
Abstract
Background:
Ureteral stents are commonly employed after ureteroscopy to treat urinary stone disease, but the devices impose a substantial burden of stent-associated symptoms (SAS), including pain and urinary side effects. The NIDDK (National Institute of Diabetes and Digestive and Kidney Diseases) Urinary Stone Disease Research Network sought to develop greater understanding of SAS causes and severity among individuals treated ureteroscopically for ureteral or renal stones.
Materials and Methods:
We designed a prospective, observational cohort study comprising adolescents and adults undergoing ureteroscopic intervention for ureteral or renal stones. Participants will undergo detailed symptom assessment using validated questionnaires, a psychosocial assessment, and detailed collection of clinical and operative data. Quantitative sensory testing will be utilized to assess pain sensitization. In addition, a small cohort (∼40 individuals) will participate in semi-structured interviews to develop more granular information regarding their stent symptoms and experience. Biospecimens (blood and urine) will be collected for future research.
Results:
The Study to Enhance Understanding of sTent-associated Symptoms (STENTS) enrolled its first participant in March 2019 and completed nested qualitative cohort follow-up in August 2019. After a planned pause, enrollment for the main study cohort resumed in September 2019 and is expected to be completed in 2021.
Conclusion:
STENTS is expected to provide important insights into the mechanisms and risk factors for severe ureteral SAS after ureteroscopy. These insights will generate future investigations to mitigate the burden of SAS among individuals with urinary stone disease.
Introduction
The use of stents to maintain ureteral patency after ureteroscopic treatment of urinary stones is common practice. 1 Both the European Association of Urology and the American Urological Association guidelines recommend ureteral stent placement in cases where patency is critical, such as solitary kidney or ureteral injury. While considered optional in cases of uncomplicated ureteroscopy, 1 nearly four of five ureteroscopic procedures result in stent placement. 2
Stents are associated with significant morbidity: more than 80% of patients report impaired quality of life from bothersome urinary symptoms and pain affecting daily activity. 3 These stent-associated symptoms (SAS) result in increased narcotic use and unplanned health care (e.g., emergency department visits). 4,5 Approximately 32% of patients report sexual dysfunction, and 58% report impaired capacity or efficiency while at work.
Most interventional studies in patients with SAS have either focused on stent factors (materials, configurations, and drug-eluting nature 6 –12 ) or investigated medications targeting urinary tract symptoms. 13,14 Still, key knowledge gaps inhibit progress toward substantially mitigating SAS. The underlying physiologic response to the ureteral stent is not well defined, yet clearly manifests in patients as signs (e.g., hematuria), symptoms (e.g., pain), or abnormal test results (e.g., sterile pyuria) (Fig. 1). Studies of acute pain suggest that a number of host phenotype factors (i.e., clinical, psychosocial, and pain sensitization) and operative factors are important considerations in the mechanism and/or patient experience and remain ill-defined in this clinical context. An additional key consideration for achieving greater understanding of ureteral SAS is proper assessment of self-reported symptoms. Available assessment instruments (e.g., the Ureteral Stent Symptom Questionnaire [USSQ]) were initially developed in the context of longer stent dwell times but were not designed to assess SAS in the relatively short (∼1 week) time frame usually associated with post-ureteroscopy stent dwell times. Other measures, such as the Patient-Reported Outcomes Measurement Information System (PROMIS), are designed to assess aspects of physical, social, and mental health in the general population and among individuals with chronic conditions but have not been extensively employed after ureteroscopy. Finally, detailed assessment of the time course of patient symptoms is needed to provide insight into discriminatory ability of the instruments.
