
Abstract
Objective:
To evaluate the safety of irreversible electroporation (IRE) for renal ablation adjacent to the ureter or bowel.
Materials and Methods:
Six adult pigs each underwent bilateral IRE of the kidney. To simulate adjacence, the left proximal ureter and duodenum were secured onto the left and right kidney capsule, respectively. Two IRE probes were placed into the renal parenchyma and configured to bridge the ureter and bowel. Therapeutic IRE was delivered at 2000 V/cm for 70 pulses in both forward and reverse polarity. The animal was survived and euthanized at 1, 3, or 14 days. Histopathology was obtained for all potentially injured bowel and ureteral segments. Retrograde pyelogram (RPG) was performed on each left-sided ureter.
Results:
Histologic analysis of the ureter identified reactive changes at the level of the periureteral adipose tissue, which progressed from acute inflammation on day 1 to focal fibrosis by day 14. Urothelial mucosa and surrounding smooth muscle layers were unaffected at all time points. RPGs did not show any abnormalities in all specimens. Histologic analysis of the bowel demonstrated acute inflammation in the serosa and subserosal tissue on day 1. Three days after IRE, inflammation and crypt abscesses were focally present in the deep aspects of the bowel mucosa. Inflammation in the mucosal layer resolved 14 days after IRE.
Conclusions:
In a porcine model of renal IRE, no significant injury was apparent after intentional ablation adjacent to the ureter and bowel. IRE may be a safe alternative to thermal ablation for tumors near the ureter or bowel.
Introduction
Traditional thermal ablation modalities for small renal masses (SRMs) such as radiofrequency ablation (RFA) and cryoablation (CA) use extreme temperatures to destroy target tissue. Tumors adjacent to the ureter or bowel are relative contraindications for use of these modalities because of the risk of thermal collateral damage to these structures. 1,2 Irreversible electroporation (IRE) is a novel ablative technology that works by passing pulsed low-energy direct current through target tissue. These pulses are delivered on the order of microseconds (usually 90 μs) with a variation in the number of pulses delivered (between 70 and 140). This causes cell death by opening pores in the cell membrane, which triggers the cell to lose its intracellular contents. The cells lose homeostasis with the end result being apoptosis. 3,4
The early clinical experience with IRE for renal masses has shown that cancer control is modestly inferior to ablative modalities such as RFA. 5,6 However, IRE may be preferred over thermal ablation for SRMs that are close to the body wall to minimize pain. 7 Since it is primarily a nonthermal mechanism of action, the architecture of the surrounding supportive tissue structures (basement membrane, nerve sheath, etc.) is preserved. This is a desirable feature that can preserve the neighboring tissue architecture and allow cell repopulation. 8 As such, IRE may potentially be employed for tumors adjacent to the ureter or bowel without the need for and complexity of hydrodissection required for thermal ablation. Our objective was to evaluate the safety of IRE in regard to this aspect.
Materials and Methods
The animal study protocol was approved by the Institutional Animal Care and Use Committee at our institution. A flowchart of the protocol is shown in Figure 1. Six adult domestic Yorkshire female pigs weighing from 22 to 32 kg were used. After an appropriate acclimation period, the animals were placed under general anesthesia using intramuscular injection of telazol (3–6 mg/kg) and atropine (0.05 mg/kg) and maintained under inhalational anesthesia using isoflurane 1% to 3% in a 50/50 mixture of nitrous oxide and oxygen. A midline incision was made to enter the peritoneum and expose each kidney. The proximal ureter on the left side was mobilized and the adventitia was secured to the anterior lower pole of the kidney using a 4–0 polyglactin suture. A segment of duodenum that would lie on the right kidney without tension was chosen. The serosa of the bowel was secured using a 4–0 polyglactin suture to the anterior lower pole of the right kidney.
