
Abstract
Introduction and Objectives:
Percutaneous management of large bladder calculi with the use of a laparoscopic entrapment sac is a minimally invasive procedure that may have advantages over open cystolithotomy and transurethral cystolithotripsy, as well as standard percutaneous cystolithotomy. We first performed this procedure in 2008, and refined it after our initial publication in 2013 by changing the position from lithotomy to supine by using a urethral catheter postoperatively instead of a suprapubic (SP) catheter, by using ultrasound guidance for access, and by changing the procedure from being inpatient to outpatient. Our objective is to assess the continued feasibility of percutaneous entrapment sac cystolithotomy (PESC) and describe modifications that simplify the technique (mPESC), comparing outcomes and complications.
Methods:
Forty seven male patients underwent PESC from 2008 to 2019, 16 who had PESC and 31 who had mPESC. After extraction of calculi, either an SP catheter was placed, or the wound was closed and a urethral catheter was placed. Operative and follow-up parameters were compared between the two cohorts.
Results:
All patients were rendered stone free. Procedure time and length of stay were both significantly shorter in the mPESC cohort. Stone burden and estimated blood loss were equivalent between cohorts. There were no complications of urethral trauma in either cohort. The PESC cohort had higher rates of leakage from the SP site (25% vs 0%), increased need for catheter over 5 days (18.8% vs 0%), and greater likelihood of recurrent retention (12.5% vs 6%).
Conclusions:
Modifications of PESC, mPESC, leads to fewer complications and reduced length of stay compared with the original PESC procedure. This safe and efficacious technique can reduce morbidity during the management of large bladder calculi and is well suited for an outpatient procedure.
Introduction
Historically, bladder calculi accounted for >50% of all urolithiasis; however, because of improvements in socioeconomic status and nutrition for the past century, particularly in developing countries, bladder calculi now account for about 5%. 1 –4 The incidence of bladder calculi, however, may actually be higher and increasing, in part because of aging populations. 5,6 Bladder calculi are far more prevalent in men because of certain risk factors, most notably bladder outlet obstruction (BOO); 80% to 90% of bladder calculi occur in men of which a majority have BOO. 6 –9 Open cystolithotomy (OC) was previously the gold standard operation for removal of large bladder calculi; however, long operative times, significant blood loss, increased morbidity, and prolonged catheterization and hospital stay have led to advances in technologies resulting in less invasive alternatives, including shockwave lithotripsy, transurethral cystolithotripsy (TUCL), and percutaneous cystolithotomy (PCL). 10
Newer endoscopic techniques, including TUCL and PCL, have evolved to reduce complications and improve outcomes. TUCL is an appealing surgical option because it requires no incision; however, there are some disadvantages of TUCL that potentially limit its safety and efficacy. By its nature, TUCL is a natural orifice procedure and if the urethra is of small caliber, endoscopic instruments may cause trauma to the urethral mucosa potentially leading to stricture formation. Furthermore, TUCL requires traversing a likely enlarged prostate, which limits irrigation, observation, and mobility. Taken together, this can result in greater risks of bladder mucosal injury, perforation, and decreased stone clearance. 9,11 PCL is an alternative procedure for large bladder calculi with certain advantages. PCL limits urethral and prostatic trauma and permits larger caliber instruments thereby reducing the likelihood of urethral stricture while simultaneously achieving complete stone clearance. 9 However, the time required for lithotripsy and stone fragment extraction can be substantial during PCL and there is a high risk of bladder mucosal injury from the lithotripter or the endoscope potentially resulting in bleeding, incomplete stone removal, and recurrence.
In response to these limitations and based on similar procedures that our group and others had performed in augmented bladders and continent urinary diversions, 12 –14 we developed the technique of percutaneous entrapment sac cystolithotomy (PESC) for large bladder stones in patients with normal native bladders and published our initial series in 2013. 15 We have subsequently refined our technique by changing the position from lithotomy to supine, by using a urethral catheter postoperatively instead of a suprapubic (SP) catheter, by using ultrasound (US) guidance for access, and by changing the procedure from being inpatient to outpatient. The objective of this study is to assess long-term outcomes and complications and introduce our modified PESC (mPESC) technique, comparing it with our original procedure (PESC).