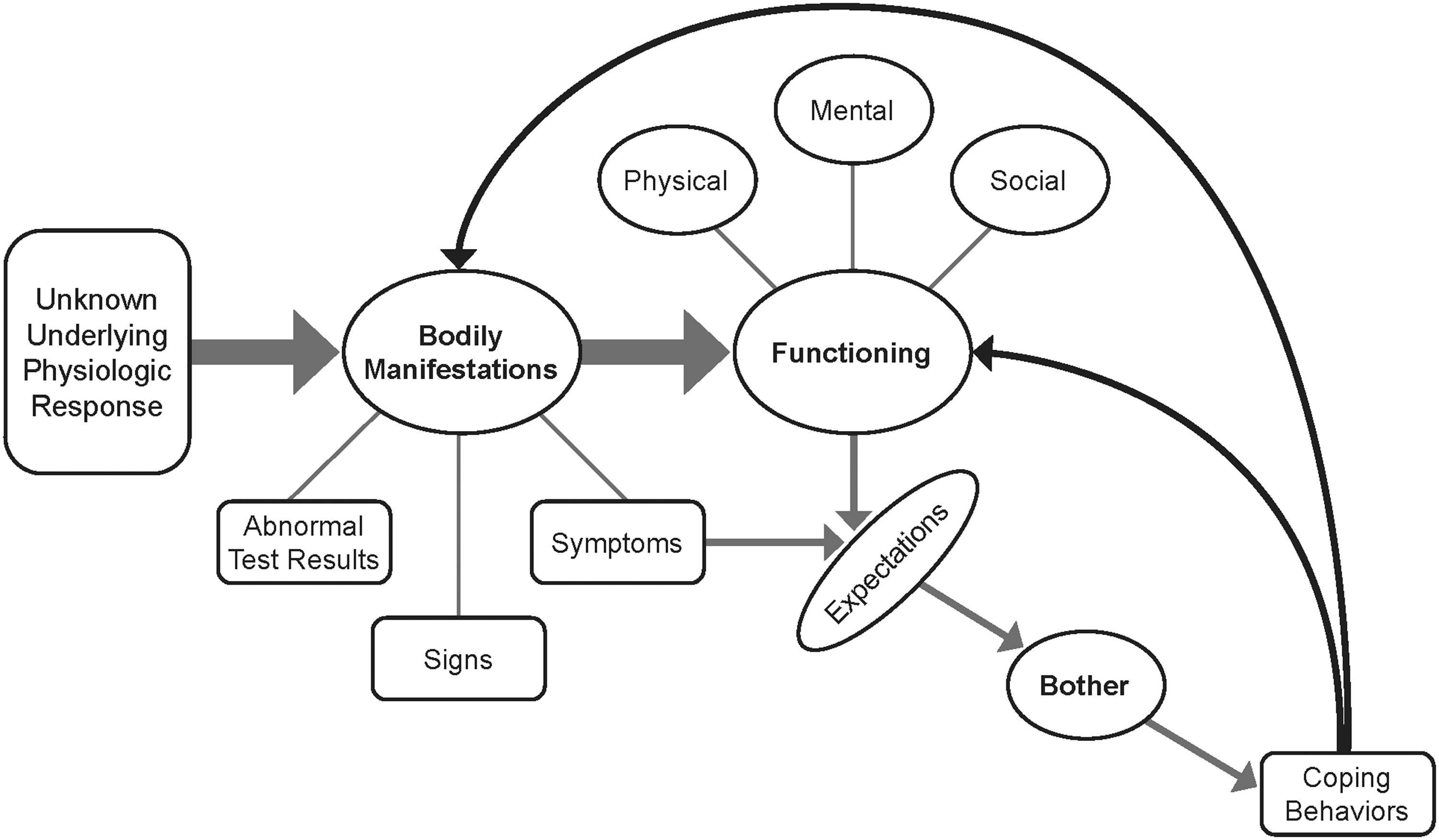
Conceptual model of ureteral stent-associated symptoms.
To gain further insight into the factors that are potentially related to SAS, the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)-funded Urinary Stone Disease Research Network (USDRN) has designed the Study to Enhance Understanding of sTent-associated Symptoms (STENTS). STENTS is a prospective, observational cohort study of adolescents and adults undergoing ureteroscopy with a planned ureteral stent placement for treatment of urinary stone disease.
