
Abstract
Aims:
To compare outcomes of monopolar vs bipolar transurethral resection of the prostate (TURP) in the management of exclusively moderate-large volume prostatic hyperplasia in terms of maximum flow rate as a surrogate for clinical efficacy, duration of catheterization, hospital stay, operative time, resection weight, transurethral resection (TUR) syndrome, acute urinary retention (AUR), clot retention, and blood transfusion.
Methods:
We conducted a search of electronic databases (PubMed, MEDLINE, EMBASE, CINAHL, and CENTRAL), identifying studies comparing the outcomes of monopolar and bipolar TURP in the management of large-volume prostatic hyperplasia. The Cochrane risk-of-bias tool for randomized controlled trials (RCTs) and the Newcastle–Ottawa scale for observational studies were used to assess included studies. Random effects modeling was used to calculate pooled outcome data.
Results:
Three RCTs and four observational studies were identified, enrolling 496 patients. No difference was observed in the clinical efficacy between each procedure at 3 months postoperatively (p = 0.99), 6 months (p = 0.46), and 12 months (p = 0.29). The use of bipolar TURP was associated with significantly shorter inpatient stay (p = 0.01) and a shorter duration of catheterization (p = 0.05). Monopolar TURP was associated with an increased risk of TUR syndrome (p = 0.03). Operative time (p = 0.58), resection weight (p = 0.16), AUR (p = 0.96), clot retention (p = 0.79), and blood transfusion (p = 0.39) were similar in both groups.
Conclusion:
Our meta-analysis demonstrated that bipolar TURP in the treatment of moderate-large volume prostatic disease may be associated with a significantly lower rate of TUR syndrome and shortened length of hospital stay, with similar efficacy when compared with monopolar TURP. Further high-quality RCTs with adequate sample sizes are required to compare both monopolar and bipolar TURP to open prostatectomy or laser enucleation in the treatment of exclusively large-volume prostates with stricter definition of size.
Introduction
Prostatic hyperplasia is defined as the progressive growth of prostatic tissue, often resulting in troublesome lower urinary tract symptoms (LUTS) caused by bladder outlet obstruction. The condition is of increased prevalence with advancing age and is, therefore, only expected to become more commonplace as a consequence of an aging population. 1,2
Various surgical modalities exist for the treatment of LUTS secondary to prostatic hyperplasia. For the treatment of moderate-severe symptoms with prostatic volume of 30 to 80 mL, transurethral resection of the prostate (TURP) continues to prove the mainstay of treatment. 3 For those with larger volume disease, open prostatectomy or laser enucleation are commonly performed procedures. However, it has been demonstrated that TURP has comparable outcomes to open prostatectomy or laser enucleation in the management of larger prostates. 4 –9 Furthermore, similar efficacy of TURP has been reported in the treatment of small- and large-sized prostates. 10 –12 Nevertheless, the available evidence regarding different types of TURP techniques in the management of exclusively large-volume prostates is limited.
Although previous meta-analyses evaluated comparative outcomes of monopolar and bipolar TURP for small- or intermediate-sized disease, 13 –16 no comprehensive meta-analysis investigated such comparison in the treatment of solely moderate-large volume prostates, with 50 mL acting as the minimum size of prostate included in this study. We aimed to perform a systematic review and meta-analysis of comparative studies to evaluate the outcomes of monopolar and bipolar TURP in the treatment of moderate-large volume prostates.
Methods
The criteria for study selection, method of analysis, data extraction, and analysis of outcomes were defined in the study protocol. We performed this study according to standards conforming to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 17
Eligibility criteria
All randomized controlled trials (RCT) and comparative observational studies evaluating the outcomes of monopolar vs bipolar TURP in the treatment of moderate-large volume prostates were considered eligible. The study population consisted of adult men of any age, with a minimum prostate size as felt appropriate to accurately demonstrate both intermediate- and large-volume disease. This cutoff was set at 50 mL or 50 g, with both units of measurement considered because of lack of congruity between studies with regard to the units of measurement. Only the studies that included patients with prostate size of >50 g, or >50 mL were considered for analysis. Any studies that included patients with prostate sizes below this threshold would, therefore, be excluded. Bipolar TURP was considered as the intervention of interest and monopolar TURP was considered as the comparator.
Outcome measures
The efficacy of each procedure was considered as the primary outcome measure. Efficacy was measured by the postoperative maximum urinary flow rate (Qmax). The secondary outcome measures included length of catheterization, length of hospital stay, procedure duration, weight of resection, the incidence of transurethral resection (TUR) syndrome, acute urinary retention (AUR), clot retention, requirement for postoperative blood transfusion, and patient-reported International Prostate Symptom Score (IPSS).
Systematic search strategy
A comprehensive search strategy was devised, and a literature search performed by two independent authors through PubMed, MEDLINE, EMBASE, CINAHL, and CENTRAL. The literature search strategy is outlined in Appendix A1. The last search was run on the 19th of February 2020.
The title and abstract of articles found on a search of the aforementioned databases were assessed initially on the title, and then abstract to identify suitable studies. If required, the full texts of relevant articles were retrieved and evaluated against the inclusion criteria for the study. In the case of discrepancies between the two searching authors, a third author's opinion was sought to reach a majority verdict.
