
Abstract
Objectives:
The Thulium Fiber Laser (TFL) is studied as an alternative to the holmium:yttrium-aluminium-garnet (Ho:YAG) laser for lithotripsy, with the advantage of an induced bubble stream (IBS). This in vitro study compared the TFL's IBS with 150- and 272 μm-core-diameter laser fiber (CDF) and in four irrigant fluids.
Methods:
A TFL of 50 W (IPG Photonics©) and 150 and 272 μm-CDF (Boston Scientific©) were used, comparing nine energies (in the range from 0.025 to 4 J). An experimental setup consisted of a vertically disposed fiber in a cuvette filled with saline, iodinated contrast agent (IOA), human urine, or deionized water (DW) at ambient temperature. High-speed imaging of three consecutive IBS was performed to determine the influence of energy on their maximum length (ML; μm), width (MW; μm), and duration (MD; μs). Fibers were cleaved with ceramic scissors between each experience.
Results:
The IBS had higher ML and MW and MD with 150CDF than 272CDF. Maximum pulse rate for 150CDF and 272CDF was 2182 and 2000 Hz, respectively. Every maximum power was higher than the technological limit of TFL (>50 W). At equal energy density, 150CDF was associated with lower dimensions and durations. The IBS had higher maximum dimensions in IOA compared with saline solution (SS). Compared with DW and urine, IBS in IOA were longer beyond 500 mJ. Over 25 mJ, IBS were thinner in DW, urine, and SS. The IBS in DW, urine, and SS had similar maximum dimensions. The IBS's duration was higher in IOA compared with DW, urine, and SS, meaning a lower theoretical maximum pulse rate and power in IOA.
Conclusion:
Lasering with 150CDF fits with lower pulse energies–higher pulse rates settings than 272CDF, such as fine dusting mode. In IOA, Induced Bubbles Streams present higher dimensions and durations than in other studied fluids, related to its higher viscosity. Safety distance and pulse rate should be increased and decreased, respectively.
Introduction
Holmium:Yttrium-Aluminium-Garnet (Ho:YAG) laser is currently the standard for laser lithotripsy. 1 Its effectiveness, versatility, and safety profile with minimal tissue penetration depth and a low risk of undesirable tissue damage are well known, due to the relatively high absorption coefficient of the Ho:YAG laser wavelength in water. 2,3 As part of the mechanism of laser ablation, a vapor bubble is induced due to a pulse activation in a fluid medium. This phenomenon, often referred to as the “Moses effect,” helps to create a vapor channel to conduct the laser energy directly to the stone surface (photothermal mechanism). 4 –7
The Thulium Fiber Laser (TFL) has been recently explored as an alternative, because it offers several advantages over the Ho:YAG laser. 8 Over its architectural differences, TFL provides a four-fold higher absorption coefficient in water, allows to connect smaller operating laser fibers (LF: 50–150 μm core diameter), and could improve dusting lithotripsy with lower energies per pulse (as low as 0.025 J), and higher maximal pulse rates (up to 2000 Hz). As a comparison, the standard “dusting” mode of Ho:YAG laser can operate at a minimum energy of 0.2 J. 3
Bubbles dynamic studies showed several differences between Ho:YAG and TFL that could explain the potential stone ablation advantages with TFL: less retropulsion, smaller fragments, and two-fold to four-fold higher ablation rates. 9 –12 Inherently, TFL produces an induced bubble stream (IBS) defined by a succession of 50 to 60 microbubbles, which creates a vapor channel at the LF tip instead of a single or double (“Moses Technology”; Lumenis®) induced vapor bubble (IVB). 9 Thus, the TFL laser generator may present other physical properties for laser ablation, which could be modified by the pulse modulation or thinner LF. Furthermore, although the irrigation rate influence on fluid temperature is demonstrated, we are lacking data about the best irrigation fluid for stone lithotripsy. 13 –15 In vitro studies used various fluids such as deionized water (DW) or saline solution (SS), but in vivo conditions during flexible ureteroscopy reveal that we face a mixture of urine, iodinated contrast agent (IOA) (used for urinary upper tract opacification and fluoroscopy), SS, or DW for irrigation. 15 –18 There is, to our knowledge, no published evidence about the impact of the irrigation fluid on the IVB formations and dynamics.