Rationale for Study Design
The purpose of STENTS is to address five important knowledge gaps: (1) comparison of patient-reported symptom assessments in the domains of urinary symptoms, pain, and interference; (2) characterization of associations between SAS and participant demographic, psychosocial, clinical, and procedural factors; (3) assessment of the association between central sensitization and stent-associated pain; (4) generation of a preliminary multivariable prediction model for severe SAS; and (5) description of SAS in a cohort of participants undergoing bilateral ureteroscopy with bilateral ureteral stent placement. We also sought to create a biospecimen repository for future research into biological mechanisms of SAS.
Study setting
The study is being conducted within the USDRN, comprising four Clinical Centers (see the Acknowledgments section). The long-term goal of the USDRN is to inform clinical practice by (1) providing evidence on the effects of fluid intake on urinary stone recurrence, 15 (2) understanding and reducing pain and suffering from the use of ureteral stents, and (3) creating data and biological specimen resources for the urologic community. The review board of each institution provided ethical approval for the study.
Domains
Patients with indwelling ureteral stents report symptoms in a variety of domains, including urinary symptoms; pain; limitations in their ability to engage in usual activities (i.e., interference), including social, work, and school-based activities; and sexual functioning. In the context of current U.S. practice for ureteroscopic stone treatment, with relatively short stent dwell times, we focused on three domains: pain, urinary symptoms, and interference in usual activities. In contrast to previous work assessing additional domains, 16 these were postulated to be the most relevant experiences for patients who had short-term ureteral stents, rather than extended ureteral stent placement (weeks).
Nested qualitative cohort
To provide evidentiary support for the assumption that these three domains would be most relevant for patients, as well as for other exploratory purposes, we planned a nested qualitative cohort (NQC) for STENTS. The NQC comprised the first 40 consecutively enrolled participants who completed daily symptom questionnaires and participated in a semi-structured interview, in addition to other procedures identical to those for the remainder of the cohort (see the Study Design section). We designed the NQC to explore several key questions, including the extent to which symptoms assessed by questionnaires were relevant to the participant's stent experience, to identify potential coverage gaps in the questionnaires or domains, and to identify the most bothersome SAS (Table 1). We also sought to understand how self-reported symptoms varied day-to-day during the relatively short dwell time of post-ureteroscopy stent placement. To ensure that the NQC sample included a sufficient age distribution, we prespecified minima as follows: 8 individuals aged 12–25 years, 12 males aged >25 years, and 12 females aged >25 years. The NQC is designed such that all participants will complete the same study procedures as those in the subsequent larger observational cohort.
Knowledge Gaps and Planned Analyses
SAS = stent-associated symptoms.
Study Design
Study population
The study population included consenting participants at least 12 years of age with a clinical indication for ureteroscopy for renal and/or ureteral stones. Exclusion criteria focused the study population to those patients without recent stenting, concomitant procedures, or conditions that would potentially interfere with completion of study procedures (Table 2). The total enrollment target for the main STENTS study is ∼460 participants, including the NQC (n = ∼40) and an exploratory bilateral ureteroscopy/stent cohort (∼60 participants).
Exclusion Criteria
Study procedures
Preoperatively, participants will complete baseline assessments of psychosocial characteristics, symptoms, clinical factors (including pertinent stone history, such as prior stent experience), and quantitative sensory testing (QST) (Fig. 2 and Table 3). In the perioperative period, investigators will collect detailed information about the ureteroscopic procedure, along with blood and urine samples. Postoperatively, participants in the main study cohort will complete symptom assessments on postoperative days 1, 3, and 5; the day of ureteral stent removal (before stent removal); and 30 days after ureteral stent removal (Table 3). QST ) will also be completed on the day of stent removal. Preoperative and postoperative medication prescribing is per usual clinical practice at each center. The study leverages variation in clinical practice between centers to explore associations between medication and symptom severity; a medication diary will be completed daily by participants from the day of procedure until stent removal. If a participant requires a second-stage procedure, the individual is followed through the entire course of treatment, including assessment of stent symptoms after first- and second-stage ureteroscopy.
