
Abstract
Background:
To summarize the current evidence on robot-assisted radical cystectomy (RARC) with intracorporeal urinary diversion (ICUD) and compare perioperative outcomes and postoperative complications of patients undergoing RARC with extracorporeal urinary diversion (ECUD) and ICUD.
Patients and Methods:
Through a systematical search of multiple scientific databases in March 2020, we performed a systematic review and cumulative meta-analysis of the primary outcomes of interest. Also, we assessed the quality of the relevant evidence according to the framework in the Cochrane Handbook for Systematic Reviews of Interventions.
Results:
Thirteen studies with 4696 participants were included in this review. No significant differences were found between the ECUD and ICUD in operation time (OT) (mean difference [MD]: −6.45, 95% confidence interval [CI]: −35.20 to 22.30), length of stay (MD: 0.36, 95% CI: −0.81 to 1.54), 30-day overall complications (odds ratio [OR]: 0.92, 95% CI: 0.60–1.41), 30-day minor complications (OR: 1.36, 95% CI: 0.85–2.19), 30-day major complications (OR: 0.70, 95% CI: 0.34–1.43), 90-day overall complications (OR: 1.34, 95% CI: 0.83–2.18), and major complications (OR: 1.03, 95% CI: 0.68–1.57). However, less estimate blood loss (MD: 99.28 mL, 95% CI: 62.59–135.98), lower intraoperative blood transfusion (OR: 1.80, 95% CI: 1.09–2.95), shorter oral intake time (MD: 0.78, 95% CI: 0.43–1.14), and 90-day minor complications (OR: 1.72, 95% CI: 1.08–2.73) were associated with ICUD. The subgroup analysis showed less estimated blood loss (MD: 149.73, 95% CI: 21.33–278.13) and less OT (MD: 32.45, 95% CI: 14.37–50.53) were found in ICUD.
Conclusions:
The ICUD is a safe and feasible alternative to ECUD, which decreases the need for blood transfusion and reduces 90-day complications. However, further quality studies are needed to evaluate effectiveness of ICUD and its oncologic outcomes, functional outcomes, cost, and the quality of life.
Introduction
At present, radical cystectomy is the standard treatment for localized muscular invasive bladder cancer, including open radical cystectomy (ORC), laparoscopic radical cystectomy, and robot-assisted radical cystectomy (RARC). 1 Over the past decades, RARC has become more popular because of less complications, more lymph node yields, less estimated blood loss (EBL), and shorter length of stay (LOS). 2 But there is similar in postoperative quality of life for patients undergoing RARC and ORC. 3 Therefore, RARC with intracorporeal urinary diversion (ICUD) has become a hot topic, to reduce postoperative complications and improve postoperative quality of life.
Many studies have shown that RARC with ICUD is safe and practicable. 4 –6 Furthermore, the studies comparing RARC with extracorporeal urinary diversion (ECUD) and ICUD procedure have been reported. 7 Hence, we performed a systematic review and meta-analysis to discuss the effectiveness of ICUD compared to ECUD in patients with bladder cancer.
Patients and Methods
Literature search
A systematic literature search was performed in March 2020 using PubMed, the Cochrane Library, and EMBASE databases. Search terms combined participant terms (bladder cancer or bladder neoplasm), intervention terms (robot-assisted radical cystectomy or robotic radical cystectomy), and comparison terms (ICUD, and ECUD). There were no restrictions to publication language and date. Besides, we also manually retrieved references, which come from relevant studies by using PubMed database.
The studies focused on patients with bladder cancer who underwent RARC and compared surgical outcomes between ICUD and ECUD were included. On the contrary, we did not include letters, cases, reviews, conference abstracts, and studies which are irrelevant to the theme or lack complete data.
Data extraction
A form was used to collect the data of interest. The author, publication year, study design, participant characteristics (age, male: female, Body Mass Index, American Society of Anesthesiologists scores, diversion type), operation time (OT), EBL, intraoperative blood transfusion, oral intake time, LOS, and postoperative complications were collected whenever available. Also, all complications were recorded, defined, and graded according to Clavien system. 8
Quality assessment
Based on our search results, the included studies quality was evaluated according to the Newcastle–Ottawa scale (NOS). 9 The total score of the NOS ≥7 is considered as high quality. In addition, the corresponding level of evidence for each outcome was assessed according to the framework in the Cochrane Handbook for Systematic Reviews of Interventions. 10 Meanwhile, the risk of bias of each study included were independently assessed using the Risk of Bias in Non-Randomized Studies–of Interventions tool (ROBINS-I) for comparative studies. 11
The above steps were completed by two of us (C.Y. and L.P.) independently. All disagreements were resolved by a senior author (A.W.) after public discussion.
