urine and stone culture status. Postoperative clinical outcomes measured included the postoperative presence of systemic inflammatory response syndrome (SIRS) criteria (respiratory rate >20, tachycardia [>90 bpm], hypothermia [<96.8F] or fever [>100.4F], and leukocytosis/leukopenia white blood cells [WBCs] >1200/mm3, <4000/mm3]), intensive care unit (ICU) hospitalization, and bacteremia.
Our primary outcome was postoperative SIRS and/or sepsis (defined as SIRS criteria with confirmed source). The threshold for statistical significance was set as p < 0.05. Basic statistical analysis and descriptive statistics were performed using Stata 15 (StataCorp. 2017, College Station, TX).
Results
Study population and preoperative parameters
A total of 56 patients were included between February and July 2019. Most patients (57%) were women and the median age was 60 ± 14 years (Table 1). The prevalence of hypertension was 55% (31/56), diabetes 23% (13/56), hyperlipidemia 45% (25/56), obstructive sleep apnea 16% (9/56), and history of smoking 34% (19/56). Approximately 70% of all patients had total stone burden >2 cm, with about 30% of patients having total stone burden between 1 and 2 cm. Nearly 11% of patients (6/56) had been hospitalized within 90 days of the PCNL, of which 50% (3/6) were cases of stone-related urosepsis and 16% (1/6) were stone-related flank pain. Most patients had more than one stone (63%) and a negative preoperative urine culture (73%).
Descriptive Characteristics
BMI = body mass index; DM = diabetes mellitus; HLD = hyperlipidemia; HTN = hypertension; OSA = obstructive sleep apnea; PCNL = percutaneous nephrolithotomy.
All preoperative urine cultures were obtained within 30 days of the planned PCNL. The prevalence of stent and nephrostomy tube placement before PCNL was fairly low, only four (7%) patients had prior nephrostomy tube placement and six (11%) patients were with a preoperative stent. Two of the four patients had positive preoperative nephrostomy tube urine cultures, and one stented patient had a positive voided urine culture. Of the patients with positive preoperative urine cultures, two patients (26%) had extended-spectrum beta-lactamase-producing or multidrug-resistant organisms and were preadmitted for intravenous antibiotics at least 48 h before the PCNL, eight patients had gram-negative organisms, three patients had gram-positive organisms, and four patients had contaminated cultures (>3 organisms that were not speciated).
All patients with positive preoperative cultures sensitive to oral antibiotics (13/15 patients) were given antibiotics tailored to organisms seen in preoperative cultures, the majority of which received cephalosporins and the remainder of which received fluoroquinolones.
Intraoperative outcomes
Stone cultures and intraoperative renal pelvis cultures were obtained from all 56 patients. The rate of positive renal pelvis cultures was noted to be 14% (8/56) and the rate positive stone cultures was 9% (5/56) (Table 2). Of the patients with positive preoperative urine cultures (15/56), 46% had negative intraoperative urine cultures. There was a high degree of concordance between stone cultures and intraoperative renal pelvis urine cultures (80%, 4/5), of which both patients with preoperative nephrostomy tubes had identical organisms in renal pelvis and stone cultures. Of the patients with positive intraoperative urine cultures, 63% (5/8) had at least one organism similar to that of the preoperative voided urine culture.
Clinical Course
POD = postoperative day; SICU = surgical intensive care unit; SIRS = systemic inflammatory response syndrome; WBC = white blood cell.
Postoperative clinical outcomes
Postoperatively, all patients were admitted for overnight observation. Fever (measured as >101.4°F or 38.5°C at any point in the postoperative hospitalized period) occurred in about 11% of patients (5/56). Tachycardia (heart rate >90 bpm) occurred in about one-third of all patients (19/56). Five patients experienced tachypnea at some point during the hospitalization (9%). The average postoperative day (POD) 1 WBC count was noted to be 12,810/mm3 and 50% of patients had some degree of leukocytosis (28/56). No patients had leukopenia on postoperative hemograms. Overall, we report that 27% of our cohort met strict SIRS criteria (15/56). Of the 15 patients who met SIRS criteria, only 6 patients (11%) were febrile and 2 patients had positive blood cultures (3%).
In addition, to place these clinical values in context, we examined the rate of ICU hospitalization. Three patients required ICU hospitalization (5%), of which two patients were diagnosed as having sepsis (3.5%). One patient requiring ICU hospitalization was secondary to hypotension and ultimately required angioembolization. Both septic patients were bacteremic with blood cultures yielding coagulase-negative staphylococcus. Of the patients with intraoperative positive renal pelvis or stone cultures, three patients met strict SIRS criteria. Of these patients, only one patient was diagnosed as having sepsis and required ICU hospitalization.
Mean baseline creatinine level was 0.95 ± 0.40 mg/dL, with a mean change of +0.18 postoperatively. The mean postoperative creatinine level was found to be 1.13 ± 0.48 mg/dL. The overall complication rate was reported at 8.9%, with 3.5% classified as Clavien II and 5.3% classified as Clavien III. With the exception of seven patients, all patients were discharged home on POD 1, which is standard at our institution. Of the seven patients who had longer stays, three were ICU hospitalizations (one of which received a transfusion), two patients had transfusions only, one patient underwent contralateral PCNL during the same hospitalization, and the last patient was diagnosed as having acute appendicitis POD 1 after PCNL. No patients experienced significant electrolyte changes or symptoms after protocol use.