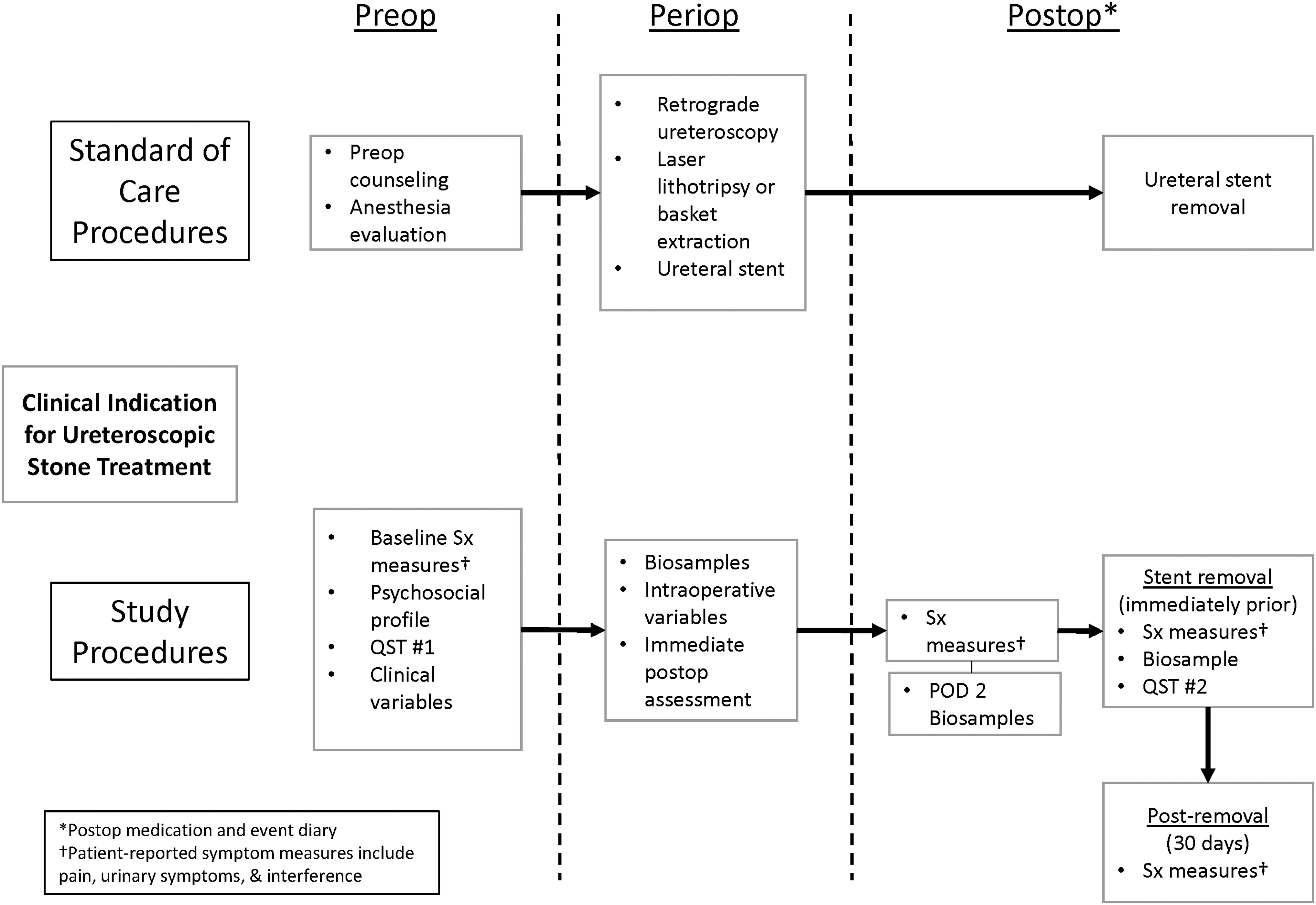
STENTS study schema. QST = quantitative sensory testing; Sx = symptoms.