Materials and Methods
After obtaining institutional review board approval, we retrospectively reviewed our endourologic database (IRB—AAAC3929) for patients who underwent PESC procedures by a single provider. Patients were considered for the procedure and included in the study if they were male, had stone burden >3 cm, had a preoperative CT scan, and were deemed not to require or did not desire bladder outlet procedures. Patients were excluded if they had CT evidence of bowel anterior to the bladder or were in urinary retention.
As previously described in our initial study, the original PESC procedure is performed under regional or general anesthesia with the patient in either dorsal lithotomy or supine position and both the SP and genital areas are exposed. Flexible cystoscopy is performed to identify the bladder calculi and allow hydrodistention of the bladder with physiologic irrigation. The dome of the bladder is identified cystoscopically, and an 18-gauge diamond point needle is placed two fingerbreadths above the pubic bone into the bladder under direct endoscopic vision. A small incision is made alongside the needle with a scalpel. A 0.038-inch guidewire is then placed into the bladder through the needle and the needle is removed. Serial dilation is performed, first with a 10F fascial dilator, and then with a 30F balloon dilator over which a 30F access sheath is advanced. The balloon dilator is removed and a 10 mm laparoscopic entrapment sac (Endocatch Gold™, Medtronic, Minneapolis, MN) is placed through the access sheath. Using the flexible cystoscope, the sac is manipulated and unfolded by placing the cystoscope into the sac and running irrigation fluid and bluntly teasing the sac open. Bladder calculi are then placed into the sac by dragging the stiff but flexible rim of the sac along the posterior bladder wall to underneath the bladder neck, bluntly but gently teasing the stones above the rim (Fig. 1). This process is aided by placing the patient into the Trendelenburg position and also by bluntly teasing stones with the cystoscope into the sac. Care has to be taken with manipulation of the stones, especially if there is an impacted stone, to not cause injury to the bladder neck, which can result in bleeding and decreased observation. Some smaller stones that elude placement and remain posterior to the sac are treated by lifting the sac so it is off the posterior wall, using a nitinol basket or flexible graspers to grab the stone, pulling the stone toward the bladder neck, lowering the sac back to the posterior wall, and then placing the stone into the sac. Once all the stones are trapped, the sac is then closed by pulling on the drawstrings that are brought up through the Amplatz sheath. The sac is quite large and long, holding 220 cc, so if the sac is not at the skin level, this is because of the sac being incompletely unraveled. This can be discerned as well through the flexible cystoscope, which can be used to more completely unfold the sac and allow the stones within to fall by gravity into the bottom. Irrigation from a nephroscope placed into the sac can also help to unfold the sac. Once the drawstring noose has been determined to be above or at the skin level, the Amplatz sheath is removed. The edges of the exteriorized sac are secured with mosquito clamps to prevent the sac from slipping back into the bladder. The Amplatz sheath is cut and shortened as desired and placed through the drawstrings to now be inside the sac. A 26F nephroscope is passed with continuous flow irrigation to fragment the stones within the sac with either pneumatic, ballistic, ultrasonic, or combination lithotripters (Figs. 2 and 3). Once all of the fragments are removed or have been fragmented enough to fit through the skin incision, the entire sac is removed. Simultaneous observation with the flexible cystoscope ensures that no stones or fragments remain outside of the entrapment sac. Only one video tower is needed and can toggle between the flexible cystoscope and the nephroscope. In the original procedure, a 0.038-inch safety wire was placed outside the sac but through the Amplatz sheath at the beginning of the case, and this was used to place a council-tip SP catheter of 20–24F at the end of the procedure.
