
Abstract
Introduction and Objectives:
Published literature on damages to a digital flexible ureteroscope (DFU) examines a limited number of ureteroscopes and shows wide variation in its durability. The aim of this study was to compare the primary damage location, causes of DFU damages, and the durability of Karl Storz Flex-Xc digital ureteroscope between University Hospital (UH) and Ambulatory Care Surgery Center (ASC). We also evaluated the available literature on the durability of DFU.
Methods:
Each damaged DFU prospectively underwent a manufacturer's evaluation to determine the reason for return and primary site of damage. Hospital data on the number of ureteroscopic procedures and damaged DFUs over 3 years were retrospectively reviewed. The possible reason for the damage was classified as either intraoperative or between the procedures. The durability of DFUs, type, and cause of damage were compared between the UH and nonteaching ASC. A chi-square test was utilized for categorical variables. When cell frequencies were <5, Fisher's exact test was used.
Results:
During the study period, 1211 ureteroscopies were performed and 143 ureteroscopes were returned to the manufacturer. The mean number of uses was 7.45 at the UH and 16.5 at the ASC. The location and cause of damage were similar at both locations. The most common locations of primary damage were at the angle cover (70.6%) and instrument channel (19.2%). Most damage occurred during the handling of the ureteroscopes between surgical procedures (78%). On review of the literature, we found that DFUs were 6 times more durable in a nonteaching hospital.
Conclusions:
The DFU was more than two times as durable in the ASC as in the UH. Most incidents occurred during handling between surgical procedures. Future research is needed to examine the impact of training and certification of support staff on durability of DFUs.
Introduction
Flexible ureteroscopes are an integral part of the endourologist's armamentarium. Since its first description in 1964, the technology and technique of flexible ureteroscopy continues to evolve. 1 However, the durability of flexible ureteroscopes remains unchanged. In 1998, when the durability of the 7.5F Karl Storz and 7.0F Wolf flexible fiberoptic ureteroscope (FFU) was compared, the authors noted that both FFU required repair after an average of 12 uses. 2 Nevertheless, the number of ureteroscopies performed continued to rise. 3 Reusable digital flexible ureteroscopes (DFUs) present a further technological advancement and provide enhanced image quality and maneuverability compared with fiberoptic ureteroscopes. 4,5 The use of DFUs also decreases the operative time by 20% without compromising on stone-free rates. 6 It has been hypothesized that the absence of fragile fiberoptic bundles in DFUs might make them more durable than FFU. 7
Information regarding the durability of DFUs is limited to few studies that evaluated a limited number of damaged ureteroscopes. The number of uses also varied widely from 1 to 159 procedures with the average cost per procedure ranging from $492 to $1137. 8 –13 Although most upper urinary tract procedures in the United States are performed in ambulatory surgical center (ASC), there is no information about durability of DFUs in ASC setting. The information regarding the fragility of DFUs is important as it adds to the financial burden of the health care system. Hence, we sought to analyze manufacturer data on the location and cause of DFU damage and compared durability between a university hospital (UH) and an ASC. We believe that this study not only strengthens the existing knowledge and understanding of the locations and possible mechanisms of DFU damage but also provides a framework for devising strategies to improve durability. Besides providing data on the largest number of damaged DFUs, this study compares damages and durability of DFUs between UH and ASC. We also performed an in-depth review of the literature on DFU damages.
Materials and Methods
We reviewed the data of all ureteroscopic procedures performed using the Karl Storz Flex-Xc between January 2017 and December 2019 at our institution. The study was exempt from institutional review board approval as it did not involve human subjects. Procedures were either performed at the teaching UH, involving several attending surgeons, residents, fellows, and staff members, or at the University affiliated ASC, involving a limited number of surgeons and staff members. Residents and fellows were not involved in the procedures at the ASC. The procedures were scheduled between UH or ASC depending on the availability of surgical time and was independent of the complexity of the procedure.