Based on this, we aimed to compare the IBS dynamics between 150 and 272 μm core-diameter laser fibers (CDF) with TFL based on IBS characteristics. Secondary, we evaluated the influence of four irrigation fluids on IBS: SS, DW, IOA, and urine.
Methods
TFL generator and LF
A 50 W TFL generator (IPG Photonics®, Russia) with a wavelength of 1940 nm was used for all experiments, and it was modified to deliver single pulses. Three lithotripsy modes are available: “fine dusting” (FD, 25–150 mJ), “dusting” (D, 200–800 mJ), and “fragmentation” (Fr, 1–6 J), with respect to a 50 W maximum power. This TFL experimental version allows to operate with a small CDF down to 50 μm. We connected 150 and 272 μm-CDF (Sureflex; Boston Scientific©). Before experiments, both LF were sectioned by ceramic scissors to assess their real core-diameter under optical microscopy (Zeiss©, Germany).
Irrigation fluids
We compared four fluids frequently encountered during endocorporeal laser litotripsy: SS (NaCl 0.9%; Fresenius Kabi, Fresenius®, France), DW (Eau PPI Lavoisier 500 mL; Chaix et Du Marais®, France), IOA (Telebrix 30-meglumine; Guerbet®, France), and human urine from a 30-year-old man with no previous history of renal calculi and a daily water oral intake of two liters. An informed consent for the collection and use of urine sample was realized. All fluids were disposed at ambient temperature (20°C), and a 10 minutes duration was followed between the infilling and the laser pulse. The density of each medium was evaluated before experiments, and viscosity was noted when available (Table 1).
Characteristics of the Irrigation Fluids
cP = CentiPOISE; DW = deionized water; IOA = iodinated contrast agent; SS = saline solution.
IBSs experiment
In this part, we aimed to compare the IBS of nine different energy rates, three per lithotripsy mode: FD (25, 50, and 150 mJ), D (200, 500, and 800 mJ), and Fr (1, 2, and 4 J). Regarding pulse modulation, we respected the pulse presetting of TFL generator in each mode, meaning that in Fr, the double pulse was retained. Each pulse energy rate was successively studied in all four fluids.
Figure 1 presents the experimental setup for IBS evaluation: The LF tip was placed vertically in a cuvette filled with the chosen fluid. A specific fiber support was manufactured to assure a perfect immobility during laser emission. A 25 V halogen lamp was disposed behind the cuvette to create sufficient contrast between the LF and the IBS on one part, and the surrounding fluid on the other part. High-speed imaging of three consecutive IBS was performed at 15,000 frames per second and 7 μm spatial resolution (FastCam Ultima APX-RS 3000™ with a fixed magnifying lense; Photron Limited©), to determine the influence of energy on maximum bubble length (μm), width (μm), and duration (μs). The laser emission and the high speed camera were initiated and stopped jointly by computational command. The LF were cleaved with ceramic scissors between each experience. Image J (ImageJ©, NIH) and Photron Fastcam Viewer™ 2.4 (Photron Limited©) were used to assess bubble length and width, and duration, respectively. A theoretical maximum pulse rate and power was calculated based on pulse energy and duration.
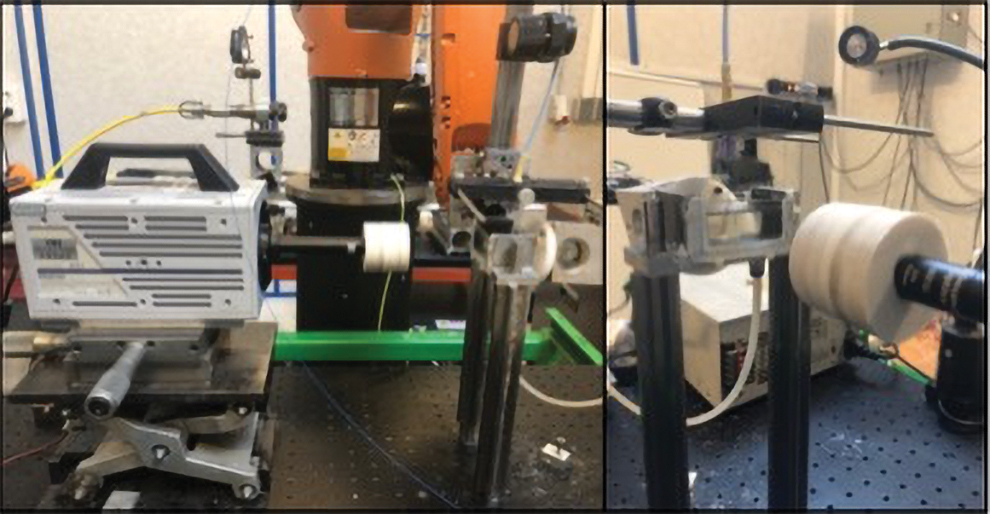
Experimental setup for the IBS video acquisition by using a FastCam Ultima APX-RS3000 with a fixed magnifying lense and a halogen lamp. IBS, induced bubble stream. Color images are available online.