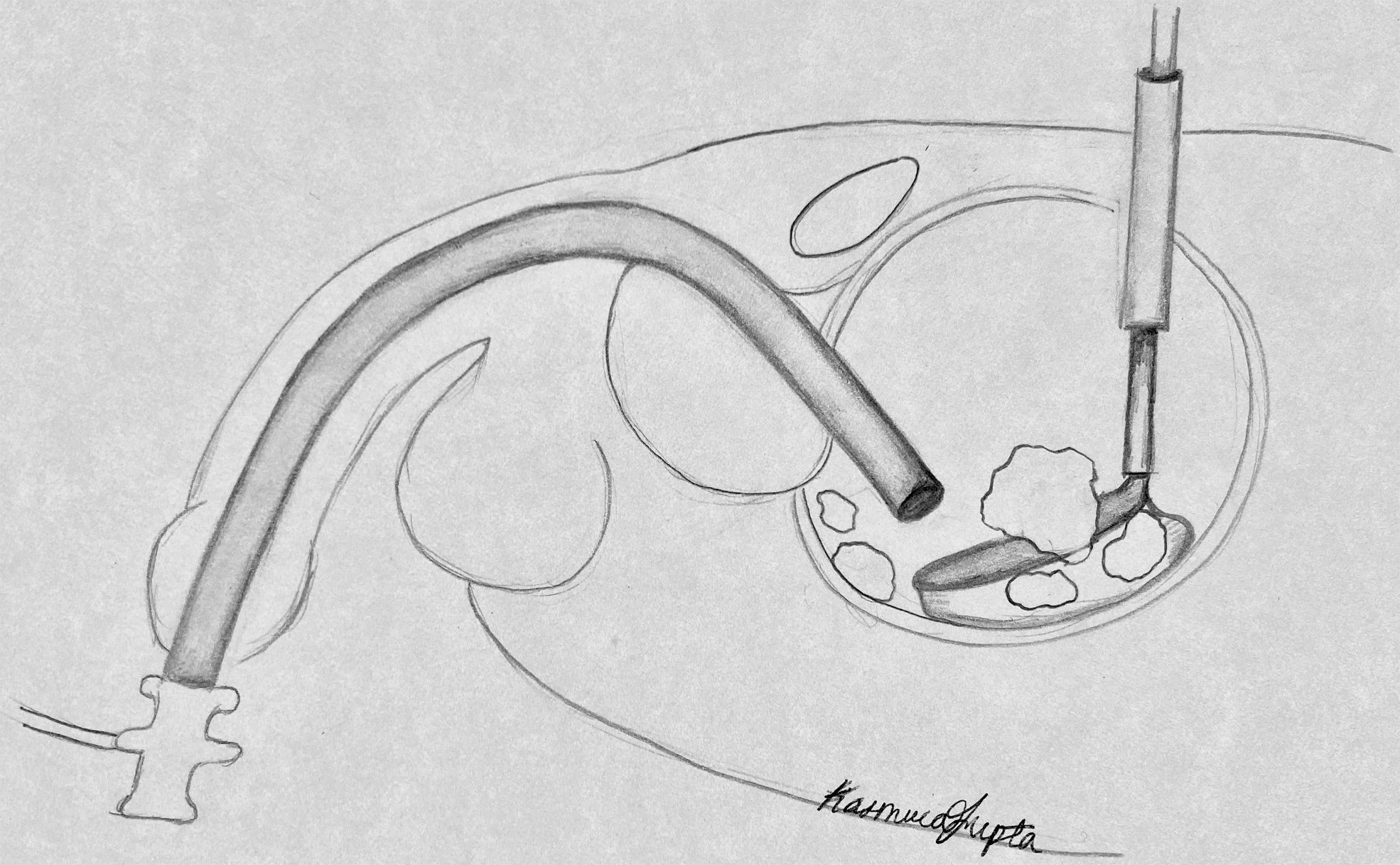
Placement of stones into laparoscopic entrapment sac.

Fragmentation of stones within laparoscopic entrapment sac.