The standard steps were followed during each procedure including but not limited to the routine use of ureteral access sheaths (UAS), single-use ball-tip 200 μm holmium laser fibers, repositioning lower caliceal stones, inserting the laser fiber or accessory devices in an undeflected DFU, and active removal of all stone fragments. The handling of DFU between cases was similar at both UH and ASC and sterilization was performed using a Sterrad® NX system at each location. There were fewer personnel involved in handling the instruments between cases at ASC compared with the UH. Patients undergoing bilateral simultaneous ureteroscopy were considered to have two uses of the DFU. The mean number of DFU uses was calculated by dividing the number of ureteroscopic procedures performed at a particular time period by the number of DFUs sent for repair during that period. The internal odometer readings regarding use of each DFU were unreliable as it was influenced by damage.
The manufacturer reports on the damaged DFUs were analyzed to elucidate the reason for return and the primary damage location. All damages except that which did not compromise the instrument's function or sterility were considered major damages by the manufacturer. In cases of multiple damages, the site of maximum damage was considered as the primary damage location. The possible mechanism of damage was determined by one of the authors (H.N.S.) after evaluating the detailed manufacturer report, photographs of each of the damaged ureteroscopes, and discussion with the field engineers. The mechanism of damage was classified as either intraoperative or during interoperative handling. We also determined the temporal trend in DFU damage to study the impact of training new residents on damage in UH.
The hospital has a risk-share agreement with the manufacturer for a monthly service charge that permits the hospital to pay the repair cost for a DFU each time a damaged ureteroscope is returned. The cost of DFU repair per procedure was calculated by dividing the repair cost by the mean number of procedures before damage. The damaged DFU was never used again and it was replaced each time with a new ureteroscope.
Statistical analysis was performed using STATA v16.0 (College Station, TX). Chi-square test was utilized to assess categorical variables. In addition, when cell frequencies was <5, Fisher's exact test was used. Value of p < 0.05 was considered significant.
Results
A total of 1211 flexible ureteroscopic procedures (947 in UH and 264 in ASC) were performed over a 3-year period. More laser lithotripsy and bilateral procedures were performed at the ASC (p = 0.001; Table 