List of Psychosocial and Patient-Reported Symptom Questionnaires
Urinary symptoms not assessed in adolescent participants.
Entire USSQ instrument completed on day of ureteral stent removal (before removal).
GQ = Global Quality; LURN SI-10 = 10-Item Lower Urinary Tract Dysfunction Research Network Symptom Index; PROMIS = Patient-Reported Outcomes Measurement Information System; USSQ = Ureteral Stent Symptom Questionnaire.
NQC study procedures
Participants in the NQC complete all study procedures as outlined, along with additional study procedures focused on addressing specific knowledge gaps. To reveal day-to-day variation in symptoms, patients complete daily symptom assessments. In addition, semi-structured interviews will be conducted by trained interviewers 7–30 days after stent removal with topics focusing on (1) relevance of symptom questionnaires to patient experience, (2) identifying coverage gaps (experiences not captured by existing instruments), and (3) prioritization of impacts from SAS. At the conclusion of the NQC, a pause will occur to reassess the frequency of stent symptom assessment.
Quantitative sensory testing
QST consists of applying a stimulus to peripheral tissue and recording a pain-related response. QST has been used extensively in pain research to study hypersensitivity and central sensitization. 17 –19 For the current study, pain thresholds to pressure stimulation and temporal summation with point pressure stimuli will be selected because they are easily implemented into clinical routine and because they may predict persistent postsurgical pain. 20,21 Expansion of painful areas is a clinically relevant phenomenon and a surrogate measure of central sensitization processes. 22 QST will be performed only in adult participants. We use repeated pointed pressure stimulation, an established human model of central pain facilitation called temporal summation. 23,24 QST will be performed on the flank (T12 dermatome) and the lower abdominal quadrant (L1 dermatome) ipsilateral to anticipated stent placement. Testing performed on the contralateral forearm will serve as a control stimulation.
Biospecimen repository
Biological specimens (blood and urine) will be collected from participants and stored for future research. Urine will be collected from all participants at baseline (shortly before ureteroscopy), on postoperative day 2, and on the day of stent removal. Blood specimens will be collected preoperatively, postoperatively before discharge from the facility, and from adults on the day of ureteral stent removal. Specimens will be stored at the NIDDK Biorepository until needed for future investigations.
Analytic considerations
Interview data from the NQC will be assessed using standard qualitative analytic approaches. For the three content areas of the interview—experiences with symptoms, quality of life, and ureteroscopy and stent removal—interviewers will systematically document the reoccurring topics/experiences and any new themes described by a participant. Reoccurring as well as less frequently described topics/experiences will be summarized. Audio recordings will be transcribed verbatim. All transcripts will be formatted similarly and imported into NVivo 12, a qualitative data management and analysis software program. A single qualitative codebook will be developed. Analysts will use NVivo 12 to independently apply the structural codes to transcripts. Intercoder reliability assessments will be conducted on ∼25% of transcripts. Next, analysts will identify and apply content-driven codes to the text for each conceptual category/structural code. Discrepancies in coding will be resolved through analyst discussions; transcripts will be recoded and the codebook revised accordingly. Once coding is complete, analysts will examine code frequencies across transcripts to describe the range of participants' experiences and the salience of the topics/experiences identified.
Analyses from the main cohort will describe the clinical and demographic characteristics of study participants and evaluate hypothesized associations between psychosocial, clinical, demographic, and operative characteristics on the one hand and patient-reported experiences on the other. Generally, descriptive statistics of the characteristics of the participants, including summary measures of central tendency and dispersion, will be reported. Variables will also be summarized by clinically relevant subgroups (age, sex, and USDRN clinical center).
