
Abstract
Background:
Partial nephrectomy (PN) is the standard of treatment in patients with cT1 renal tumors. Current guidelines recommend PN as a standard of treatment in patients with cT1 renal tumors. However, the commonly accepted criteria for which surgical outcomes are evaluated both functionally and oncologically are not yet clear. The aim of this study was to evaluate compounding factors that affect the operative and functional outcomes for laparoscopic partial nephrectomy (LPN) in patients with cT1 renal tumors.
Methods:
This study was registered at NCT04213157 for patients who underwent LPN with the diagnosis of clinical T1 renal tumors. Between November 2009 and August 2018, 292 patients were included in the study. The patients were allocated into two groups according to the tumor size: T1a (n = 215) and T1b (n = 77). Demographic features, clinical tumor characteristics, and intraoperative and postoperative outcomes were analyzed. A negative surgical margin, warm ischemia time of <20 minutes, and no postoperative major complications were accepted to achieve the trifecta outcomes. Pentafecta was defined as trifecta criteria plus >90% preservation of baseline renal function (RF) and no stage upgrade of chronic kidney disease at 12 months after surgery. Univariate and multivariate analyses were used to identify factors predicting trifecta and pentafecta.
Results:
Preoperative variables including age, gender, and baseline RF were similar between the two groups. The warm ischemia time was 13.4 vs 15.9 minutes (P = 0.001). The positive margin rate was 0.9% vs 2.6% (P = 0.284), and the major complication rate was 3.3% vs 2.6% (P = 0.548). The achievement of the trifecta rate was 88.4% vs 75.3% (P = 0.006) and pentafecta rate was 72.6% vs 42.9% (P = 0.001). Multivariate analysis showed that tumor complexity, baseline RF, and diabetes mellitus are independent predictors of achieving pentafecta outcomes.
Conclusion:
LPN is an effective and reliable method for renal tumors even in T1b with satisfying surgical and functional outcomes.
Introduction
The main goal of partial nephrectomy (PN) is to reduce the incidence of chronic kidney disease (CKD) and subsequently prevent cardiovascular mortality. Current guidelines recommend PN in patients with renal tumors ≤7 cm as a standard procedure whenever it is technically feasible. 1 However, the majority of patients with large renal tumors (4–7 cm) are still treated with radical nephrectomy (RN). 2 Thereby, the efficacy and safety of PN in the management of them are still controversial.
Trifecta is an assessment of the short-term outcomes following PN that was described by Buffi and colleagues for the first time using margins, ischemia, and complication system. The definition refers to the criteria of having a negative surgical margin (NSM), warm ischemia time (WIT) <20 minutes, and no postoperative complication of grade 3. 3 Besides, pentafecta is a novel definition that includes the >90% preservation of renal function (RF) and no stage upgrading of CKD at 12 months postoperatively in addition to the trifecta outcomes. 4
In this study, we aimed to compare trifecta and pentafecta outcomes in patients with clinical T1a and T1b renal tumors who underwent laparoscopic partial nephrectomy (LPN). Patient, surgical, and tumor-specific variables were also evaluated to predict the achievement of trifecta and pentafecta outcomes following LPN. To the best of our knowledge, it is the first single-center study that evaluates the predictive factors to achieve both trifecta and pentafecta outcomes in a standard cohort following LPN.
Materials and Methods
Medical records on 395 patients with the complete data who underwent LPN from November 2009 to August 2018 were retrospectively evaluated. Patients with bilateral renal tumors (n = 8), solitary kidney (n = 8), horseshoe kidney (n = 4), pelvic ectopic kidney (n = 2), allograft kidney (n = 2), and those with multiple renal tumors in a single kidney (n = 3) or with >7 cm renal tumor (n = 6) were excluded. Patients who were operated on for colon cancer (n = 4), prostate cancer (n = 2), endometrial cancer (n = 1), or adrenal mass (n = 2) within the first year after LPN were also excluded. Finally, patients managed with different LPN techniques such as off-clamp (n = 36) or selective arterial clamping (n = 16) were excluded from the study as well. Two hundred ninety-two patients who have a follow-up of at least 12 months were included in the study. Those patients were allocated into two groups according to tumor size: 215 patients with tumor size ≤40 mm were included in T1a group and 77 patients with tumor size 41–70 mm were included in T1b group.