Statistical analysis
For the IBS studies, length, width and duration, theoretical maximum pulse rate, and power are presented as median values and compared by using a two-tailed Student t-test was used with Rstudio and GraphPad Prism; p-values of <0.05 were regarded as statistically significant. Nonlinear and linear regression models were calculated, in all fluid mediums and added as curves in all graphs.
Results
The observation under optical microscopy of both 150 and 272 μm-CDF showed a 162 and 289 μm real core-diameter, respectively. We calibrated our experiments according to those findings. Thus, to maintain a same irradiance (W/μm2) or energy density (J/μm2), it would be necessary to select a three-fold lower pulse energy with 150 μm-CDF, considering the same pulse rate for irradiance.
Induced bubble streams
Impact of LF diameter
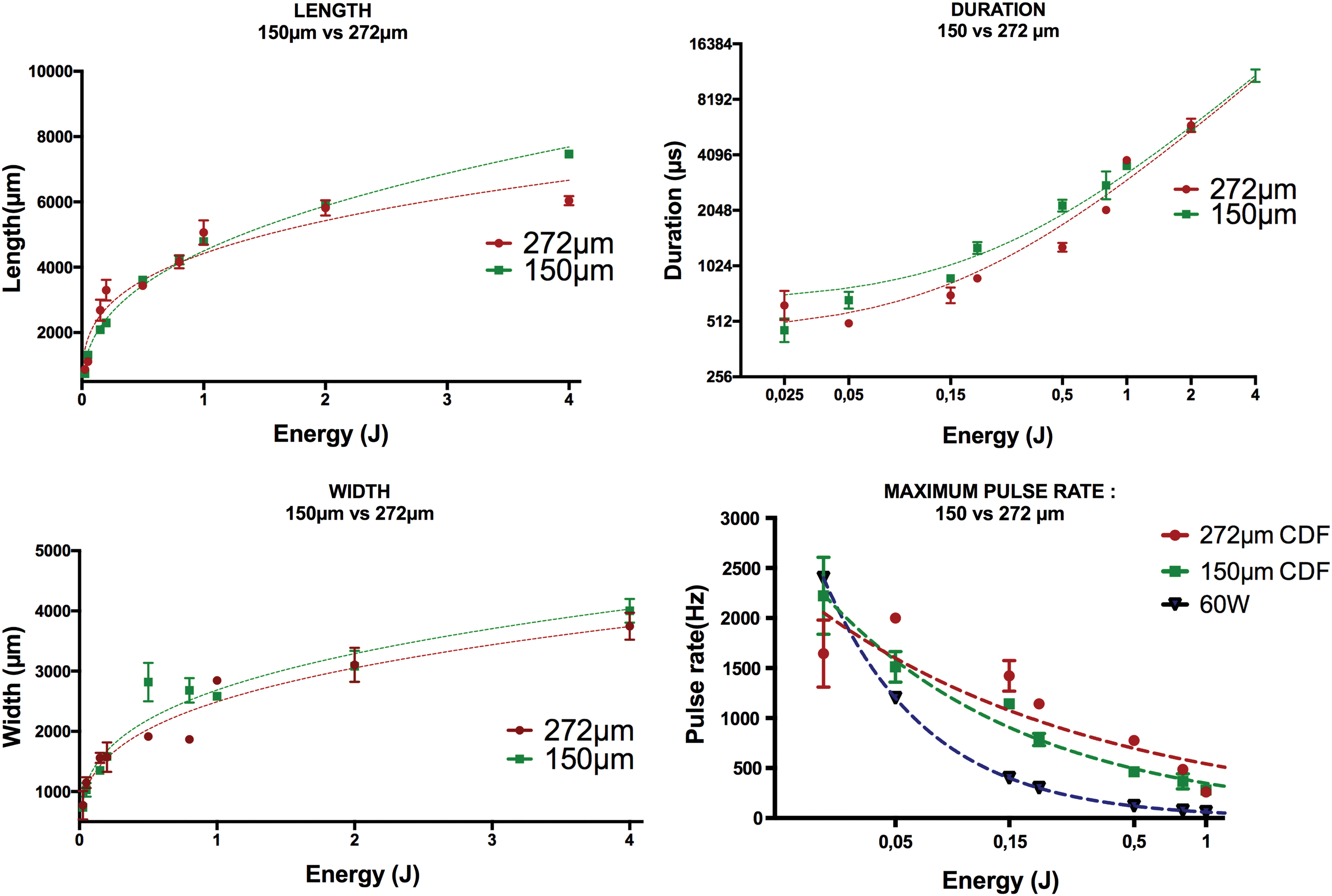
IBSs had higher maximum lengths with 150 μm-CDF than 272 μm-CDF, except when energy was 25 (p = 0.04), 150, 200 mJ (p = 0.02), and 1 J (Fig. 2 and Table 2). The nonlinear regression model (NLRM) evaluation showed, respectively, for 150 and 272 μm-CDF's lengths: length = (3.653 ± 0.004445) + (0.3864 ± 0.00899) × Energy and length = (3.645 ± 0.01168) + (0.2962 ± 0.02225) × Energy, respectively.
IBS of 150 and 272 μm-CDF with TFL in SS. CDF, core-diameter laser fiber; SS, saline solution; TFL, Thulium Fiber Laser. Color images are available online.
Induced Bubble Stream Characteristics According to Energy (J) and Laser Fiber Core Diameter with Thulium Fiber Laser
The IBS had higher maximum widths with 150 μm-CDF than 272 μm-CDF, except when energy was 25 (p = 0.04), 50, 150 mJ (p = 0.04), and 1 (p = 0.03) and 2 J (Fig. 2 and Table 2). An NLRM was estimated for 150 and 272 μm-CDF's widths: width = (3.429 ± 0.010356) + (0.2929 ± 0.01969) × Energy and width = (3.396 ± 0.009856) + (0.2933 ± 0.01873) × Energy, respectively.
These differences were statistically significant at 500 mJ and 4 J for length, and 500 and 800 mJ for width.