Statistical analysis
The Review Manager software (RevMan) Version 5.3. was used for statistical analysis in our study. The mean difference (MD) and odds ratio (OR) were calculated for continuous and dichotomous variables, respectively, with 95% confidence intervals (CIs). The heterogeneity between studies was assessed by using the chi-squared and I- squared test. Random-effects models were used for cumulative analyses, which were of high heterogeneity (I 2 > 50%). Otherwise, fixed-effects models were used.
A subgroup analysis of pairwise comparison was performed for RARC with ileal conduit urinary diversion. Finally, p-value of <0.05 was considered as a statistical significance.
Results
Initially, a total of 709 studies were identified by our search strategy. After excluding duplication, irrelevant records, and low-quality studies, the remaining 13 studies were included in our meta-analysis. 12 –24 The specific process is shown in Figure 1. The characteristics of included studies are shown in Table 1. All included studies were of high quality because their scores were ≥7 (NOS), also shown in Table 1 for details.
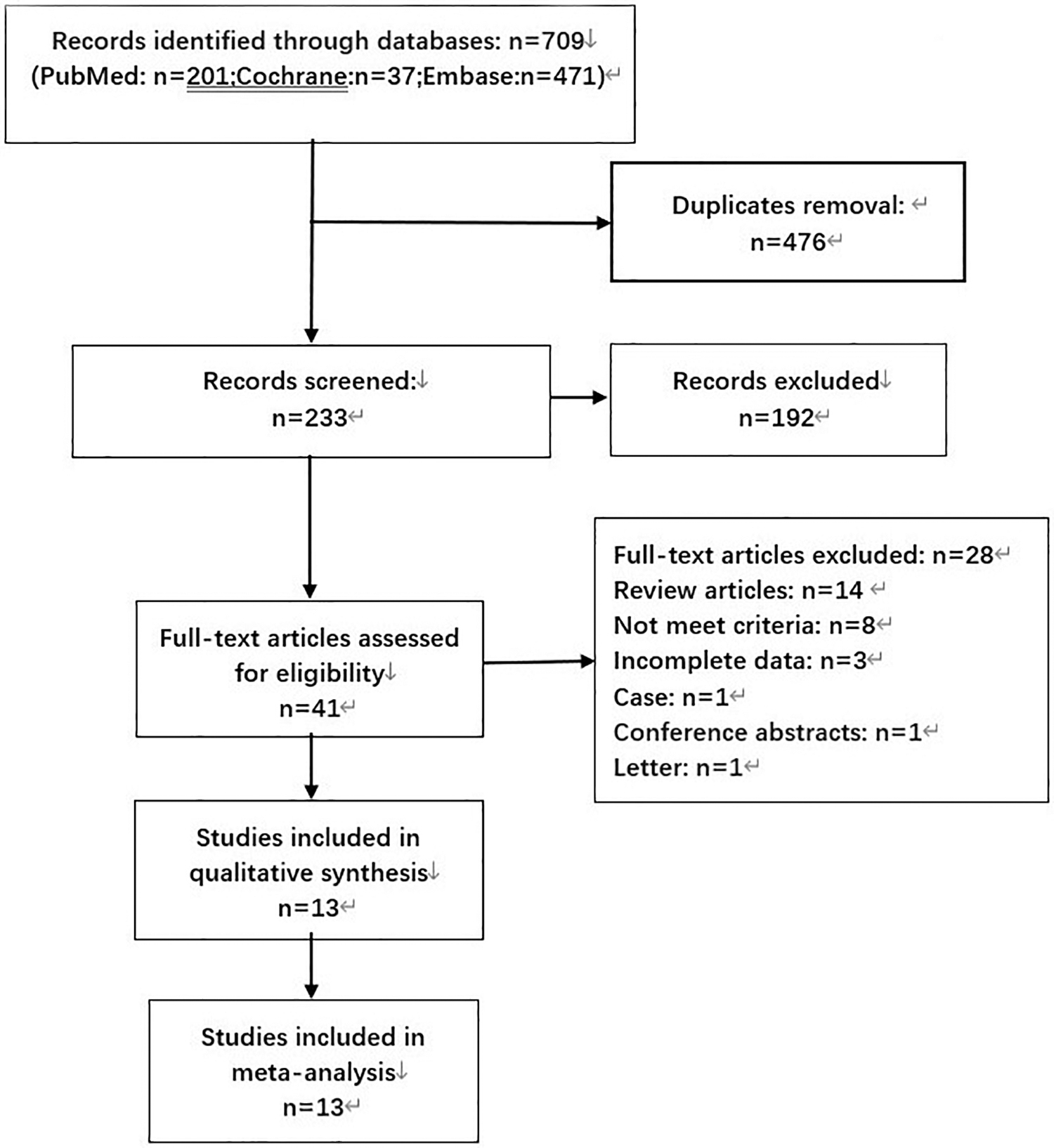
PRISMA flow diagram.