The demographics of patients including age, sex, body mass index, and systemic diseases as well as the clinical tumor characteristics' such as tumor size, and side were recorded. The tumor complexity was evaluated by RENAL nephrometry score (RNS). 5 All LPNs were performed by one surgeon (E.O.). Intraoperative and postoperative variables including operation time (OT), WIT, estimated blood loss (EBL), preoperative and postoperative hemoglobin (Hgb) values, perioperative complications, length of hospital stay, final pathology, and surgical margin status were recorded. Complications that occurred within the 3 months postoperatively were graded according to the Clavien–Dindo classification system. 6 Using the CKD Epidemiology Collaboration (CKD-EPI) equation, the estimated glomerular filtration rate (eGFR) was used for the assessment of RF. 7 Patients were stratified from 1 to 5 before and 1 year after surgery according to their eGFR values to one of the CKD stages.
The reliability and effectiveness of LPN were assessed in short- and long-term by using trifecta and pentafecta outcomes. Obtaining an NSM, WIT <20 minutes, and the absence of major postoperative complications (Clavien–Dindo ≥ grade 3) was accepted to achieve the trifecta outcomes. 3,8 Pentafecta was defined as trifecta criteria plus >90% preservation of total eGFR and no stage upgrade of CKD from preoperative values 12 months after LPN. 4
Statistical analysis
The data were analyzed using Statistics Package for Social Sciences version 24 (IBM SPSS®, Armonk, NY). Independent sample t-test was used for comparison of normal distribution parameters, and the Mann–Whitney U test was used for parameters that had nonnormal distribution. The chi-square test was used to analyze categorical variables according to groups. The effect of time and groups on eGFR change was analyzed by two-way analysis of variance. The independent risk factors affecting the achievement of trifecta and pentafecta were analyzed by binary (logistic) regression analysis as both univariate and multivariate. Correlations between normally distributed data of WIT and RNS were assessed using the Pearson correlation coefficient (r). Analysis results are presented as mean ± standard deviation (SD) for the quantitative and normal distribution data, and all categorical data are presented as frequency (percentage). The significance level was taken as P < 0.05.
Results
Our analysis included 292/395 (73.9%) patients with the complete data who underwent LPN. Of these, 215 (73.6%) patients with tumor size ≤40 mm were included in the T1a group and 77 (26.4%) patients with tumor size 41–70 mm were included in the T1b group. The mean age was 56.9 ± 13.5 (18–86) and 55.1 ± 12.1 (24–82) years in the T1a and T1b groups, respectively. There was a statistical difference between the T1a and T1b groups according to tumor complexity including tumor size and RNS as expected. The demographic features of patients and clinical tumor characteristics are shown in Table 1. The distribution of the number of patients in the study cohort by years is shown in Figure 1.