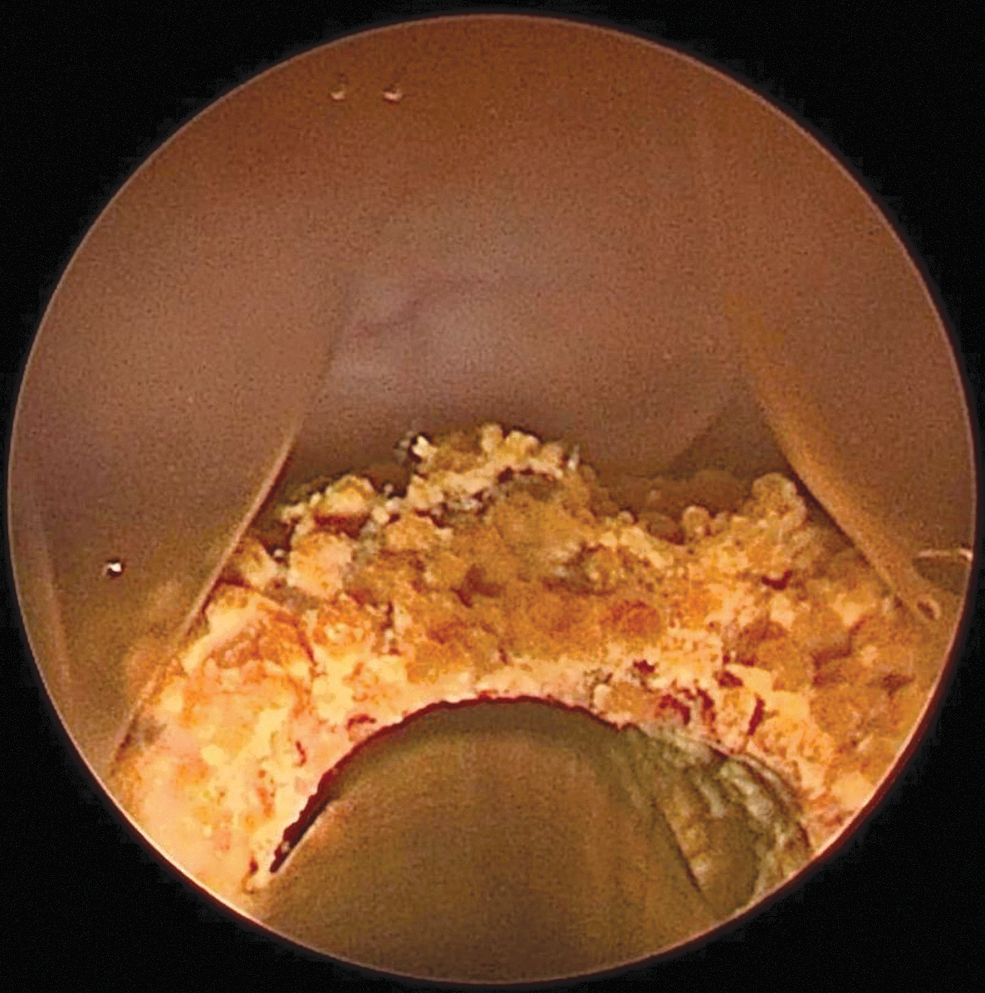
Fragmentation of stones within laparoscopic entrapment sac.
Our modified technique, mPESC, offers the following variations. The patient is always placed in a supine position. We find this makes manipulation of stones easier and allows both surgeon and assistant to be on the same side of the operating table to have a clear view of the video tower on the opposite side of the table. US is used to guide the needle puncture, which helps to prevent bowel injury and assure that the dome of the bladder is accessed (Fig. 4). Dome entry is important in making sure the entrapment sac trocar is lined up better to slide nicely along the posterior bladder wall. Instead of placing a 20–24F council-tip SP catheter over a wire, the wire is removed and a 16F 5-cc balloon standard urethral catheter is placed to gravity. Once the bladder is decompressed, the fascia is approximated with 2–0 braided mid-term absorbable suture, the skin is closed with a subcuticular 4–0 monofilament mid-term absorbable suture, and then sealed with liquid cyanoacrylate. Per our original protocol, patients in the SP catheter cohort were observed overnight and a clamp trial was performed on postoperative day 1. If patients were able to void per urethra, the SP catheter was removed. If patients failed the clamp trial, the SP catheter was left in place and the patients followed up in the office for repeat voiding trial. Patients in mPESC cohort were all discharged on the day of surgery with the urethral catheter in place and either instructed how to remove the catheter on the first postoperative day if they were felt to be at minimal risk of urinary retention or asked to come to the office in 3 days for a voiding trial in the office if they were deemed to be at higher risk of urinary retention (larger prostate, moderate postvoid residuals). Patients had a follow-up visit at 1 month to go over 24 hour urine results, measure postvoid residuals, and perform bladder US to rule out residual stones or fragments. Follow-up evaluation was also performed yearly to check voiding, adherence to antilithogenic and prostate medications, and to check voiding studies, postvoid residuals, PSA (if indicated), and bladder US to rule out recurrence.