Data extraction
Using the Cochrane recommendations for intervention reviews, a data extraction spreadsheet was produced. Information was extracted from each of the included studies by two independent reviewers. This comprised study-related data (first author, year of publication, journal, country of origin, study design, units of measurement to define prostate size, sample size), baseline demographics of the study populations (age, baseline prostate-specific antigen [PSA], baseline IPSS, baseline Qmax, prostate size, and/or volume), and primary and secondary outcome data.
Summary measures and synthesis
For measured continuous variables (serial Qmax, length of catheterization, hospital stay duration, operative time, resection weight, and IPSS), the mean difference (MD) between each group was calculated. For dichotomous variables (incidence of TUR, AUR, clot retention, and postoperative blood transfusion), the odds ratio (OR) was established as the summary measure. The OR is the odds of an event in the bipolar group compared with the monopolar group. In the analysis of Qmax, an OR of >1 would favor the monopolar group. In the analysis of incidence of TUR syndrome, AUR, clot retention, or postoperative blood transfusion, an OR of <1 would favor the monopolar group.
Two independent review authors extracted data into Review Manager 5.3 software for data synthesis. 18 Random effects modeling was used for the analysis. All results are presented in a forest plot with 95% confidence intervals (CIs).
The statistical heterogeneity and calculation of inconsistency was assessed using the I 2 statistic. Zero percent to 50% represents mild heterogeneity; 50% to 75% moderate; 75% to 100% substantial heterogeneity.
In addition, sensitivity analysis was performed to further evaluate the sources of heterogeneity and assess the robustness of our results. For each dichotomous variable the pooled OR, risk ratio (RR) and risk difference (RD) were estimated to identify the possible alteration in direction of pooled effect size. The effect of each study was also evaluated, by assessing the resultant effect when removing one study at a time (leave-one-out sensitivity analysis).
Results
Our literature search resulted in 642 articles. Ultimately, a total of seven studies 7 –9,19–22 (three RCTs, 19,20,22 four retrospective observational studies 7 –9,21 ) met the eligibility criteria of this review (Fig. 1). The included studies reported a total of 496 patients of whom, 244 underwent monopolar TURP and 252 had bipolar TURP.
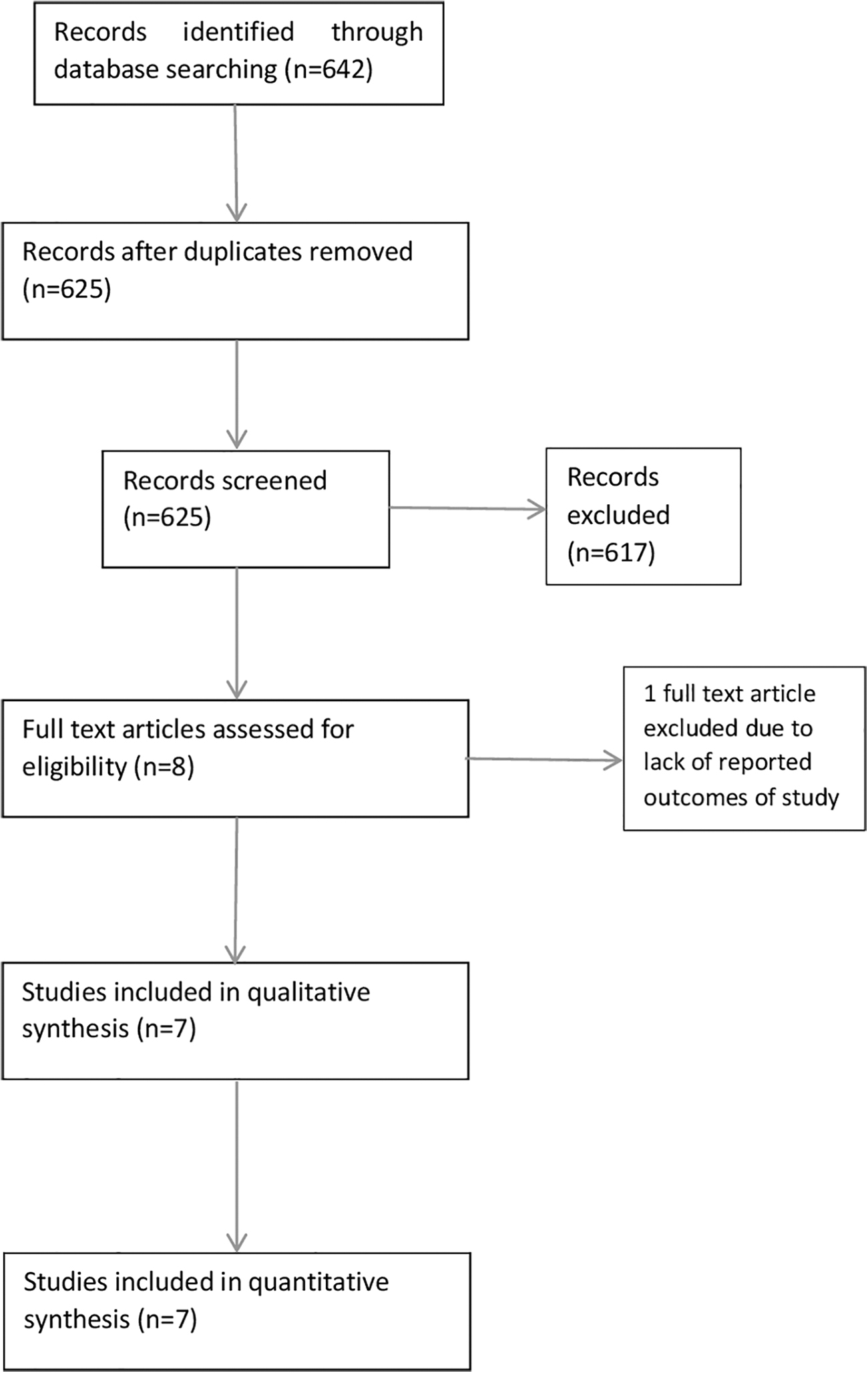
Study flow diagram.