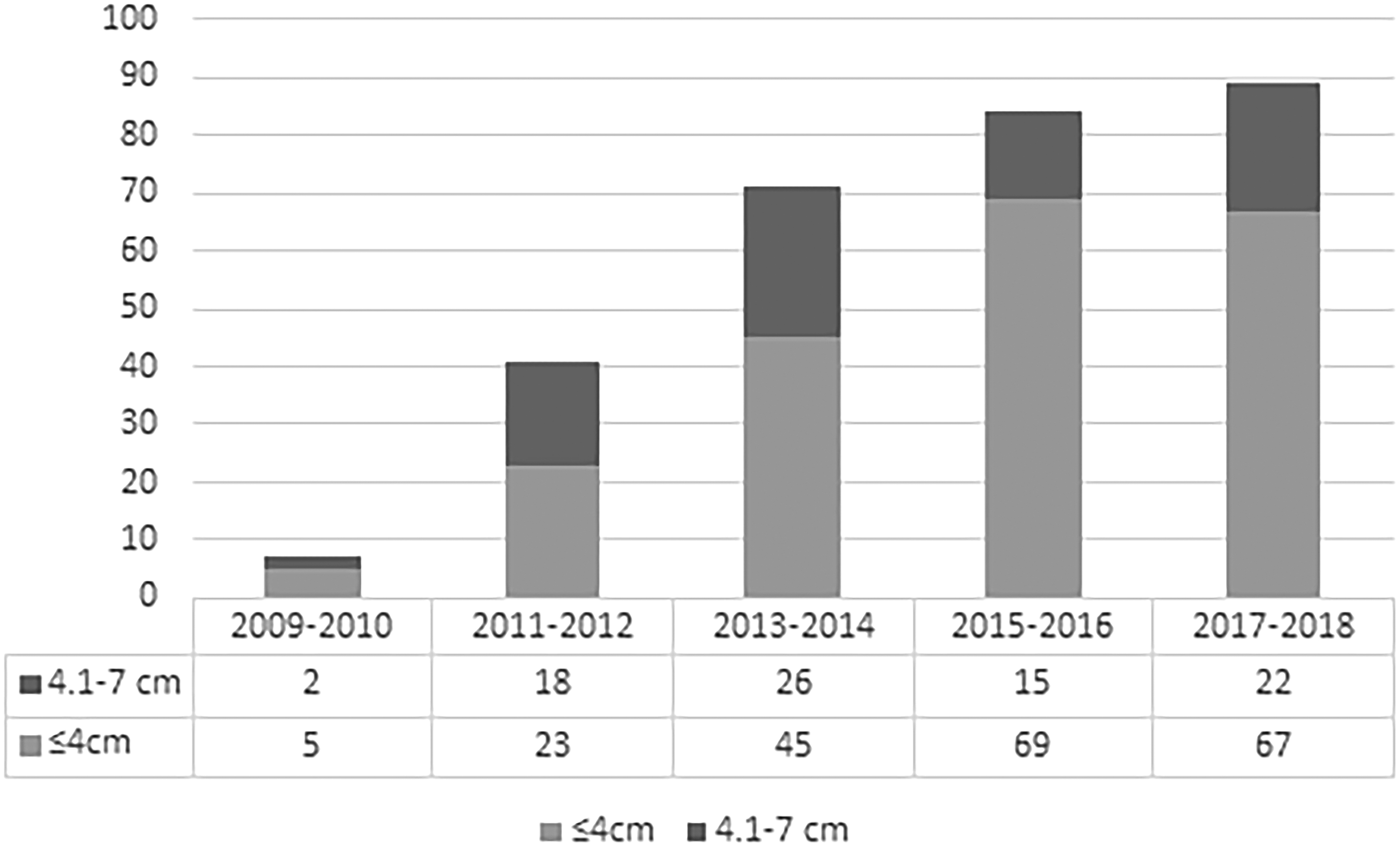
The number of the study cohort for patients with cT1 renal tumor undergoing LPN from November 2009 to August 2018. LPN, laparoscopic partial nephrectomy.
Demographic and Clinical Tumor Characteristics
Continuous variables are presented as mean ± SD, and categorical variables are presented as number (%).
ASA, American Society of Anesthesiologists; BMI, body mass index; CAD, coronary artery disease; DM, diabetes mellitus; HT, hypertension; RNS, RENAL nephrometry score.