Characteristics and Quality Assessment of Included Studies
Mean ± standard deviation.
Mean.
Median (interquartile range).
Mean (range).
Male:female.
Number of ASA score ≥3.
Using Newcastle–Ottawa scale scoring rules.
ASA = American Society of Anesthesiologists; BMI = body mass index; NA = not available; RARC-ECUD/RARC-ICUD = robot-assisted radical cystectomy with extracorporeal urinary diversion/robot-assisted radical cystectomy with intracorporeal urinary diversion.
Risk of bias
An included study 17 was found to have a high risk of bias (selection of the patients, performance bias, and observer bias of outcomes) according to the ROBINS-I tool, and the remaining 12 studies had a moderate risk of bias.
Perioperative outcomes
There was no statistical difference between the EUCD and ICUD for OT (MD: −6.45, 95% CI: −35.20 to 22.30, p = 0.66, Fig. 2A). The quality of evidence was low (high heterogeneity and wade CIs). However, a less EBL (MD: 99.28, 95% CI: 62.59–135.98, p < 0.00001, Fig. 2B) and a lower blood transfusion (OR: 1.80, 95% CI: 1.09–2.95, p = 0.02, Fig. 2C) were associated with ICUD. The quality of evidence for both EBL and transfusion was moderate.

Forest plot and meta-analysis of operation time
Prognostic outcomes
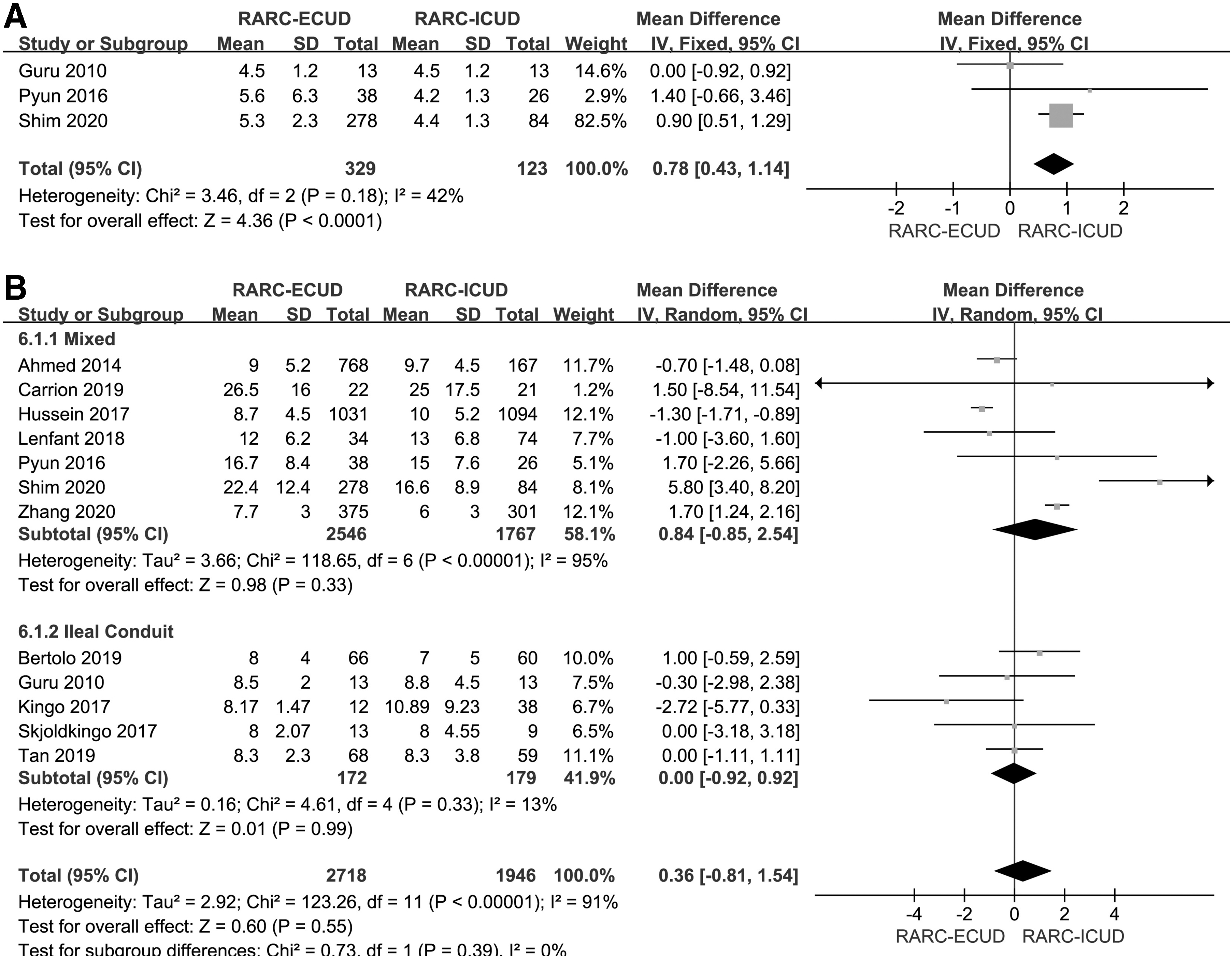