The IBS duration was higher with 150 μm-CDF than with 272 μm-CDF (statistically significant at 200 and 500 mJ), except when energy was 25 mJ. An NLRM showed for 150 and 272 μm-CDF's durations: duration = (648 ± 89.07) + 2596 ± 57.03) × Energy and duration = (442.7 ± 106.7) + 2539 ± 68.3) × Energy, respectively.
The nonlinear regression evaluation is consistent with the quantitative analysis for length, width, and duration.
Theoretical maximum pulse rate for 150 and 272 μm-CDF was 2182 and 2000 Hz. Every maximum power was higher to the technological limit of TFL (>50 W), except for 25 mJ (50 W for 150 μm-CDF and 40 W for 272 μm-CDF) (Fig. 2 and Table 2).
At equal energy density or irradiance, 150 μm-CDF was associated with lower length, width, and duration (50 mJ150μm-CDF vs 150 mJ272μm-CDF, 150 mJ150μm-CDF vs 500 mJ272μm-CDF).
Impact of irrigation fluids
The IBS had higher maximum lengths and widths when activation was made in IOA compared with SS, except when energy was 150 and 200 mJ, and 25 mJ, respectively (Fig. 3 and Tables 3 and 4). These differences were statistically significant for energy higher than 800 mJ for length, and 150 mJ for width (except 500 mJ). Compared with DW and urine, IBS in IOA were longer beyond 500 mJ (but were shorter for lower energies). For 50 mJ or more, IBS were thinner in DW, urine, and SS than in IOA.

IBS of 150 μm-CDF with TFL according to medium fluid: SS, deionized water, iodinated contrast agent and urine. Color images are available online.
Induced Bubble Stream Characteristics According to Energy (J) and Liquid Medium with Thulium Fiber Laser
Theoretical Maximum Pulse Rate and Power According to Fluid Medium
The IBS duration was higher in IOA compared with DW, urine, and SS, meaning a lower theoretical maximum pulse rate and power in IOA (Fig. 3 and Tables 3 and 4). Theoretical maximum power was above technological limit of the TFL (50 W) in all fluid mediums, except for 25 mJ.