Intraoperative and postoperative outcomes are demonstrated in Table 2. The T1b group had a higher OT, WIT, and EBL. The T1a and T1b groups had similar intraoperative complication rate (2.8% vs 2.6%, P = 0.929) and overall postoperative complication rate up to 3 months (8.8% vs 11.7%, P = 0.466). Postoperative major complications were detected in 7 (3.3%) patients in the T1a group and in 2 (2.6%) patients in the T1b group. Four patients in the T1a group and one patient in the T1b group underwent angioembolization due to arteriovenous fistula or ongoing hematuria. Three patients in the T1a group underwent a Double-J stent insertion for urinary extravasation. RN was performed in one patient of the T1b group because of renal vein thrombosis in the postoperative third month. NSM rate was 99.1% (213/217) and 97.4% (75/77) in the T1a and T1b groups, respectively. The relative decrease in eGFR <10% was achieved in 172 (80%) patients in the T1a group and in 49 (63.6%) patients in the T1b group (P = 0.004). However, the mean relative decrease in eGFR after the first year of surgery was 7.1% ± 8.9% in the T1a group and 9.1% ± 8.4% in the T1b group (P = 0.094). Although, the rate of CKD upstaging was found 23.3% of the overall cohort, new-onset stage IV CKD (GFR <30 mL/min) was only detected at 2.1% of those.
Intraoperative and Postoperative Variables
Continuous variables with normal distribution are presented as mean ± SD, and categorical variables are presented as number (%).
Continuous variables with nonnormal distribution are presented as median (IQR).
AML, angiomyolipoma; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; Hgb, hemoglobin; IQR, interquartile range; LOS, length of hospital stay; RCC, renal-cell carcinoma.
The main effects of the T1a and T1b groups were significant when comparing GFR changes over time according to groups (P < 0.001). The mean eGFR value was higher in the T1a group than in the T1b group. The time effect was also statistically significant (P < 0.001). However, group and time interaction was not statistically significant (P = 0.790). The statistical outcomes of time and group interaction on eGFR are summarized in Table 3 and Figure 2.