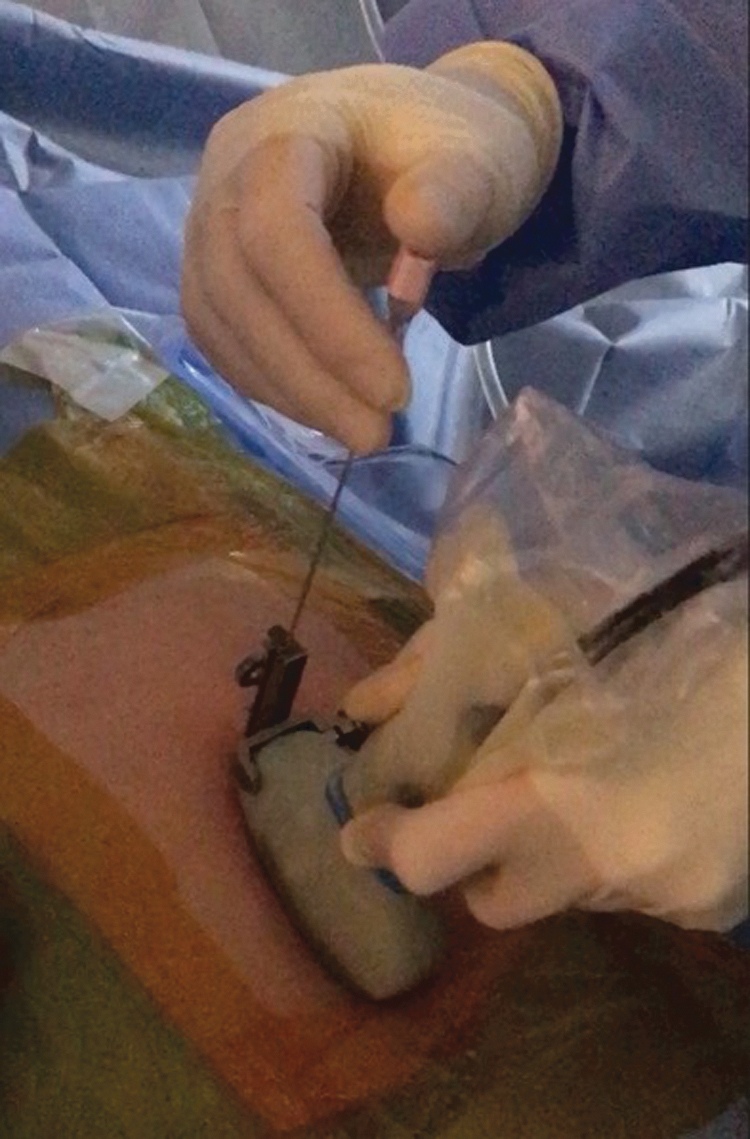
Ultrasound-guided percutaneous access.
Results
A total of 47 men with bladder calculi were included. Sixteen men were in the original PESC cohort from 2008 to 2012 and 31 men were in the mPESC cohort from 2013 to 2019. Average age was 73 in the PESC group and 68 in the mPESC group, which was not significantly different. There were also no significant differences between the two groups in the number or size of stones. Average Hounsfield units of stones for all patients was 665 ± 231.5. Average intravesical prostatic protrusion for all patients, as measured on CT in the midsagittal plane, was 14.1 mm ±5.4. The average operative time was significantly shorter for mPESC (54 minutes) compared with PESC (103 minutes, P < 0.0001). All patients were stone free at the end of the procedure, which was determined by bladder US at 1 month postoperatively. There was no significant difference in estimated blood loss (EBL) between the groups. Length of stay was significantly shorter in the mPESC group, 0 days compared with 1 day (P < 0.0001). There were no complications of urethral trauma in either group. The PESC group had higher rates of leakage from the SP site (25% vs 0%), increased need for urethral catheter over 5 days (18.8% vs 0%), and greater likelihood of recurrent retention (12.5% vs 6%). There was one complication in each group requiring an ER visit: acute retention in the PESC and a dislodged catheter in the mPESC group.