1). The mean number of uses at the UH and ASC were 7.45 and 16.50, respectively. The most common reason for return was a failed leak test (93%). Other causes for return were image loss (5.3%) and loss of deflection (1.7%). The most common site of primary damage was the angle cover at both locations and the difference was not statistically significant (Fig. 1). The majority of the damage at both locations (78%) occurred during interoperative handling rather than during procedures. The mechanism of intraoperative damage to DFUs included laser misfiring, application of excess torque, passage of the laser fiber through a deflected ureteroscope, and friction of the ureteroscope inside the UAS owing to surrounding stone fragments within the UAS (Fig. 2). Analysis of the temporal trend in DFU damage at the UH did not reveal any statistically significant difference in the number of repairs in each quartile (Fig. 3).
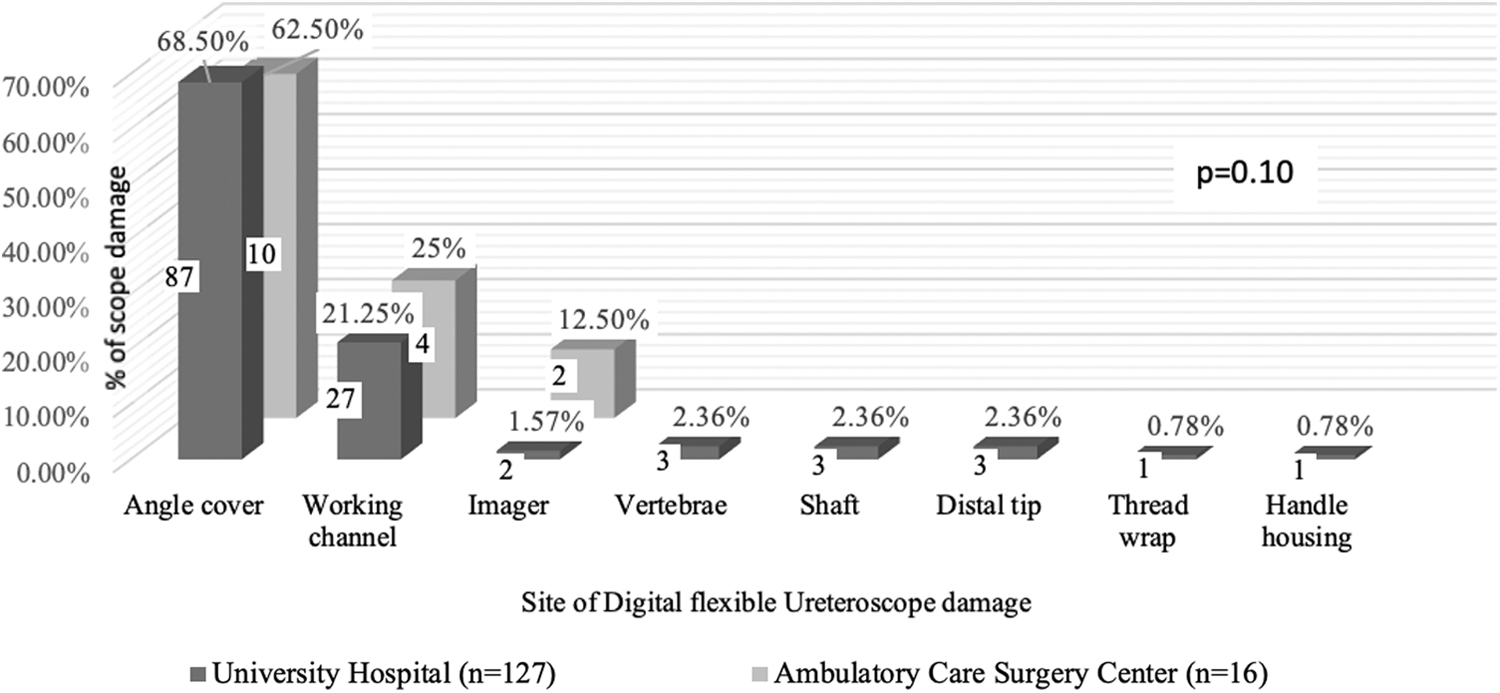
Primary site of digital flexible ureteroscope damage in University Hospital and Ambulatory Care Surgery Center.
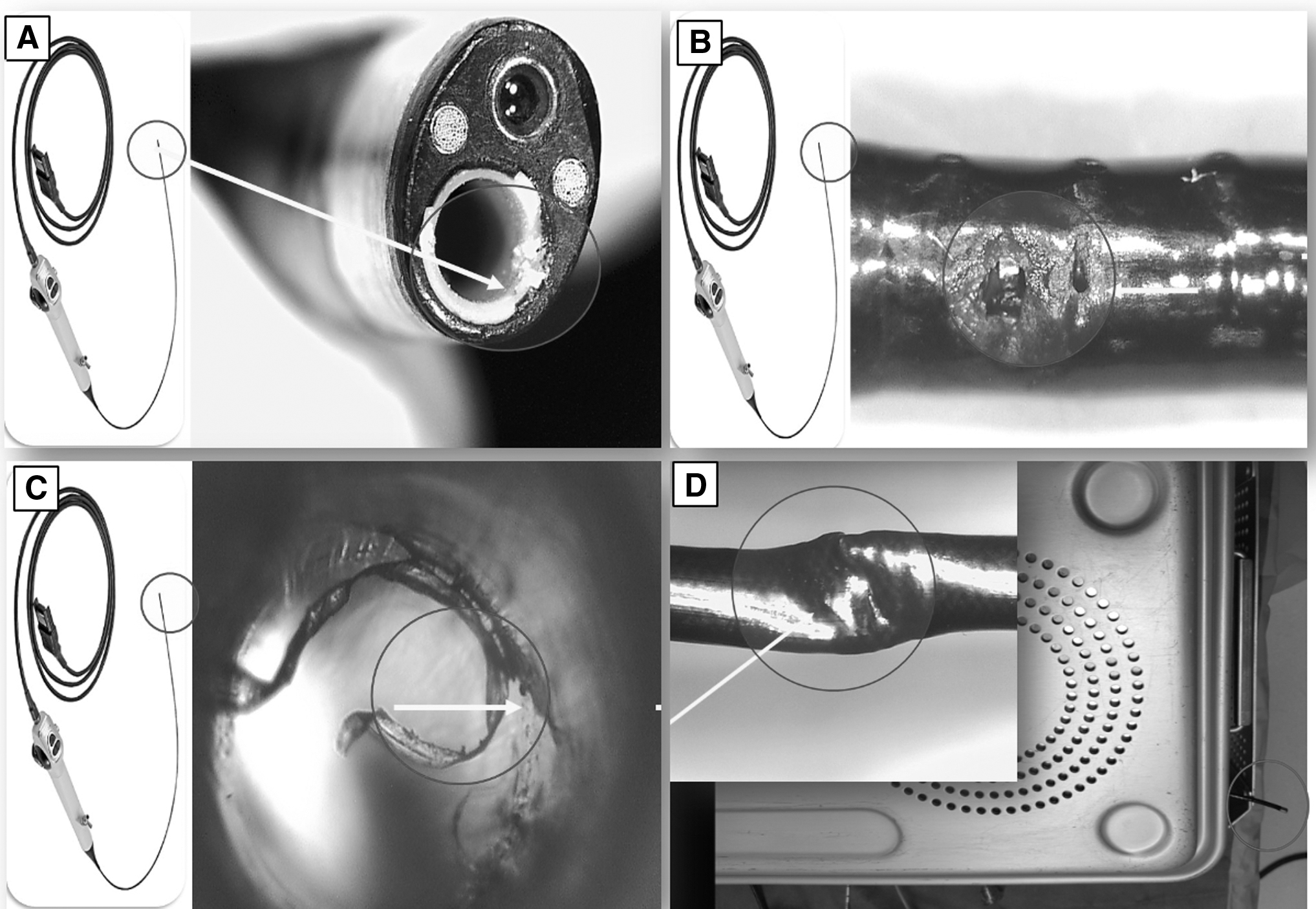
Various possible mechanisms of Digital flexible ureteroscope damages.
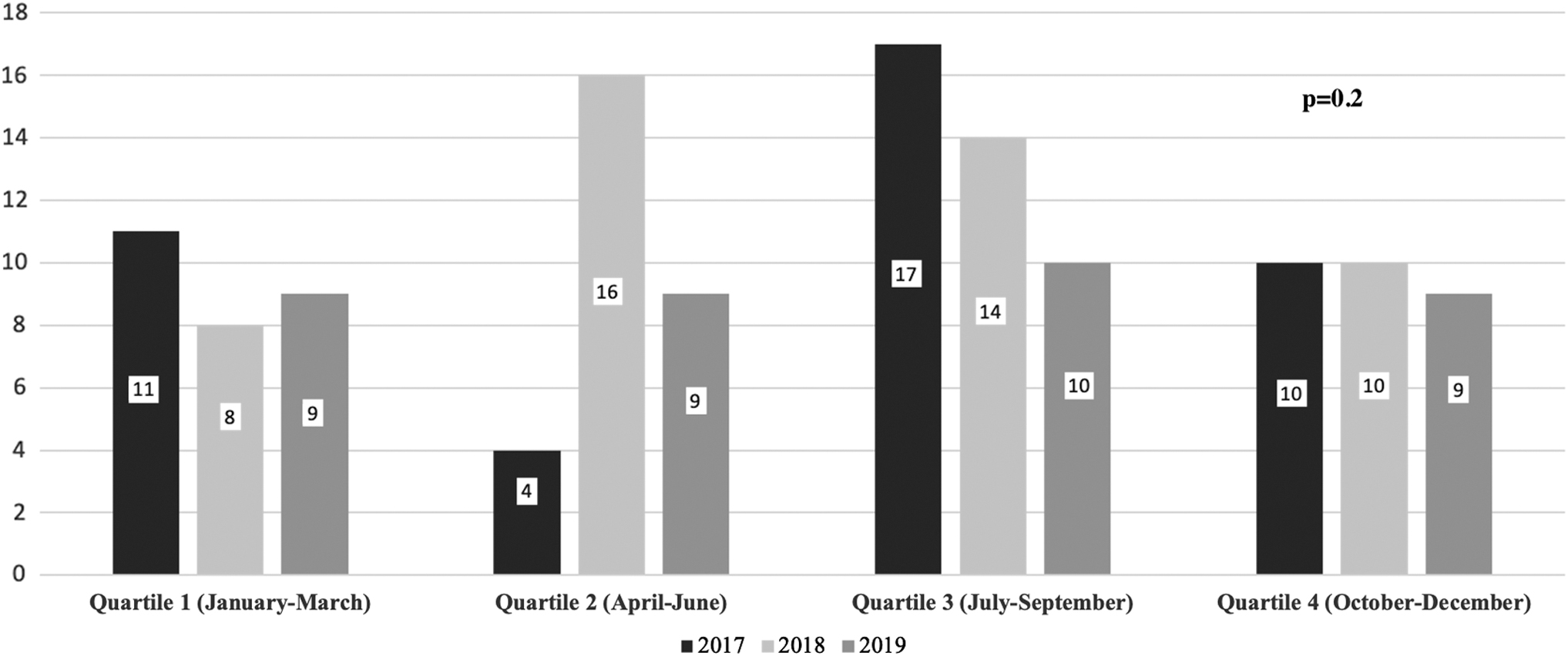
Digital flexible ureteroscope damage trend by quartile and year (2017–2019) in the University Hospital.