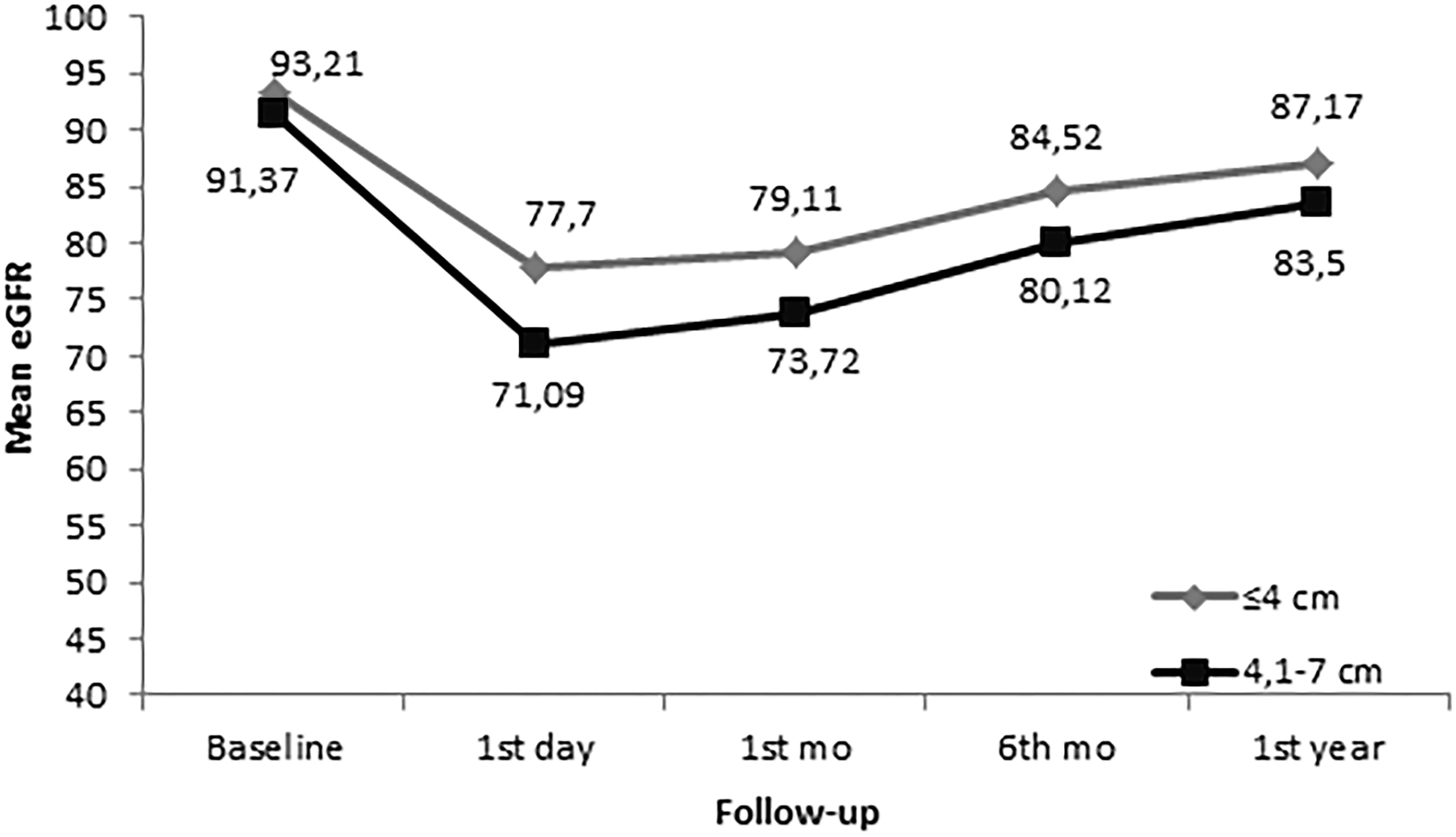
The mean eGFR changes over time for the T1a and T1b groups have been shown. Group–time interaction in terms of renal function was found to be statistically similar between the two groups. eGFR, estimated glomerular filtration rate.
Comparison of Estimated Glomerular Filtration Rate Changes According to T1a and T1b Tumor Groups
Postoperative time periods.
1, descriptive statistics; 2, the result of general linear model analysis.
Different lowercase letters show a significant difference between groups and time by the Bonferroni test.
Achieving trifecta outcomes was higher in the T1a group compared with the T1b group (88.4% vs 75.3%, P = 0.006, respectively). The increase in the complexity of tumors has a negative effect on achieving trifecta outcomes in the univariate analysis. The only variable that was identified as a statistically significant risk factor for trifecta outcomes in multivariate analysis was RNS (Table 4). Besides, WIT and RNS are subjected to the Pearson correlation analysis. WIT was detected to be positively correlated with RNS (r = +0.38; P < 0.0001).
Associations of Preoperative Patient and Tumor Characteristics with Trifecta After Laparoscopic Partial Nephrectomy
Bold indicates statistical significance level at P < 0.05.
Ref. Cat: age <70 years.
OR, odds ratio; CI, confidence interval.
Achieving pentafecta rates was also significantly higher in the T1a group than in the T1b group (72.6% vs 42.9%, P = 0.001, respectively). The increase in RNS has a negative effect on achieving pentafecta outcomes in the univariate analysis. In contrast, the higher baseline RF was found to be a positive predictive factor for pentafecta outcomes in univariate analysis. Moreover, RNS, the lower baseline RF, and the presence of diabetes mellitus (DM) were identified as significant risk factors for pentafecta outcomes in multivariate analysis (Table 5).
Associations of Preoperative Patient and Tumor Characteristics with Pentafecta After Laparoscopic Partial Nephrectomy
Bold indicates statistical significance level at P < 0.05.
Ref. Cat: age <70 years.