Table 1 presents the baseline characteristics of the included studies, specifying the first author, year of publication, journal, study design, and minimum prostatic size/volume included. Table 2 further outlines the baseline demographics of the included patients, with the total number of patients having each intervention and their associated preoperative variables (age, PSA, IPSS, Qmax, and prostate size/volume). Of included studies, the mean prostatic size of patients was 108.46 g for those who recorded prostatic size in grams, and 98.04 mL in the remainder. The preoperative demographics were comparable across each of the studies, with similar age, baseline PSA, and IPSS observed across each of the included studies.
Baseline Characteristics of Included Studies
LUTS = lower urinary tract symptoms; RCT = randomized controlled trial.
Baseline Demographics of Included Studies
IPSS = International Prostate Symptom Score; NR = not reported; PSA = prostate-specific antigen; Qmax = maximum urinary flow rate.
Methodologic quality and risk of bias
Two independent authors conducted a methodologic quality and risk of bias on each of the included articles. The Cochrane tool and Newcastle–Ottawa scale were used to assess the risk of bias of randomized trials and observational studies, respectively. The summary of and results of the methodologic quality assessment is displayed in Figure 2 for randomized trials, and Table 3 for observational studies.
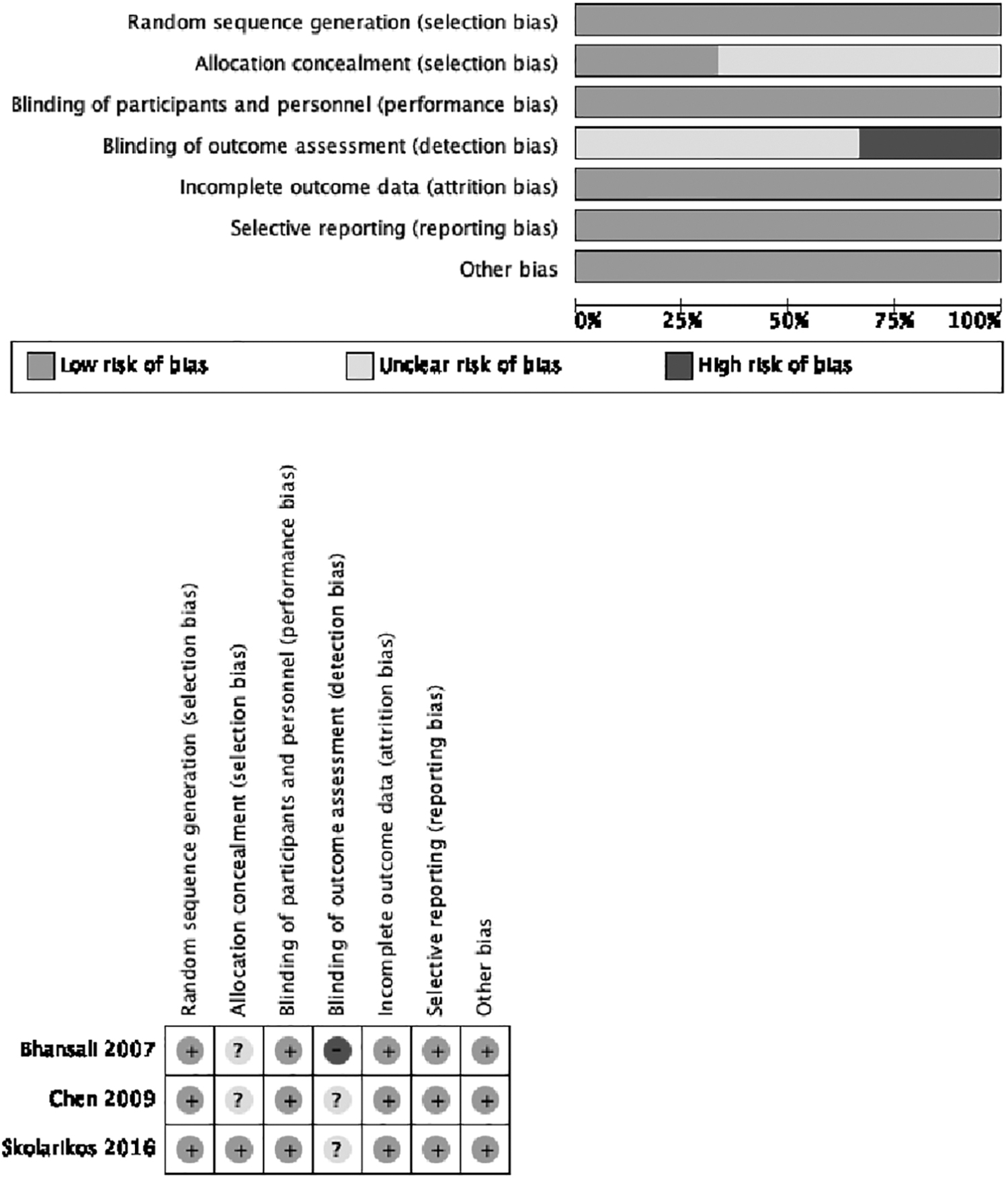
Methodologic quality of included randomized controlled trials.