Type of Procedures Performed in University Hospital and University Ambulatory Care Surgery Center
p = 0.001.
UH = University Hospital.
The replacement cost was $9995 for major repairs and $328 for minor repairs. Only six ureteroscopes had minor damage, whereas all other DFUs were determined to have sustained major damage. The mean repair cost incurred per procedure was $1263 at the UH and $571 at the ASC.
Discussion
DFUs were initially considered more durable compared with their fiberoptic counterparts. 7,10 However, this was challenged by the observation that the number of uses of the Olympus DFU URF-V was 14 cases when compared with Olympus FFU URF-P5 of 18 cases. 14,15 The fact that the damage to a few fibers in FFU does not preclude its use can explain its longevity. In contrast, a DFU becomes nonfunctional if one component in the chain is compromised.
Our findings, that the angle cover is the most common site of damage (65%), are echoed by other authors who also noted that 51% of the evaluated Flex-Xc ureteroscopes had angle cover damage. 16 Over the past 2 years and in an attempt to minimize damage to the angle cover, the manufacturer has changed the orientation of grommets at the deflection angle. Grommets are now placed internally (and not externally) to decrease friction at this site and thereby increase the durability. In contrast to our observations, the common sites of DFU damage published in literature include the working channel, deflecting mechanism, distal vertebrae, shaft, and bending tube (Table 2). 9 –12,17 –19 Determination of the possible mechanism of DFU damage is challenging. Most authors noted that damages commonly occur within the working channel and are secondary to laser activation (43.59%) or to the deflection mechanism owing to a steep infundibulopelvic angle and extreme manipulation of the ureteroscope (75%). 9,18,20,21 On the contrary, we noted that 78% of the damage occurred in the interoperative period during handling, sterilization, and storage of the ureteroscopes. Our observations are similar to those of other authors who suggest that this damage can be minimized by appropriate training of support staff. 16,22 Upon employing dedicated trained urology staff for ureteroscope handling and sterilization, not a single episode of damage occurred to 11 prospectively used FFU processed 478 times. 23
Digital Flexible Ureteroscope Damages Literature Review
Also included fiberoptic ureteroscope damages for calculation.
The site of damage was not evaluated.
NA = not available.
On literature review, we noted that DFU was six times more durable in the nonteaching hospital or ASC compared with the teaching hospital. The mean number of uses was 97.53 cases in nonteaching hospitals compared with 15.92 in teaching hospitals (Table 2). One can submit that teaching hospitals are committed to training residents and serve as tertiary referral centers for managing patients with complex stones. It has been shown that the use of laser and treatment of complex stones has been associated with poor DFU durability. 12,16,19 The data from the ASC in our study closely resembled nonteaching urology practice as all the procedures were performed by the attending urologist with minimum staff involved in the handling and sterilization of the ureteroscope. Despite more ureteroscopy being performed for nephrolithiasis (80.67% vs 40.4%), the mean number of DFU use in our study at the ASC was more than twice that of the UH. This difference may be partly because of a higher rate of simultaneous bilateral ureteroscopy at ASC (7.95% vs 3.3%). Although a bilateral simultaneous procedure might increase intraoperative wear and tear of DFUs, the perioperative strain owing to processing and sterilization will not be doubled.