Detailed descriptions of each analysis will be included in each article describing results from STENTS. The analytic approach will be as follows: The distribution of responses to self-reported symptom measures (i.e., pain score, Table 3) and psychosocial questionnaires will be examined. If variables are normally distributed, parametric tests (e.g., two-sample t-test) to compare two groups or analysis of variance for more than two group comparisons will be used. If outcome variables are not normally distributed, nonparametric tests (e.g., Wilcoxon rank-sum test) to compare two groups or the Kruskal–Wallis test for more than two group comparisons will be used. If outcomes are binary or categorical, we will use chi-square tests and logistic or multinomial regression models to examine associations. Further analyses of subgroup differences will use multivariable regression to control for demographic characteristics and multiple measures of clinical and operative history. Power calculations were based on four anticipated statistical tests of the hypotheses: t-tests, logistic regressions, correlations, and chi-square tests (with continuity correction). All demonstrated adequate power (>80%) to detect small-to-moderate effect sizes (Supplementary Table S1). All calculations are based on a two-sided significance level of 0.05.
Discussion
STENTS provides the largest well-characterized prospective cohort of individuals undergoing ureteroscopy with stone treatment and stent placement and will be the first to include pediatric and adult patients. The comprehensive data collection will enable detailed characterization of participant psychosocial characteristics, baseline clinical data, and granular procedural details. Detailed outcomes, including symptom assessment using multiple validated instruments across the domains of pain, urinary symptoms, and interference, supplemented by semi-structured interview data, will provide a robust picture of the patient experience in the modern ureteroscopy era. We anticipate that patient care for stone disease will be improved by leveraging STENTS study results.
STENTS data will enable several contributions to the scientific understanding of, and treatment of patients with, ureteral SAS. For example, data from the NQC will contribute to the understanding of day-to-day variation in SAS, participants' lived experience with an indwelling stent as well as stent removal, and any potential coverage gaps for self-reported symptoms after ureteroscopy. QST will provide insights into the pathophysiology of stent-related pain, the degree to which baseline hypersensitivity and central sensitization contribute to the severity of symptoms, and the extent to which SAS could lead to central sensitization. Large sample size and detailed phenotyping will provide an opportunity to identify risk factors for more severe SAS. Finally, the creation of a biospecimen repository will provide opportunities for future studies directed at biological mechanisms underlying SAS.
The use of multiple instruments across the three domains creates the potential for a parsimonious set of measures for rapid assessment of postoperative symptoms in clinical practice. The entire USSQ will be administered before ureteral stent removal. Questionnaires with a substantial number of items to complete often face barriers to implementation in clinical practice, so more efficient (fewer-item) instruments may be helpful in this regard, as noted by Borofsky and colleagues. 25 Our findings may also indicate an opportunity to revise domains or the analytic period of interest, which could be addressed in a future study. Finally, we have noted participants undergoing ureteroscopy during the COVID-19 pandemic, which will permit exploratory analyses of cohorts based on treatment before and during the pandemic.
Potential exists for gaining insight into the mechanism(s) of severe SAS. Detailed procedural information will provide insight into the contribution of the ureteroscopic intervention to symptom severity. The psychosocial inventory can assess the extent to which specific factors, such as the presence of substantial somatic symptom burden, can increase the likelihood of severe SAS.
These insights may provide important opportunities for future interventional studies. For example, if central sensitization (or the development thereof) has a strong association with severe symptoms, then medications known to attenuate central sensitization (e.g., gabapentin) could be evaluated. If certain psychologic conditions increase the risk of severe symptoms, then medication or mindfulness-based strategies could be assessed for improved pain control. 26
Other strategies for mitigating the burden of ureteral SAS include more selective utilization of stents. For example, the detailed clinical data could inform a risk-prediction model for severe ureteral SAS, allowing identification of at-risk individuals in whom stents could be omitted as clinically appropriate. Alternatively, additional follow-up resources (e.g., nurse teleconference or patient education) could be directed toward these patients, reducing the risk of unnecessary high-acuity health care utilization.