Methodologic Quality of the Observational Studies Assessed with the Newcastle–Ottawa Scale
Each column allocated maximum of 1 *, aside from ‘Comparability of cohorts’ (maximum 2 *'s).
Regarding the RCTs, the risk of selection bias for the random sequence generation was low in all studies. However, the risk of selection bias regarding the allocation concealment was unclear in two studies. 19,20 The risk of attrition bias and reporting bias were low in all studies. Although the performance bias was low in all studies, the detection bias was unclear in two studies 20,22 and high in one study. 19 Regarding the observational studies, the risk of bias was low in three studies 7,9,21 and moderate in one study. 8
Outcome synthesis
Primary outcome (efficacy)
Data on efficacy were measured by the impact of each procedure on Qmax at 3-, 6-, and 12-month follow-ups.
Qmax at 3 months
Qmax at 3-month follow-up was reported by four studies 9,19 –21 enrolling a total of 245 patients (Fig. 3a). The mean Qmax at 3 months in the monopolar and bipolar groups were 20.64 ± 3.11 and 19.31 ± 2.70, respectively. There was no statistically significant difference in Qmax at 3 months between the two groups (MD 0.01, 95% CI −1.22 to 1.24, p = 0.99). Low heterogeneity existed among the included studies (I 2 = 12%, p = 0.33).
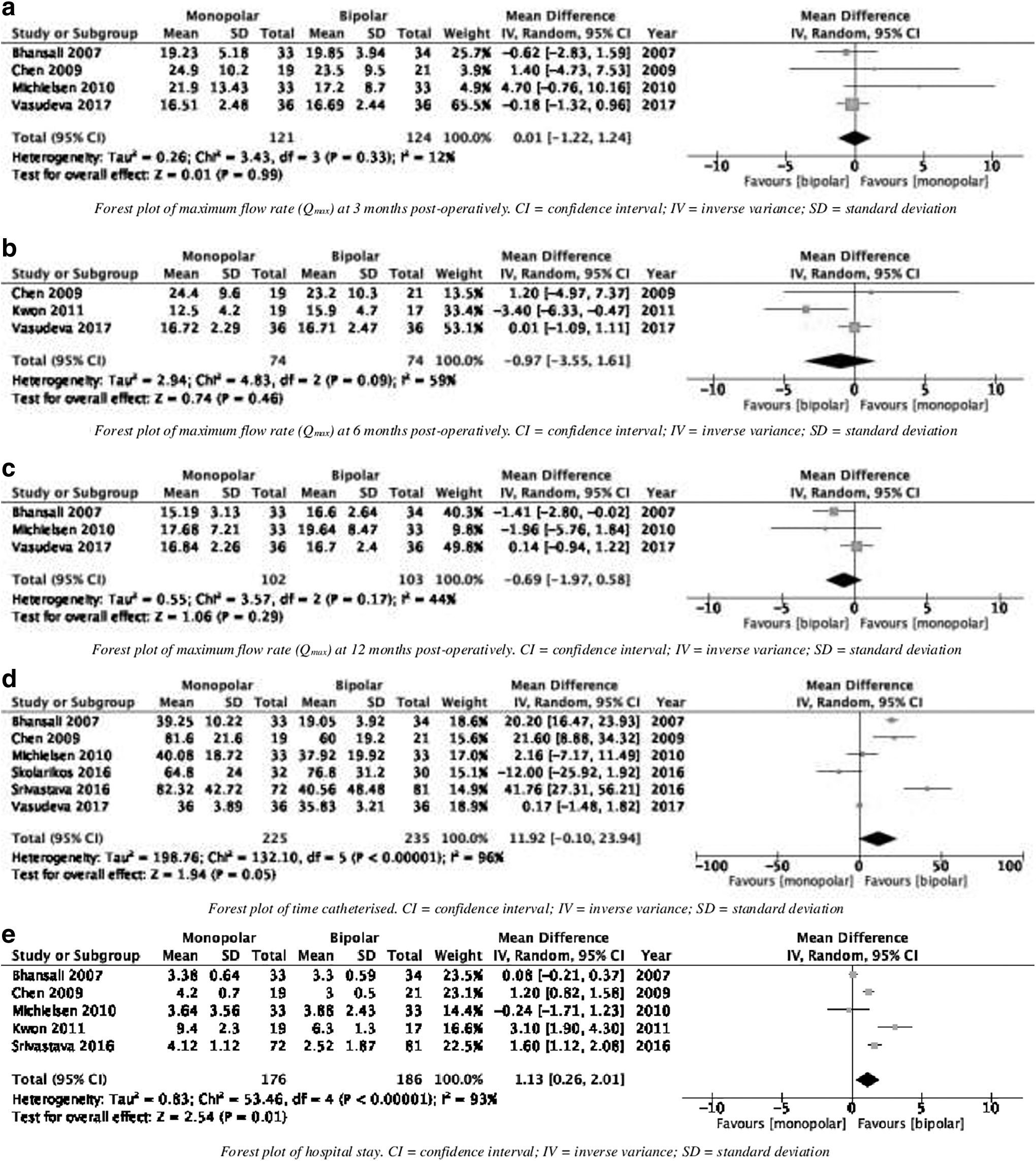
Forest plots.