A shorter oral intake time was related to ICUD (MD: 0.78, 95% CI: 0.43–1.14, p < 0.001, Fig. 3A). The quality of evidence was low (small sample size). For LOS, all studies showed that the difference between ECUD and ICUD was not significant (MD: 0.36, 95% CI: −0.81 to 1.54, p = 0.55, Fig. 3B). The quality of evidence was moderate.
Forest plot and meta-analysis of oral intake time
Complications
We, respectively, analyzed the overall complications, minor complications (Clavien grade I–II), and major complications (Clavien grade III–V). No significant differences between two procedures were found for 30-day overall complications (OR: 0.92, 95% CI: 0.60–1.41, p = 0.71, Fig. 4A), minor complications (OR: 1.36, 95% CI: 0.85–2.19, p = 0.20, Fig. 4B), and major complications (OR: 0.70, 95% CI: 0.34–1.43, p = 0.32, Fig. 4C).
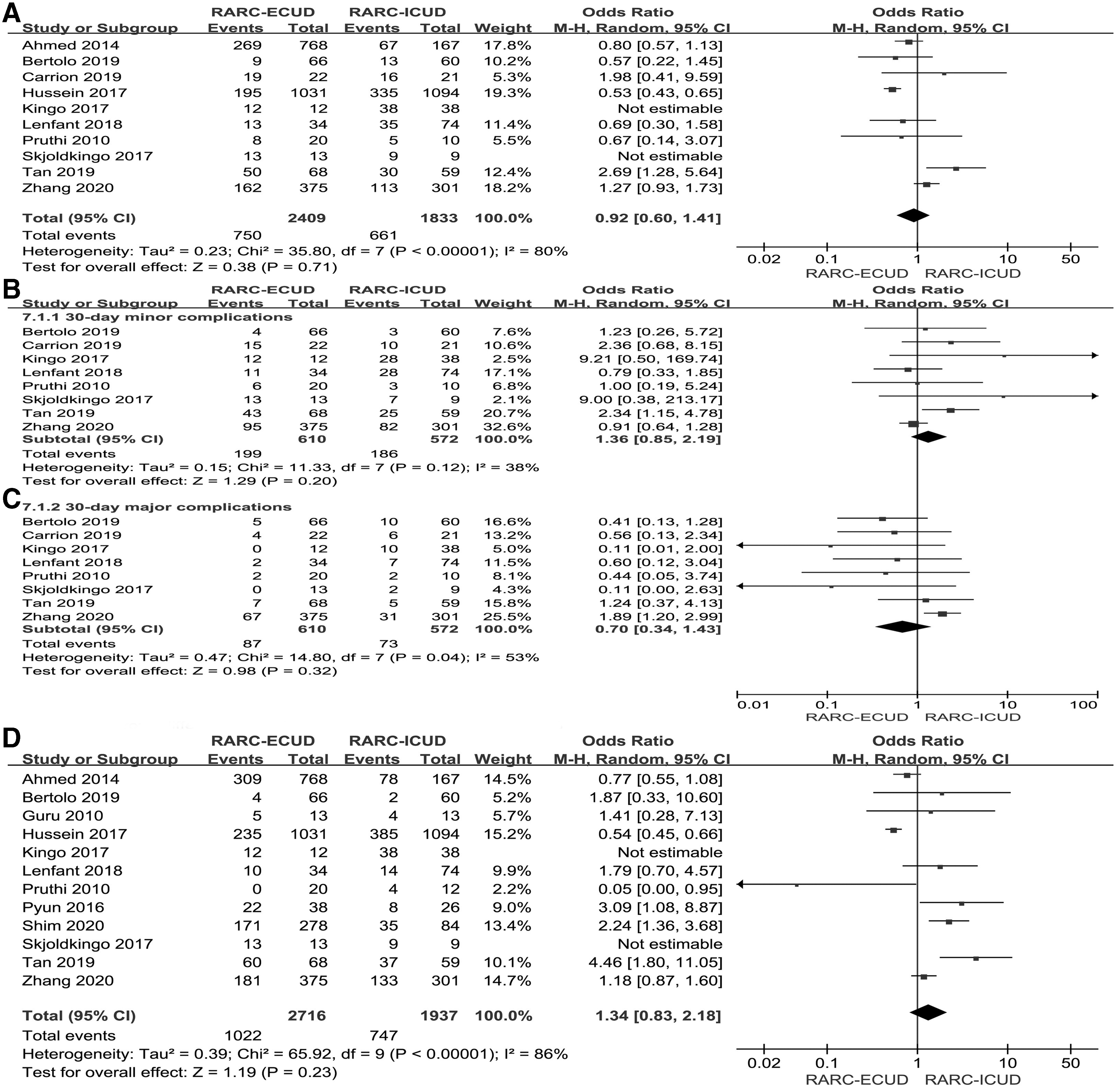
Forest plot and meta-analysis of 30-day overall complications
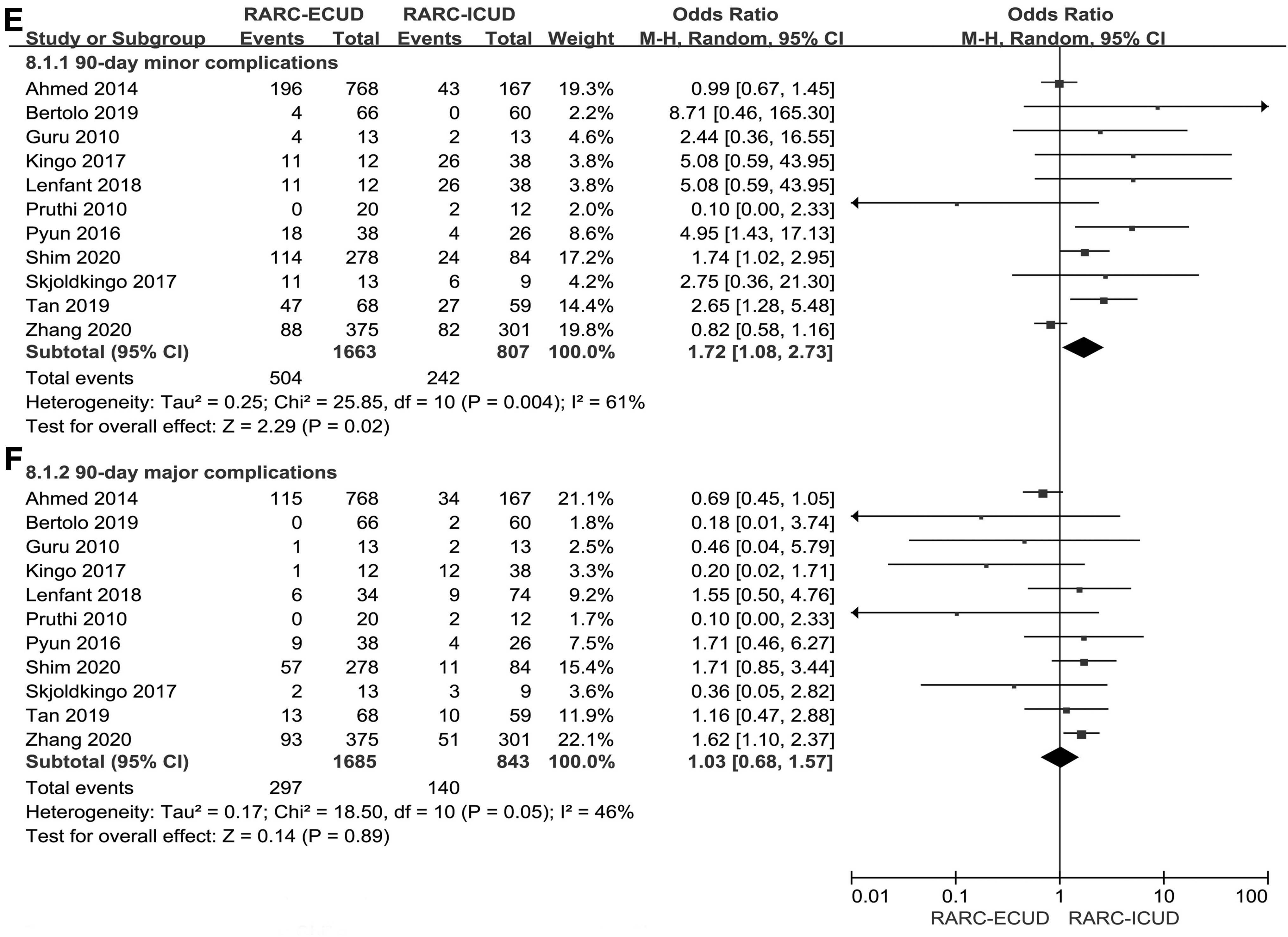
For 90-day complications, there was no significant difference between two techniques in the overall complications (OR: 1.34, 95% CI: 0.83–2.18, p = 0.23, Fig. 4D). However, a significant difference between the two groups was found for minor (OR: 1.72, 95% CI: 1.08–2.73, p = 0.02, Fig. 4E) and major (OR: 1.03, 95% CI: 0.68–1.57, p = 0.89, Fig. 4F) complications.