Conclusions
STENTS is an observational, prospective cohort study that will contribute substantially to several key unanswered questions regarding ureteral SAS after ureteroscopy for stone removal. Beyond the analyses outlined herein, a substantial number of potential secondary research questions exist that could be addressed in this well-characterized cohort. These insights will lead to strategies for mitigating the burden of ureteral SAS, either through novel therapeutics or through risk stratification. These findings and data will be an important contribution to the urologic community, as well as patients requiring ureteroscopic stone treatment.
Footnotes
Acknowledgments
We thank Peter Hoffmann for article preparation and submission. Mr. Hoffmann did not receive compensation beyond his employment by Duke University.
Urinary Stone Disease Research Network (USDRN): The following individuals were instrumental in the planning and conduct of the STENTS study at each of the participating institutions.
Clinical Centers
University of Pennsylvania/Children's Hospital of Pennsylvania, Philadelphia, PA: PI: Peter P. Reese, MD, MSCE; Gregory E. Tasian, MD, MSCE. Co-I: Justin Ziemba, MD, MSEd. Study Coordinators: Emily Funsten, Adam Mussell, Rebecca McCune, Salima Shah, Arushi Jain, Antoine Selman-Fermin.
University of Texas Southwestern Medical Center, Dallas, TX: PI: Naim M. Maalouf, MD; Jodi A. Antonelli, MD. Co-I: Brett A. Johnson, MD; Margaret S. Pearle, MD, PhD; Linda A. Baker, MD. Study Coordinators: Brooke Piskator, Joyce Obiaro, Cynthia Rangel, Martinez Hill.
University of Washington, Seattle, WA: PI: Jonathan D. Harper, MD; Hunter Wessells, MD. Co-I: Michele Curatolo, MD; Todd Edwards, PhD; Mathew Sorensen MD. Collaborator: Robert Sweet, MD. Study Coordinators: Tristan Baxter, Holly Covert, Elsa Ayala, Lisa Flint.
Washington University in St. Louis, St. Louis, MO: PI: Alana C. Desai, MD; H. Henry Lai, MD. Co-I: Kefu Du, MD. Study Coordinators: Susan Mueller, RN; Linda Black, RN; Aleksandra Klim, RN.
Scientific Data Research Center
Duke Clinical Research Institute, Duke University, Durham, NC: PI: Charles D. Scales, Jr, MD, MSHS; Hussein R. Al-Khalidi, PhD. Co-I: Amy Corneli, PhD; Bryce Reeve, PhD; Kevin Weinfurt, PhD. Statistician: Honqiu Yang, PhD. STENTS Project Lead: Davy Andersen. USDRN Project Lead: Laura Johnson. Lead CRA: Andrew Dodd. Data Manager: Omar Thompson. Qualitative Research Core: Carrie Dombeck, Kevin McKenna, Teri Swezey.
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)
Project Scientist: Ziya Kirkali, MD. Program Official: Christopher Mullins, PhD.
Author Disclosure Statement
Dr. Antonelli reported relationships with the following entities: Boston Scientific Corp, Cook Medical (Advisory Board). Dr. Tasian reported relationships with the following entities: Dicerna (advisory board, scientific study), Alnylam (advisory board), Novome (advisory board), and Allena Pharmaceuticals (consultant). No other authors reported disclosures relevant to this article.
Funding Information
This research was supported by the National Institutes of Health/NIDDK, as follows: U01DK110961 (University of Pennsylvania/Children's Hospital of Pennsylvania to P.P.R. and G.E.T.), U01KD110986 (Washington University St. Louis to A.D. and H.H.L.), U01DK110994 (University of Texas Southwestern to N.M.M.), U01DK110954 (University of Washington to J.D.H. and H.W.), and U01DK110988 (Duke University to C.D.S. and H.R.A.).
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.