Qmax at 6 months
Three studies 7,9,20 (148 patients) reported Qmax at 6-month follow-up (Fig. 3b). The mean Qmax at 6 months was 17.87 ± 4.93 in the monopolar group, whereas it was 18.60 ± 3.27 in the bipolar group. There was no significant difference in Qmax outcomes at 6 months between the monopolar and bipolar groups (MD −0.97, 95% CI −3.55 to 1.61, p = 0.46). Moderate between-study heterogeneity existed (I 2 = 59%, p = 0.09).
Qmax at 12 months
Three studies 9,19,21 enrolling 205 patients, reported Qmax at 12-month follow-up (Fig. 3c). The mean Qmax at 12 months in the monopolar group was 16.57 ± 1.03 and it was 17.65 ± 1.41 in the bipolar group. The pooled analysis did not find any significant difference in Qmax at 12 months between the two groups (MD −0.69, 95% CI −1.97 to 0.58, p = 0.29). The between-study heterogeneity was moderate (I 2 = 44%, p = 0.17).
Secondary outcomes
Duration of catheterization
The mean duration of catheterization was reported in six studies, 8,9,19 –22 enrolling a total of 560 patients (Fig. 3d). The mean catheterization time in the monopolar and bipolar groups were 57.3 ± 19.8 hours and 45.0 ± 18.5 hours, respectively. The use of bipolar approach was associated with a marginally significant decrease in duration of catheterization when compared with the monopolar approach (MD 11.92, 95% CI −0.10 to 23.94, p = 0.05). A high-level heterogeneity among the analyzed studies was detected (I 2 = 96%, p < 0.00001).
Length of stay
The mean length of stay was reported in five studies 7,8,19 –21 enrolling a total of 362 patients (Fig. 3e). The mean length of stay in the monopolar group was 4.95 ± 2.25 days, and it was 3.80 ± 1.33 days in the bipolar group. Bipolar TURP was associated with significantly shorter length of hospital stay compared with monopolar TURP (MD 1.13, 95% CI 0.26 to 2.01, p = 0.01). A high level of heterogeneity among the analyzed studies was detected (I 2 = 93%, p < 0.00001).
Operative time
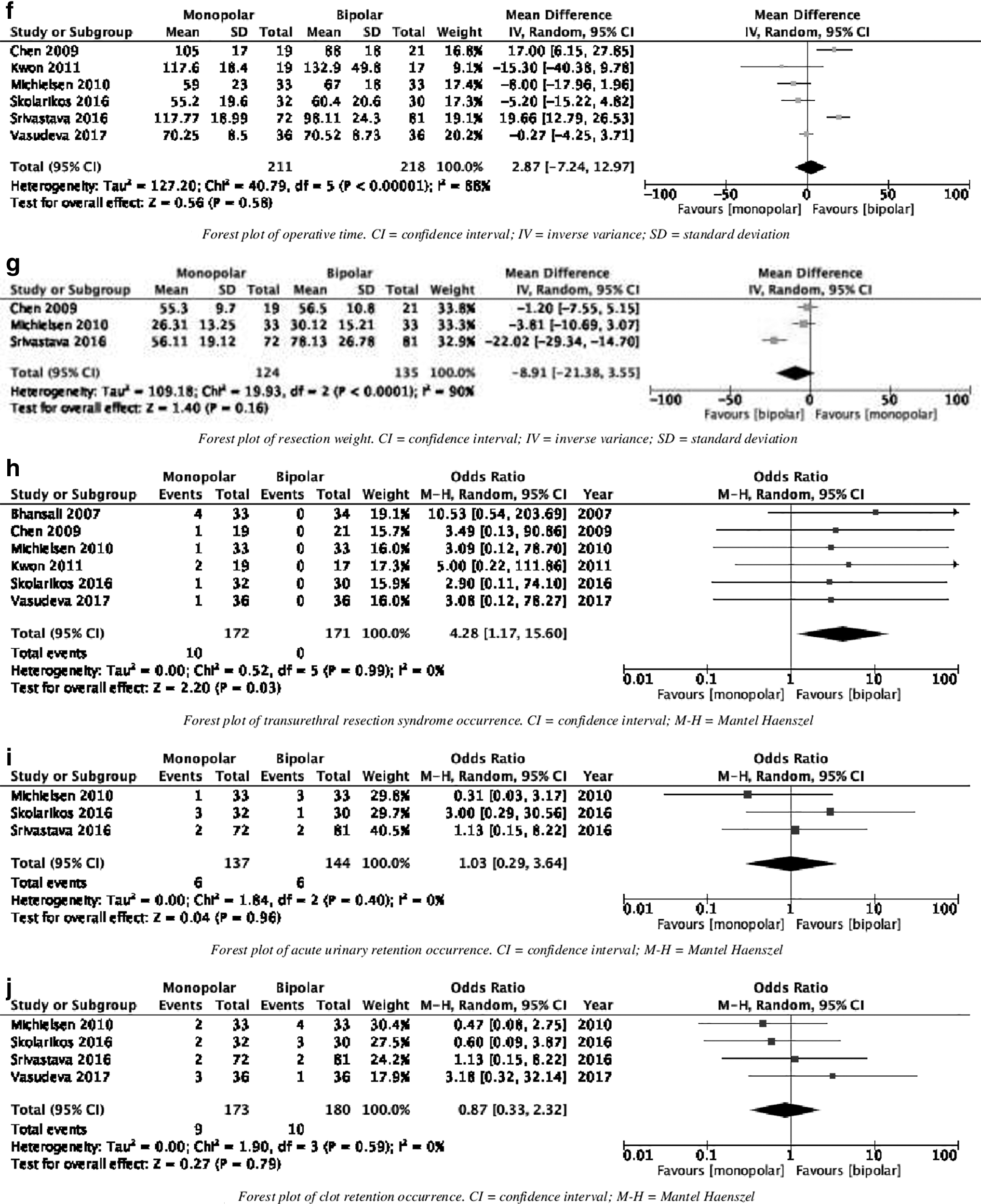
The operative time was reported in six studies, 7 –9,20–22 enrolling a total of 429 patients (Fig. 3f). The mean operative time in the monopolar group was 87.5 ± 26.7 minutes, and it was 86.2 ± 24.5 minutes in the bipolar group. There was no statistically significant difference in operative time between the two groups (MD 2.87, 95% CI −7.24 to 12.97, p = 0.58). A high level of heterogeneity among the analyzed studies was detected (I 2 = 88%, p < 0.00001).