Discussion
The primary endpoint of this study was to demonstrate the safety and feasibility of this novel renal pelvis sterilization protocol as well as demonstrate early infectious outcomes with our initial cohort of patients. Infectious complications lead to the highest morbidity and mortality rates following PCNL. The Clinical Research Office of the Endourology Society PCNL Global Study showed that percutaneous treatment of stones results in overall complication rates of about 20.5%, 16.5% minor and 4% major. 23 In this study of over 90 centers internationally, about 11% of patients developed postoperative fever >38.5°C, which corresponds with our data. Various groups have reported rates of postoperative fever and infection of <3% or as high as 30%. 24,25 Systematic review of mortality rates related to stone disease showed that of 2550 mortalities, the most common cause of mortality was sepsis (around ∼9%). 26 It is of no surprise that decreasing infectious complications to reduce these morbid outcomes has been a primary goal of PCNL.
Antibiotic treatment before PCNL has been well established in the field, 24,27 yet there has been no systematic means for sterilizing the collecting system at the time of PCNL. Given that urine collected from the renal pelvis and the stone are better predictors of potential urosepsis 13 and that irrigation fluid during PCNL has been shown to be related to development of fever, 24 using a sterilizing solution intraoperatively seemed to be an ideal method by which to decrease the rate of infectious complications. This is the first study, to the best of our knowledge, to attempt to sterilize the collecting system before PCNL. Povidone–iodine was selected as the antiseptic of choice given its ubiquitous use in the operating room and relatively low cost. It has been shown in multiple arenas to not only be useful in sterilizing prosthetics/implants but also in management of intra-abdominal infections. 19,28 Gentamicin is a critical antibiotic for the treatment of gram-negative organisms and has been used for over two decades in both prosthetic salvage and intravesical instillation safely to reduce the incidence of colonization and infection. 21,29,30
Utilizing our protocol, the rate of postoperative fever (>38.5°C) was consistent with that previously published at 10.7%. Despite the overall SIRS prevalence in our initial cohort of ∼26.7%, the overall sepsis rate remained low at 3.5%. More critically, in the setting of renal pelvis urine or stone culture positivity, SIRS was diagnosed in three patients and sepsis ultimately in only one patient. Interestingly, about 50% of patients with positive preoperative cultures treated with antibiotics were observed to have positive intraoperative renal pelvis or stone cultures, underlining the importance of renal pelvis sterilization at the time of the procedure. In addition, neither septic patient showed concordance between blood culture and renal pelvis/stone culture, suggesting that even organisms from these sources may not predict urosepsis. No patients with preoperative nephrostomy tubes (4/56) were diagnosed as having sepsis or SIRS. One patient with preoperative ureteral stents was diagnosed as having sepsis, but did not require ICU hospitalization. While these results corroborate published clinical outcomes for sepsis, 7 when compared with historical cohorts from previously published data at our institution, where sepsis rates ranged from 8% to 10%, this represents a promising means by which infection-related complications may be limited. 31
In addition to aiding in decreasing infectious complications, the use of povidone–iodine instillation into the collecting system was useful for improved identification of renal pelvis access, as the urine or contrast return would be brown tinged or reddish-brown if partial access was achieved. Although not compared directly, this helped improve the speed of recognition of our access as other methods were not required to confirm appropriate access. Intraoperative visualization was not negatively affected by betadine as it would wash out soon after PCNL when full irrigation began.
Given the nature of this pilot study, there were several limitations. As the goal of this study was to first demonstrate feasibility and safety, there was no comparison with a prior protocol that did not incorporate this novel technique. The next step is to perform case-matched comparison with a historical cohort from data collected in the years before the institution of this protocol. In addition, there have been some data that suggest that povidone–iodine may result in elevated systemic levels of iodine in rats in the setting of open intestinal mucosa. 32 Therefore, to ensure adequate safety, serum iodine levels may be drawn for future patients in which this protocol is utilized to ensure nontoxic, systemic iodine levels. In addition, the utility of this protocol will likely be further corroborated in a larger multicenter study to determine if our protocol should be added to standard of care, especially in high-risk individuals. An additional avenue of study may be to compare alternative antibiotic agents in the irrigation fluid to identify optimal agents for inclusion. Recent chromatography studies have demonstrated that higher levels of fosfomycin tromethamine have been noted inside the stone, as opposed to second-generation cephalosporins. 33
While the current study has its limitations, it does appear that this technique is safe and relatively straightforward to introduce into the workflow of PCNL. This novel protocol may hold particularly significant value in the setting of colonized urinary tracts as only 1 of 10 patients with preoperative drainage tubes (either nephrostomy or ureteral stent) had sepsis despite often having positive intraoperative renal pelvis or stone cultures. However, further study will need to be undertaken before definitively establishing this protocol as the standard of care.
Conclusions
We report a novel technique for renal pelvis sterilization using intrarenal instillation of betadine and antibiotic-laden irrigation during PCNL. Overall, the rate of sepsis was low in our cohort, especially in patients with prior drainage catheters. There were no adverse reactions or complications related directly to our protocol. While more data are required to definitively claim efficacy, we believe this protocol is safe and feasible to incorporate as part of the PCNL workflow. Further research and development will be required to ultimately create a protocol to decrease the rate of infectious complications and decrease morbidity and mortality rates secondary to PCNL.
Footnotes
Acknowledgment
The authors are grateful to Alp Turgut for the support provided in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No external funding was utilized for this research study.