Ref. Cat: DM (yes).
The overall survival rate was 97.3% in the cohort. It was found comparable as 98.6% and 93.5% in the T1a and T1b groups, respectively (log-rank test, P = 0.055).
Discussion
In this study, a total of 292 patients with renal tumors underwent LPN with global ischemia. There were 215 (73.6%) patients with ≤40 mm and 77 (26.3%) patients with 41–70 mm renal tumor. Trifecta and pentafecta outcomes have achieved 190 (88.4%) vs 58 (75.3%) (P = 0.006) and 156 (72.6%) vs 33 (42.9%) (P = 0.001), respectively, in the T1a and T1b groups.
Trifecta is a marker of the endpoints we aim for in PN. In fact, the main goal is to preserve RF as much as possible and to obtain a better survival outcome. Nevertheless, surgically induced CKD is an isolated event and has a limited functional decline and less impact on survival compared with CKD associated with medical disorders. There are a variety of trifecta definitions available in the literature by different authors; the only common criterion in all definitions is to achieve an NSM. The other components of the concept such as complications, WIT, or postoperative evaluation of RF are not clear. The overall trifecta rates in the LPN series vary between 31.6% and 74.3% in the literature. 8 –10 The dissimilarity is caused by a wide range of circumstances such as heterogeneity of patient cohort, differences in surgical techniques, and the different definitions of the trifecta as well as the surgeon's experience. In a recent study, it has stated that while more PN has been performed in patients with T1 renal tumors in the centers with high surgical volume, the complication rate has an inverse correlation with hospital volume; however, patients have better outcomes. 11
One of the limiting factors for the evaluation of the quality of LPN is the difference in the assessment of complications. 3,4,8 The most common postoperative complications are bleeding and urine leakage with a reported incidence of 10% and 5%, respectively. 12 Nevertheless, in the very first retrospective studies that presented the initial experience of the experienced surgeons, LPN for patients with larger renal tumors (>4 cm) was reported to have increased postoperative complication rates and/or in WIT. Rais-Bahrami and colleagues compared the outcomes of LPN in patients with T1a and T1b renal tumors. The postoperative complication rate was 37% in patients with tumors >4 cm vs 21.8% in the others (P = 0.039). 13 In our study, the postoperative complication rate was found to be slightly higher in the T1a group. We consider that it is related to the learning curve and the surgeon's experience. When our cohort is evaluated by chronological order, it is determined that in the early phase of the learning curve that patients with smaller tumors underwent LPN. However, those with larger tumors have been managed laparoscopically with increased surgical experience. This consideration is compatible with the previous literature. 8
Preservation of RF as much as possible after PN is crucial for functional outcomes. Mir and colleagues concluded that the RF loss of the operated kidney after PN is ∼20%. This loss is attributed to the ischemic insult on the remaining kidney and loss of nephron during tumor resection or renal reconstruction. In patients with a contralateral healthy kidney, the global renal functional decline is ∼10% due to the compensatory role of the normal kidney. 14 Furthermore, Choi and colleagues 15 and Porpiglia and colleagues 16 showed that increased WIT severely alleviated RF in the operated kidneys in the early postoperative period. Although the affected kidneys had a recovery period of 3 months to 1 year, it was observed to occur at a lower rate in the kidneys where the specified ischemia time was prolonged. The optimal threshold of WIT to preserve functional impairment following PN is still controversial. However, in the recent studies in which trifecta outcomes were evaluated, they accepted the threshold value for WIT as 20 minutes. 10,17 In our study, we used 20 minutes for WIT as a surrogate marker of RF preservation, and WIT has been found to be positively correlated with RNS. Porpiglia and colleagues assessed 206 patients with renal tumors who underwent LPN. The overall trifecta rate was reported as 63.1%, and it increased progressively from 24.9% to 84.9% with increasing surgical experience; however, tumor complexity has an inverse correlation with trifecta achievement. 8 In our study, the only variable that was also identified as a negative predictive factor for trifecta outcomes in multivariate analysis was RNS.