Resection weight
The resection weight was reported in three studies, 7,9,19 –22 enrolling a total of 259 (Fig. 3g). The mean resection weight in the monopolar group was 45.9 ± 13.9 g, and it was 54.9 ± 19.6 g in the bipolar group. There was no statistically significant difference in the resection weight between the two groups (MD −8.91, 95% CI −21.38 to 3.55, p = 0.16). A high level of heterogeneity among the analyzed studies was detected (I 2 = 90%, p < 0.00001).
TUR syndrome
The incidence of TUR syndrome was reported in six studies, 7,9,19 –22 enrolling a total of 343 patients (Fig. 3h). The rate of TUR in the monopolar group was 5.8%, whereas there were no reported cases in the bipolar group. Monopolar TURP was associated with significantly higher risk of TUR when compared with bipolar TURP (OR 4.28, 95% CI 1.17 to 15.60, p = 0.03). A low level of heterogeneity existed among the included studies (I 2 = 0%, p = 0.99).
Acute urinary retention
The incidence of AUR was reported in three studies, 8,21,22 enrolling a total of 281 patients (Fig. 3i). The rate of AUR in the monopolar and bipolar groups were 4.4% and 4.2%, respectively. There was no statistically significant difference in the risk of AUR between the two groups (OR 1.03, 95% CI 0.29 to 3.64, p = 0.96). A low level of heterogeneity among the studies existed (I 2 = 0%, p = 0.40).
Clot retention
The incidence of clot retention was reported in four studies, 8,9,21,22 enrolling a total of 353 patients (Fig. 3j). The rate of clot retention in the monopolar group was 5.2%, whereas it was 5.6% in the bipolar group. There was no statistically significant difference in the risk of clot retention between the two groups (OR 0.87, 95% CI 0.33 to 2.32, p = 0.79). A low level of heterogeneity among the studies existed (I 2 = 0%, p = 0.83).
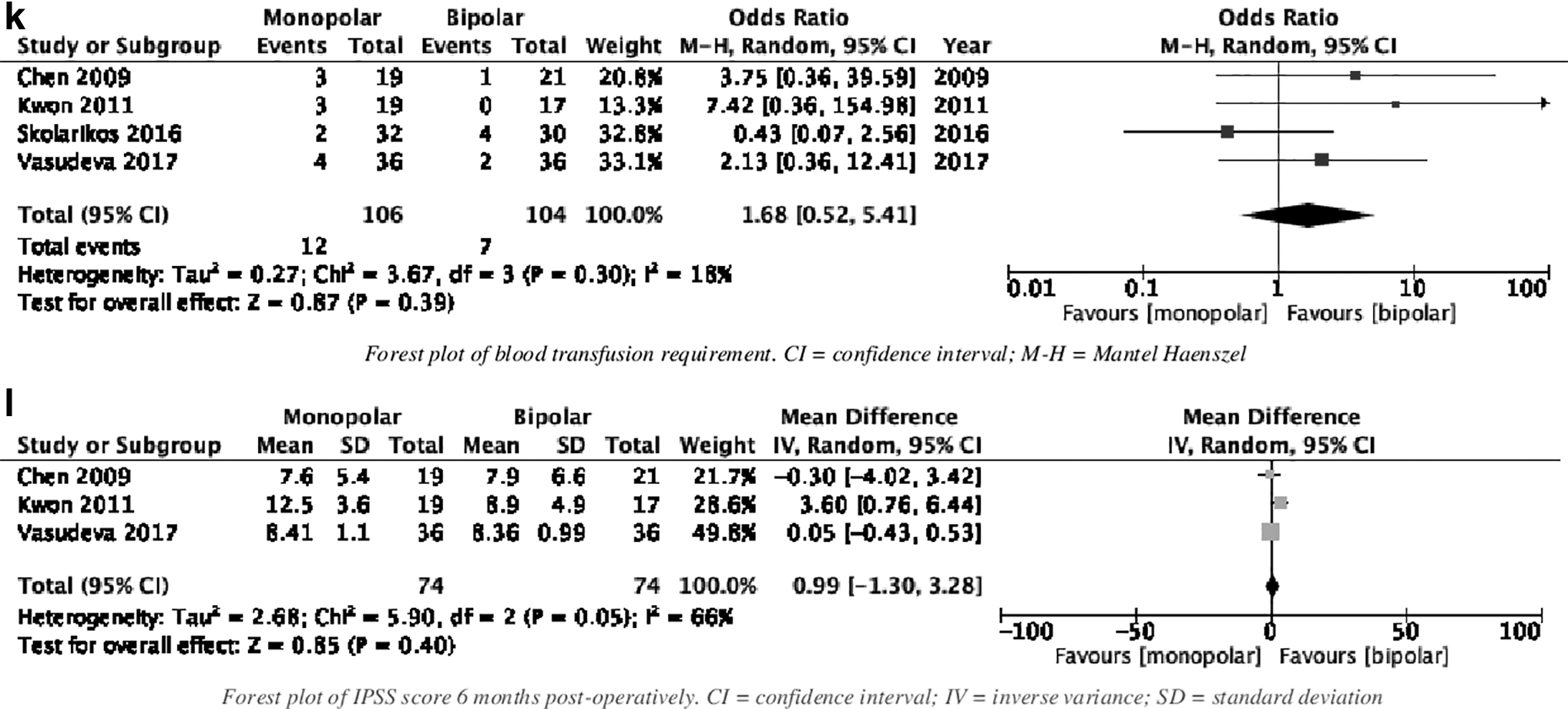
Blood transfusion
The incidence of requiring a blood transfusion postoperatively was reported in four studies, 7,9,20,22 enrolling a total of 210 patients (Fig. 3k). The rate of blood transfusion requirement in the monopolar and bipolar groups were 11.3% and 6.7%, respectively. There was no statistically significant difference in the need for blood transfusion between the two groups (OR 1.68, 95% CI 0.52 to 5.41, p = 0.39). A low level of heterogeneity among the studies existed (I 2 = 18%, p = 0.30).
International Prostate Symptom Score
Patient reported IPSS 6 months postoperatively was reported in three studies, 7,9,20 enrolling a total of 148 patients (Fig. 3l). The mean IPSS 6 months postoperatively was 9.25 ± 1.94 in the monopolar group, and 8.35 ± 0.36 in the bipolar group. There was no statistically significant difference in the IPSS at 6 months postoperatively between the two groups (MD 0.99, 95% CI −1.30 to 3.28, p = 0.40). A moderate level of heterogeneity among the studies was detected (I 2 = 66%, p = 0.05).
Sensitivity analysis