The IBS in DW, urine, and SS had similar lengths, widths, and duration evolution beyond energy as verified by nonlinear (length and width) and linear (duration) regression models (data not shown). Those results did not differ among CDF.
Discussion
150 μm vs 272 μm-CDF TFL IBSs
IBS dimensions and duration
The IBS studies with 150 μm-CDF showed greater length, width, and duration than for 272 μm-CDF, according to the NLRMs. Our data are supported by the energy density (J/cm2) thesis, which is three-fold higher with 150 μm-CDF at equal pulse energy, compared with 272 μm-CDF. When analyzing IBS at equal energy density, we found that 150 μm-CDF was associated with a lower length, width, and duration. The IBS characteristics may depend on the physical properties of IVB and its surface pressure, which remain unknown for both Ho:YAG and TFL. Lowering the CDF could result in smaller cavitation bubbles with a lower cavitation pressure, explaining its smaller dimensions or duration. Differently speaking, a lower LF could produce lower IBS, considering length and width, with a shorter duration. Those results support 150 μm-CDF as an LF made for FD: very low pulse energy (<200 mJ), very high pulse rates (>100 Hz). This could also explain the thinner produced fragments and fissures with 150 μm CDF compared with 272 μm-CDF. 12 Overall, 150 and 272 μm-CDF NLRM show an exponential increase of IBS dimension for lower pulse energy than 2 J. In clinical practice, 4 and 6 J pulse energies may not be relevant, even during miniaturized or standard percutaneous nephrolithotomy. Considering that, we could affirm the nonlinear association between IBS dimension and pulse energy.
Furthermore, the impact of CDF on IBS is controversial. Although a larger CDF produces larger vapor bubbles with Ho:YAG, it has not been described with TFL. 9,19 In Hardy et al. in vitro experiment, the IBS dimensions were not interpreted to be influenced by CDF but 105 μm-CDF IBS were thinner but with greater lengths than 270 μm. Our data integrate a wider range of pulse energies. This could explain the current results, with statistically significant differences in dimensions higher than 800 mJ. As a limitation, we emphasize that our CDF choice could have influenced our results, considering that the LF models are not systematically announced in the available literature.
Theoretical maximum pulse rate beyond pulse energy
Bubble dynamics analysis in medium fluid needs a laminar surrounding liquid for reproductible IBS. 20 To maintain this physical state, an IBS needs to be entirely reabsorbed before a next IBS could appear. Based on this, our findings report the theoretical maximum pulse rates and power for both 150 and 272 μm-CDF. Even 150 μm CDF would present lower maximum values, they were higher to the technological limit of the TFL generator (50 W for experimental, 60 W for medical use), except for 25 mJ. To our knowledge, we first define these useful safety data for TFL. However, as previously described, when decreasing the pulse energy, the amount of time to create an IBS is greater. 9,20 This unrecorded time could have minimized the IBS duration and overrated the theoretical maximum pulse rates and power. Further, we could analyze the IBS length as the maximum working distance for radiation delivery during ureteroscopic laser lithotripsy, as TFL peak absorption in water is close to the highest point. 8,10,21 This could consist of a second safety concept for clinical practice.
Although Hardy et al. affirm that TFL induces a four-fold smaller IBS than Ho:YAG, we noticed similar dimensions (length and width) between TFL IBS and Ho:YAG vapor bubble. In their study, they compare very low pulse energies for TFL (5 to 35 mJ) to a minimal 200 mJ to maximal 1 J pulse energy for Ho:YAG, using 105 μm (TFL) and 272 μm (TFL and Ho:YAG) CDF. At available minimal respective settings (25 mJ for TFL, 200 mJ for Ho:YAG), the statement is valid, but our findings reveal similar dimensions at equal settings. Consequently, the “stream” phenomenon and the radiative ablation effect could explain the better efficiency of TFL, even with a lower peak power (PP, W) than Ho:YAG. Thus, the PP could influence the TFL's ability to ablate stones. It represents the maximum value of power during the laser pulse (second), whereas the average power (W) is defined as the energy of a single pulse (J) times the number of pulses per second (Hz). Previous TFL generators used a 100 W PP, whereas the last experimental versions present a five-fold higher PP (500 W), which is still three-fold lower than Ho:YAG's (1700 W). 10,22 –24 A recent in vitro evaluation of comparative PP with both High Power Ho:YAG and TFL reported longer pulse width (duration) and lower PP for TFL, but a lower retropulsion, without sacrificing the ablation efficiency. Thus, the ablation volumes were two-fold higher with TFL compared with Ho:YAG in their experiments. 25 The link between ablation efficiency (ablated weight or volume, fissures, and produced fragments) and IBS dynamics is manifest but further investigations are needed to determine the part of each component of stone ablation.