We initially attributed the durability of DFU to the absence of trainee involvement at the ASC. To study the impact of resident teaching on DFU durability, we further performed subgroup analysis of the damages at UH by quartile and year. We did not find any correlation between training incoming residents and damage to the DFUs. Our findings support the position that DFU damages are mostly unrelated to procedures if appropriate technical steps are adhered to. 16 The importance of implementing a systematic training process that incorporates simulation, observation, assisting, and performance of at least 5 procedures under guidance is demonstrated in a study revealing increased durability of DFUs from 11 to 22 procedures on adherence to a systematic credentialing process. 9
Previous studies have noted that DFUs are more durable when high-level disinfection (HLD) with Cidex® is used instead of sterilization (Table 2). When HLD of Flex-Xc using Cidex OPA was compared with sterilization using low-temperature hydrogen peroxide gas (Sterrad NX), the authors noted that Sterrad NX was nearly four times more expensive and caused almost twice as much damage to the ureteroscope compared with Cidex. 24 Similarly in FFU, HLD with Cidex was also found to cause less damage when compared with sterilization by Sterris 1. 25 Although Karl Storz Flex-Xc DFUs are validated by the US Food and Drug Administration (US-FDA) for both HLD and sterilization with Sterrad or V-PRO® method, the choice depends on national guidelines and/or hospital protocols. In the United States, the FDA maintains a list of high-level disinfectants that can be used to reprocess flexible endoscopes. 26 Our hospital policy does not permit the use of HLD.
Very few studies have investigated and determined the cost associated with DFU damage. 11 –13,17 Borofsky and colleagues provided a comprehensive analysis for Flex-Xc damage, including purchase, reprocessing, and repair cost, and found that the global cost per case was $1086. 17 Despite not including the initial purchase cost and reprocessing cost in this analysis, we found that the cost incurred per procedure at the UH ($1263) was much higher than these authors'. However, because of increase in durability, the cost per case was much lower in the ASC ($571). Of interest, on a review of the literature we noted that although the mean number of uses before damage of the ureteroscope was similar across all teaching hospitals (11–12.5), the cost per procedure varied widely ($492–$1086). This highlights the problems with calculating the cost as it depends on multiple factors including variability in repair or replacement contract between the manufacturer and the hospital. We never repaired a damaged DFU for reuse as performed elsewhere, because repaired ureteroscopes may be less durable than new ureteroscopes. 9,12
One may contend that our study is a single-center experience involving DFUs from only one manufacturer, thus limiting the generalization of the results to DFUs from other manufacturers. We however feel that this study design minimizes the potential for confounding factors. Other limitations include the retrospective nature of the study and lack of data regarding the complexity of the procedures. In our opinion, the validity of the findings is maintained as the DFU damage data were recorded prospectively by the manufacturer. The cost calculation was also not comprehensive and was based on the risk-share agreement model between the manufacturer and the institution. However, this finding might be applicable to other institutions with similar models. This study provides much needed data on DFU damage in community and nonteaching urology practice in the United States.
Over the last few years, various disposable ureteroscopes have been introduced and marketed to be more cost-effective. 12,27,28 This study is timely in this regard as it shows that most of the damage to DFUs is preventable. As such, before transitioning to a disposable ureteroscope, approaches to increase the longevity of reusable DFUs should be implemented. If DFUs can last an average 97.53 cases in nonteaching hospital, the onus of maximizing durability of DFUs in teaching hospitals is on the persons handling the instruments. We also observed that previous studies did not provide a comprehensive list of recommendations to increase the durability of DFUs. 9,10,18,19 Hence, after reviewing the available literature and manufacturer guidelines, we have compiled a comprehensive checklist to minimize DFU damage (Supplementary Appendix SA1). Because most of the damage to DFU is preventable, we plan to initiate a mandatory certification curriculum for residents, fellows, and support/instrument handling staff on DFU handling. We will also examine the impact of these strategies on durability of DFUs in near future.
Conclusion
We conclude that DFUs were more than two times more durable in the ASC setting than in the UH. We noted that most of the damages to DFUs occurred at the angle cover and happened during handling between surgical procedures. Future research is needed to examine the impact of training and certification of support staff on the handling and sterilization process on durability of DFUs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding information was received.
Supplementary Material
Supplementary Appendix SA1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.