Subgroup analysis
The subgroup analysis suggested that ICUD was associated with less OT (MD: 32.45, 95% CI: 14.37–50.53, p = 0.0004, Fig. 2A) and less EBL (MD: 149.73, 95% CI: 21.33–278.13, p = 0.02, Fig. 2B) compared with ECUD. No differences between the two procedures were found in intraoperation blood transfusion (OR: 1.42, 95% CI: 0.27–2.95, p = 0.68, Fig. 2C), and LOS (MD: 0, 95% CI: −0.92 to 0.92, p = 0.99, Fig. 3B).
Discussion
Recently, the efficacy of ICUD has received wide attention because of a smaller incision, reduced pain, reduced risk of urinary leakage, and fluid imbalances. 4,25,26 So, we performed the systematic review to provide the best available evidence on this approach by comparing with ECUD.
For OT, we found that there was high heterogeneity. The subgroup analysis showed that the difference of ICUD type played a main role in the high heterogeneity. Lenfant and colleagues have proved this point. 18 Sensitivity analysis showed that initial experience and learning curve also were associated with high heterogeneity. In addition, Hussein and colleagues confirmed that whether extended lymph node dissection is also a source of heterogeneity. 16 Our subgroup analysis showed that the ICUD was 32.45 minutes less than ECUD. But it is a questionable significance in the clinic because of different surgeons and learning curve. In this connection, Tan and associates reported that a significant OT difference between the second of 29 cases and the first 30 cases (p = 0.004). 23 Besides, Dell'Oglio and colleagues believed that surgical experience was associated with shorter OT and the relationship was nonlinear according to multivariable linear regression models (p = 0.003). 27
Our cumulative analysis showed that a lower volume (99.28 mL) of EBL in the ICUD group, which is not necessarily clinical significance unless the total of blood loss is sufficient to transfusion. Hence, we further analyzed the difference in intraoperative blood transfusion rate between two groups, and found that an 80% risk of transfusion was reduced in the ICUD group compared with ECUD. Tan and associates believed that pneumoperitoneum and superior vision contribute to reduce blood loss by providing precise dissection. 23 For clinical significance, lower transfusion rate reduces potential risk factors, such as hemolysis. 28 On the contrary, based on previous studies, blood transfusion is strongly associated with tumor recurrence and mortality after radical cystectomy. 29 So more and more attention has been paid in a reduction of blood loss and transfusion rate in surgery.