Irrigation fluids and lithotripsy
The IBS studies in several fluid mediums showed that IOA has an influence on bubble formation, dimensions, and duration (Fig. 3 and Tables 3 and 4). In SS, DW, and urine, IBS had similar lengths, widths, and duration; whereas IOA's IBS were longer, wider, and greater than in others. To our knowledge, no previous in vitro experiments studied induced bubble dynamics in these “endo-urological fluids.” Consequently, theoretical maximum pulse rates and power would be lower in IOA. The greater IBS lengths in IOA may also be relevant as a higher working distance. Clinicians should consider pumping out the IOA after opacification before laser lithotripsy to avoid potential side effects and unintended laser pulses.
Considering that, we must recognize some limitations to this experiment. First, we used a nationally revoked IOA for intravenous injection because of its high osmolar characteristic. 26 These products are still commercialized for intra-cavity injection. The national committee recommendation does not state which product clinicians should use but the high-osmolar products could induce a slightly higher pressure in the concerned cavity (renal pelvix), causing a higher pain rate in the postoperative period. Moreover, we performed our tests with human urine from a 30 year-old man without any history or renal calculi. The samples may not have been relevant, with no hypercalciuria, no hyperoxaluria or any metabolic disorder that could induce the crystallization or the lithogenesis. 27 Color-guided urine samples could improve the experimental setup when a biological analysis is not available, as used for animal in vivo studies. 28
Considering these limits, the greater viscosity of the IOA can explain our results. In fluid dynamics, although the events during bubble generation are strongly influenced by the laser parameters, the subsequent bubble evolution is primarily influenced by the properties of the fluid and the boundary conditions close to the laser tip. 20 Therefore, we must recognize the absence of dynamic viscosity measurement for our urine sample and DW, whereas IOA density was higher compared with the three other fluids. We suppose that the viscosity of SS, DW, and urine was close, according to our results and the fluid density. Moreover, we emphasize the difference of temperature between our experimental conditions (20°C) and clinical situations (37°C), even more during laser lithotripsy. 15,17,29,30 This could have modified our findings. Finally, our experimental setup included a fixed magnifying lense, forcing to readjust the distance and the contrast for each IBS acquisition.
Conclusion
The TFL is currently evaluated as an alternative to Ho:YAG laser for stone lithotripsy. This study analyzed the IBS dynamics beyond CDF, laser pulse energy, and irrigation fluids. The IBS with 150 μm-CDF presented greater dimensions and a longer duration compared with 272 μm-CDF. These results are due to a three-fold greater energy density with 150 μm-CDF and, consequently, lowering by three times the pulse energy would help to maintain similar IBS characteristics. Our study suggests that 150 μm-CDF is made for FD lithotripsy. Intraoperative IOA opacification of the upper tract during flexible ureteroscopy should be considered by clinicians, as TFL's IBS have greater dimensions and longer durations than in the other encountered fluids. Safety distance and pulse rate should be increased and decreased, respectively.
Research Involving Human Participants or Animals
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
This article does not contain any studies with human participants or animals performed by any of the authors.
Footnotes
Authors' Contribution
F.P.: protocol development, data collection and management, data analysis, article writing, and editing. L.B.: protocol development, data collection and management, and article editing. C.G.: protocol development, data collection. S.D.: protocol development, article writing, and editing. O.T.: protocol development, data analysis, article writing, and editing.
Acknowledgments
The authors thank Gregory Altshuler and Ilya Yaroslavsky at IPG Medical Corporation (Marlborough, MA) for providing the TFL used in the experiments and for discussion of the results.
Author Disclosure Statement
The authors declare that they have no conflict of interest; however:
O.T. has been declared as a consultant for Boston Scientific Corporation, Coloplast, Wolf, B-Braun, IPG photonics, Olympus and Rocamed. S.D. has been declared as a consultant for Boston Scientific Corporation and Coloplast.
Funding Information
Frédéric Panthier received a French Association of Urology Research Grant (2018).