The use of random-effects or fixed-effects model did not significantly alter calculated outcomes from continuous data. The direction of pooled effect remained unchanged when OR, RR, or RD were calculated from dichotomous variables. After one-leave out sensitivity analysis, removal of the study Skolarikos and colleagues 22 or Vasudeva and colleagues 9 reduced the duration of catheterization in favor of the bipolar group more significantly (MD 16.19, 95% CI 3.03 to 29.35, p = 0.02; MD 14.95, 95% CI 0.94 to 28.36, p = 0.04, respectively). The individual removal of Chen and colleagues, 20 Kwon and colleagues, 7 or Srivastava and colleagues 8 affected the direction of pool size in the analysis of length of hospital stay and made the results insignificant (MD 1.13, 95% CI −0.12 to 2.38, p = 0.08; MD 0.76, 95% CI −0.09 to 1.61, p = 0.08; MD 1.00, 95% CI −0.03 to 2.04, p = 0.06, respectively). Moreover, in the analysis of TUR syndrome, removal of study Bhansali and colleagues 19 made the results statistically insignificant (OR 3.46, 95% CI 0.82 to 14.58, p = 0.09).
Discussion
We performed a systematic review and meta-analysis of reported outcomes for monopolar and bipolar TURP in the management of exclusively moderate-large volume prostatic hyperplasia. We included seven comparative studies, enrolling a total of 496 patients, of whom 244 underwent monopolar TURP and the remaining 252 had bipolar TURP. Our analyses demonstrated that the use of bipolar TURP was associated with a significantly reduced incidence of TUR syndrome and length of hospital stay compared with the monopolar approach. There was a marginally significant reduction in duration of catheterization in those patients having bipolar TURP, rather than monopolar. However, there was no significant difference in the efficacy of TURP (using Qmax as a unit of measurement), operative time, resection weight, IPSS measured 6 months postoperatively, and frequency of adverse effects such as AUR, clot retention, or the requirement for a postoperative blood transfusion between the monopolar and bipolar groups. The between-study heterogeneity was low-moderate, and the quality of the evidence was moderate.
To the best of our knowledge this is the first meta-analysis comparing outcomes of monopolar and bipolar TURP in the treatment of exclusively moderate-large volume prostate glands, with an incorporated minimum cutoff size adopted. Previous meta-analyses have compared monopolar and bipolar TURP in the treatment of small-moderate sized prostates.
The cutoff we adopted for a moderate-large sized prostate was set as a minimum of 50 g or 50 mL. Both values were used because of the heterogeneity of the definition of “moderate-large” prostate within the literature. The use of 50 mL enabled us to narrow and focus on solely intermediate-larger sized prostates. European Association of Urology guidelines 3 have recently set a cutoff of 80 mL volume as a definition of “large” prostate and included TURP as one of the recommended modalities for surgical treatment. Of note, our review had an average prostatic size of included patients of 108.46 g or 98.04 mL. This is a far larger average than previous systematic reviews, or meta-analyses, which have included patients with a lower average prostate size.