The risk of prolonged ischemia for irreversible kidney damage as well as the loss of nephron volume may be associated with functional decline at any rate following PN. Renal functional recovery after PN is strongly associated with baseline RF, and the quality and quantity of renal parenchyma preserved. Nonetheless, WIT >25 is a crucial surrogate that adverse postoperative RF. 18 Current literature suggests the threshold of 90% preservation of eGFR and no CKD upstaging 1 year after PN for the evaluation of long-term functional outcome. 4,19 Therefore, pentafecta outcomes could be considered in evaluating the long-term outcomes in a precise manner after PN. However, no LPN series evaluated pentafecta outcomes in the literature.
A recent study has stated that the prognostic risk of CKD is increased when the baseline RF is <60 mL/min (CKD stage 3A) or the RF is <45 mL/min (CKD stage 3B) in patients with renal tumor undergoing surgical treatment. 20 In our study, although CKD stage upstaging has found to be higher in the T1b group 1-year following LPN, patients with new-onset CKD stage IV (<30 mL/min) were found to be comparable to the T1a group (1.9% vs 2.6%, P = 0.696). Castellucci and colleagues have compared trifecta and pentafecta in patients with renal tumors <4 cm vs ≥4 cm who underwent robot-assisted partial nephrectomy. Trifecta was achieved at 72.9% vs 44.7% (P < 0.01). Pentafecta was achieved at 23.5% vs 10.5% (P = 0.08). The authors found no significant predictive factors for trifecta and age as a predictive factor for pentafecta. 21 In a similar study that was conducted by Kim and colleagues, it was reported that WIT was higher in the T1b group. However, the T1a and T1b groups were found to be comparable in PSM and overall complication rate. While the trifecta rate was higher in the T1a group (65.3% vs 43.3%, P = 0.017), the pentafecta rate has found to be similar (38.3% vs 26.7%, P = 0.172). Tumor size and OT were predictive of trifecta achievement. Tumor complexity has been stated as the only factor that predicts pentafecta achievement on multivariable analysis. 22
According to the existing literature, the use of pentafecta criteria and the quality of PN outcomes provide a stricter and more objective assessment, although there are differences in identification. We may state that the outcomes of our study are comparable with the previous studies. 21 –23 Age, gender, comorbidities, and baseline RF are not predictive factor for trifecta. However, RNS has found a major predictor for both trifecta and pentafecta. Additionally, lower baseline RF and the presence of DM are the negative predictors for pentafecta outcomes.
The present study and findings were limited by the retrospective analysis of the prospectively maintained database, single-center, and single surgeon experience that limited in terms of generalization and reproducibility of the outcomes. However, it may be considered that a single surgeon experience may help standardization of surgical techniques and postoperative outcomes. As with other similar studies, selection bias that may affect functional and oncological outcomes is another limitation. However, we included only patients who have a single renal tumor that managed by the global PN technique to improve the accuracy of renal functional outcomes. The strength of the study may be considered as the assessment of pentafecta outcomes of patients who underwent an LPN. A similar assessment was not previously available in the literature.
Conclusions
The present study revealed that tumor complexity is a crucial predictor of both trifecta and pentafecta outcomes in LPN for clinical T1a and T1b tumors. LPN is an effective and reliable method for renal tumors >4 cm as long as all efforts are made to minimize the duration of WIT.
Footnotes
Compliance with Ethical Standards
Authors' Contribution
M.N.M.: conception and design, acquisition of data, statistical analysis, and drafting of article. E.O.: conception and design, statistical analysis, critical revision of the article, and supervision. M.G.: acquisition of data, statistical analysis, and drafting of article. Y.B.: acquisition of data and drafting of article. Y.K.Y. and S.S.: conception and design, critical revision of the article, and supervision.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received for this article.