Percutaneous Entrapment Sac Cystolithotomy vs Modified Percutaneous Entrapment Sac Cystolithotomy
All analyses performed using Mann–Whitney U test, values reported in following format: Median (25th percentile, 75th percentile).
Denotes significance
mPESC = modified PESC; PESC = percutaneous entrapment sac cystolithotomy.
Discussion
Surgical removal of bladder calculi is a historically important and evolving procedure. In one of the earliest translations, Hippocrates oathed “I will not use the knife, not even, verily, on sufferers from stone, but I will give place to such as are craftsmen therein.” 16 As crafts of this trade, urologists have innovated the surgical management of bladder calculi for the past century from open procedures, including OL, to less invasive endoscopic procedures, including TUCL and PCL.
Prior studies have been performed comparing PCL with OC and TUCL. Compared with OL, PCL has been shown to have similar stone-free rates (SFRs), but shorter procedure time, decreased EBL, and reduced duration of catheterization. 17 Randomized studies comparing PCL with TUCL have shown similar SFR, complication rates, and retreatment rates, with mixed results of length of procedure and hospital stay. 10,18 –21 Yet, TUCL carries a risk of urethral stricture, seen in almost 3% of patients, which is not seen in PCL. 10 Based on these studies, the European Association of Urology issued a strong recommendation for PCL when TUCL is not possible or is associated with a high risk of urethral stricture. 22 Importantly, PCL must be used in the appropriate patient. Caution must be exercised in patients with a history of lower abdominal surgery, pelvic radiation, and history of pelvic hardware as there is increased risk of intervening bowel or foreign bodies. In these cases, a preoperative CT scan and a combination of cystoscopy and US can aid in safe percutaneous access. In addition, PCL is contraindicated in patients with a history of bladder cancer to avoid tumor spillage. 23
Innovations to PCL include the use of a laparoscopic entrapment sac, which can improve efficiency by reducing operative time through improved ease of stone clearance, especially in bladders with multiple diverticula that can harbor smaller stone fragments. Furthermore, the sac provides an additional layer of protection between the lithotripter and bladder wall to reduce mucosal trauma and keep bladder pressures low as excess irrigant escapes extracorporeally. 12 –15
In this study, we had a significant difference in operative time favoring the mPESC group. This difference is likely because of enhanced surgical skill over years of employing the percutaneous technique, as well as using supine position for easier manipulation of stones and better observation, and using US guidance for a better trajectory into the bladder and easier deployment of the entrapment sac. Furthermore, advancements in lithotripters has likely contributed to improvements in stone clearance and operative time. Patients were initially treated with the Olympus ShockPulse and since coming to market, all patients are now treated with the Swiss LithoClast® Trilogy. In addition, our study shows that primary closure of the percutaneous SP access tract and placement of a urethral catheter permits same day surgery without increased complications. In fact, we had a lower rate of complications in the mPESC group compared with the original PESC group. The PESC group had higher rates of leakage from the SP site, likely related to the SP tract remaining open longer and not having a chance to seal closed with a urethral catheter for complete bladder drainage. Overall, there were no urethral injuries, no major bleeding complications, and no bladder wall injuries.
Our study has its limitations. This is a retrospective study from a single surgeon at a single center with a relatively small sample size. Future randomized trials with a greater number of patients and longer follow-up are needed to further evaluate the safety and efficacy of mPESC.
Conclusions
Modified PESC leads to fewer complications and reduced length of stay compared with the original procedure. This safe and efficacious technique can reduce morbidity during the management of large bladder calculi and is well suited for an outpatient procedure.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding information was received.