About prognostic outcomes, we found that a 0.78 day shorter oral intake time was associated with ICUD. We believed that ICUD improved bowel anastomosis, decreased bowel exposure, and reduced risk of fluid imbalances, which was attributed to the results. However, it has little clinical significance because of the small sample size and widely variable approaches to post-op recovery, including enhanced recovery after surgery protocol, and intensive inpatient monitoring vs early discharge to home with outpatient nursing care.
For LOS, there was no significant difference with high heterogeneity. Subgroup analysis also showed that heterogeneity mainly comes from diversion type. But, two of 12 included studies supposed that LOS was shorter for ICUD than for ECUD because of the less complications related to bowel resection, especially gastrointestinal complications. 21,24 Moreover, it is closely associated with functional outcomes that ICUD may be superior to ECUD, simply due to absence of big transabdominal incisions in the latter. Since patients urinate by intra-abdominal pressure produced by straining using the abdominal muscles in the postoperative period, having an intact abdominal wall musculature might be advantageous in this regard. Balbay et al. and Atmaca et al. indirectly proved it, who reported that better trends were detected in ICUD concerning daytime continence. 30,31
For 90-day complications, our mate-analysis showed patients who underwent ICUD had lower 90-day minor complications, especially gastrointestinal. The lower postoperative complications are beneficial to improve postoperative recovery and quality of life, which is more popular in clinic. Moreover, Hussein and colleagues insisted that the complications will be lower with development of ICUD. 16 Obviously, the ICUD has great potential. Some studies of all included studies analyzed related complications according to the organ system involved, and found that the main postoperative complications of RARC were gastrointestinal and urinary infections. 12,14,24 Meanwhile, some studies found that the prediction of complications included age, BMI, American Society of Anesthesiologists (ASA) score, preoperative chemotherapy or abdominal surgery, and intraoperative blood transfusion after univariable and multivariable analysis. 12,16 Based on these predictions, we can better implement individualized treatment (surgical options) and reduce postoperative complications in clinic.
In addition, some included studies have mixed results on the survival and oncologic outcomes. Carrion and associates did not find differences in survival and oncologic results. 14 However, Hussein and colleagues found differences in terms of distant recurrences, disease-specific survival, recurrence-free survival, and overall survival between two groups. 16 We believed that the different results were associated with disease related factors, such as pathologic stage, nodal status, PSMs, and so on. Thus, the differences on survival and oncologic outcomes between the two procedures need further argument.
Besides, all included studies did not compare the quality of life between the two groups. A study found that RARC with intracorporeal orthotopic neobladder had a comparable bladder cancer-specific health-related quality-of-life scores to open orthotopic neobladder. 32 Therefore, the difference of quality of life is worth discussing between ECUD and ICUD.
Finally, we found that current studies on ICUD rarely compare the differences between the ileal conduit and neobladder. Desai and associates compared two kinds of urinary diversion types and found that the outcomes are not exactly similar between the two groups. 33 However, it needs more studies comparing the two approaches because of small sample size.
Although we performed this meta-analysis with the rigorous methodology of review and quantitative synthesis, some inherent limitations cannot be avoided. First, all included studies were analytical research, which reduced the quality of evidence. Second, the differences in patients' characteristics in urinary diversion type and in surgeon's experience in each of the studies might represent a major source of bias. Third, our study lacks the analysis of oncologic outcomes, functional outcomes, cost, and the quality of life between the two surgical techniques.
Conclusion
In conclusion, our systematic review and meta-analysis indicates that the RARC with ICUD is a safe and feasible alternative to RARC with ECUD. Also, ICUD is associated with less EBL, lower blood transfusion, shorter oral intake time, and lower 90-day complications. On subgroup analysis, the ICUD provides shorter OT. However, the results should be applied prudently in clinic because of the low quality of evidence. Further quality studies are needed to evaluate effectiveness of RARC with ICUD and its oncologic outcomes, functional outcomes, cost, and the quality of life.
Authors' Contributions
Conceived and designed the experiments: A.W. Analyzed the data: C.Y., L.P., Y.D., and H.W. Contributed reagents/materials/analysis: L.P., T.W., Y.D., and X.Z. Wrote the article: C.Y. and Y.D. All authors have read and approved the final article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by National Natural Science Foundation of China, grant no. 81900617, application code: H0503, relying unit code: 63700708A0140-0268.