Alexander and colleagues 13 performed a large systematic review of 59 RCTs, comparing bipolar vs monopolar TURP for LUTS secondary to prostatic hyperplasia. The included prostate volumes ranged from 39 to 82.6 mL. Consistent with our findings, the authors concluded that bipolar TURP demonstrated no statistically significant difference in clinical efficacy, in comparison with monopolar TURP (as measured by IPSS 12 months postoperatively). The findings of no significant difference in clinical efficacy were echoed by smaller reviews performed by Omar and colleagues 14 and Mamoulakis and colleagues 15 In contrast, Tang and colleagues 16 claimed a clinically relevant difference in efficacy in favor of bipolar technique, although they had no statistical proof of such finding (p = 0.12).
Our findings indicate that bipolar TURP is associated with significantly lower rate of TUR syndrome when compared with monopolar TURP. In our meta-analysis, the rate of TUR syndrome in the monopolar TURP group was 5.8%. This is higher than the figure reported in the large-scale review by Alexander and colleagues, 13 who found that 2.4% of those having monopolar TURP developed TUR syndrome. Although the total cohort included in our study is smaller, a reciprocal increased risk of TUR syndrome is expected when dealing with larger volume prostates caused by the increased quantity of fluid shift during resection with nonconductive fluids. There were no substantial data in our included studies regarding amount of irrigation fluid used. Links have been established previously between the increased volume of irrigation fluid and the incidence of TUR syndrome. 23 –25 The decreased risk of TUR syndrome represents one of the major advantages of bipolar TURP over monopolar.
Although risk factors for TUR syndrome include operative time, 24 –27 resection weight, 24,25 and blood loss, 23 –26 our review found no difference in incidence related to these factors. However, there was heterogeneity in the data with regard to resection time and weight of resected tissue.
Although the difference in resection weight did not reach statistical significance, the quantity of tissue resected is ∼9 g more in the bipolar group, with comparison with the monopolar group. Despite this, no difference was observed in the primary measured outcome (maximum flow rate) in respective pooled analysis.
Patients having bipolar TURP had shorter inpatient stay and marginally shorter duration of catheterization in our study. The reduction in hospital inpatient stay and duration of catheterization has beneficial effects for both clinician and patient; allowing the patient to return home early, reducing their risk of developing hospital-acquired infections, and providing a financial saving to health care providers. This, along with the reduced risk of TUR syndrome in those having bipolar TURP, should make it the procedure of choice in those who elect to have TURP for their troublesome LUTS secondary to prostatic hyperplasia.
Our findings confirm that both modalities are effective in the treatment of prostatic hyperplasia, still maintaining the gold standard for surgical management of benign prostatic enlargement. Bipolar TURP holds the advantage of having an improved safety profile, with reduced incidence of TUR syndrome, as well as the association of shortened length of hospital stay and reduced time of catheterization. Bipolar TURP is a suitable choice for patients with large-volume prostates, factoring in patient choice and surgeon preference.
Our review and the reported outcomes have limitations. Only three studies were RCTs, to provide high-level evidence on outcomes of monopolar and bipolar TURP in the management of exclusively intermediate-large volume prostatic hyperplasia. Of the included studies, four had nonrandomized design and are, therefore, at an inevitably increased risk of selection bias. Furthermore, some of the included studies had small sample sizes that may subject our study results to type 2 error. With regard to the incidence of blood transfusion requirement or the event of clot retention, no data were provided regarding the preoperative anticoagulant status of patients involved in the relevant studies.
Conclusion
Our meta-analysis demonstrated that bipolar TURP in the treatment of moderate-large volume prostatic disease may be associated with a significantly lower rate of TUR syndrome and shortened length of hospital stay, with similar efficacy when compared with monopolar TURP. Further high-quality RCTs with adequate sample sizes are required to compare both monopolar and bipolar TURP with open prostatectomy or laser enucleation in the treatment of exclusively large-volume prostates with stricter definition of size.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Abbreviations Used
Appendix
Appendix A1. Literature Search Strategy
| Search No. | Search strategy * |
|---|---|
| #1 | MeSH descriptor: [transurethral resection of prostate] explode all trees |
| #2 | Transurethral resection of prostate: TI,AB,KW |
| #3 | MeSH descriptor: [TURP] explode all trees |
| #4 | TURP: TI,AB,KW |
| #5 | MeSH descriptor: [monopolar] explode all trees |
| #6 | Monopolar: TI,AB,KW |
| #7 | MeSH descriptor: [bipolar] explode all trees |
| #8 | Bipolar: TI,AB,KW |
| #9 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 |
| #10 | MeSH descriptor: [benign prostatic hyperplasia] explode all trees |
| #11 | Benign prostatic hyperplasia: TI,AB,KW |
| #12 | MeSH descriptor: [bladder outlet obstruction] explode all trees |
| #13 | Bladder outlet obstruction: TI,AB,KW |
| #14 | #10 OR #11 OR #12 OR #13 |
| #15 | #9 AND #14 |
This search strategy was adopted for following databases: MEDLINE, EMBASE, CINAHL, and the Cochrane Central Register of Controlled Trials (CENTRAL).