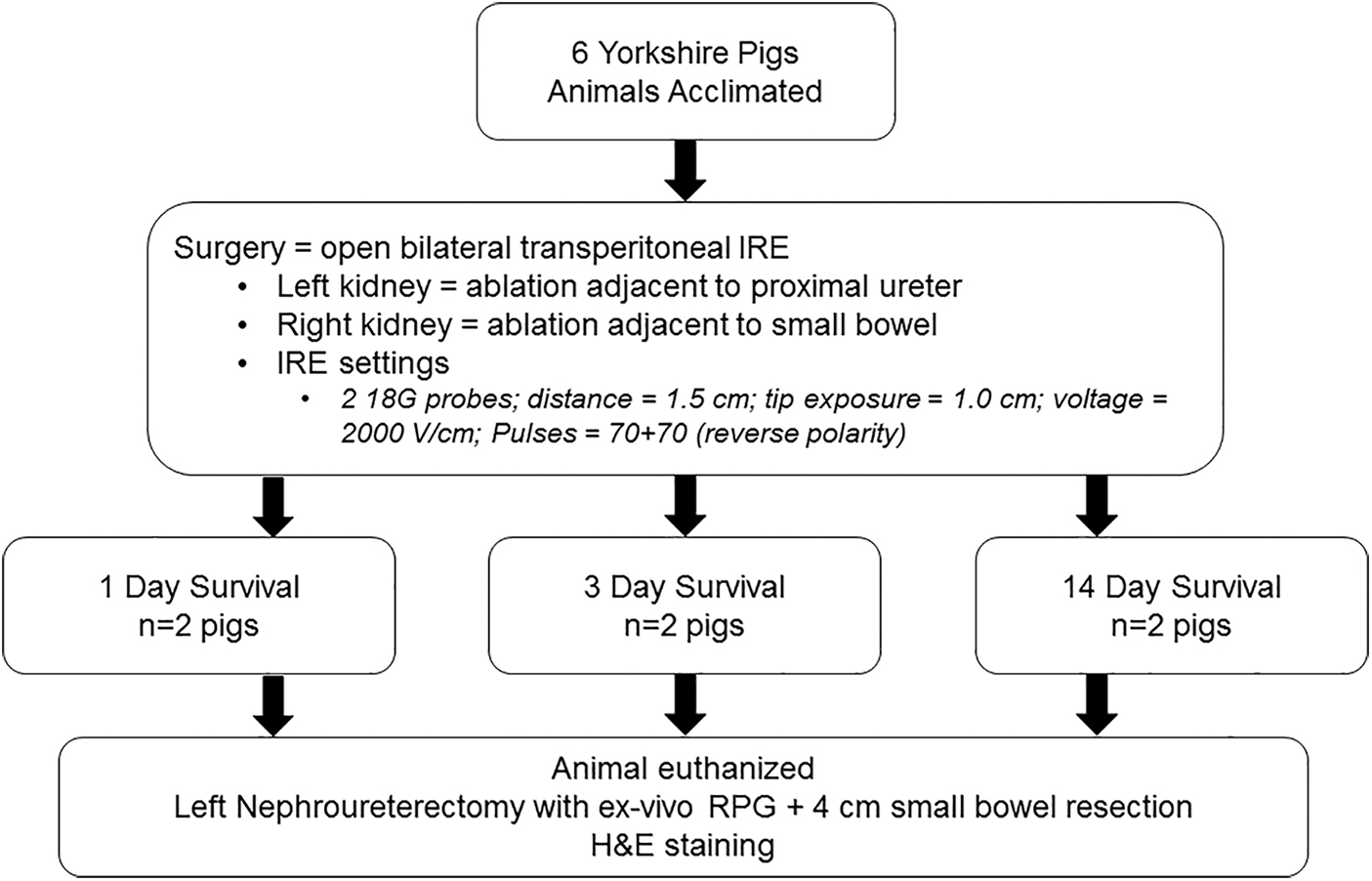
Flowchart of animal IRE protocol. H&E, hematoxylin and eosin; IRE, irreversible electroporation; RPG, retrograde pyelogram.
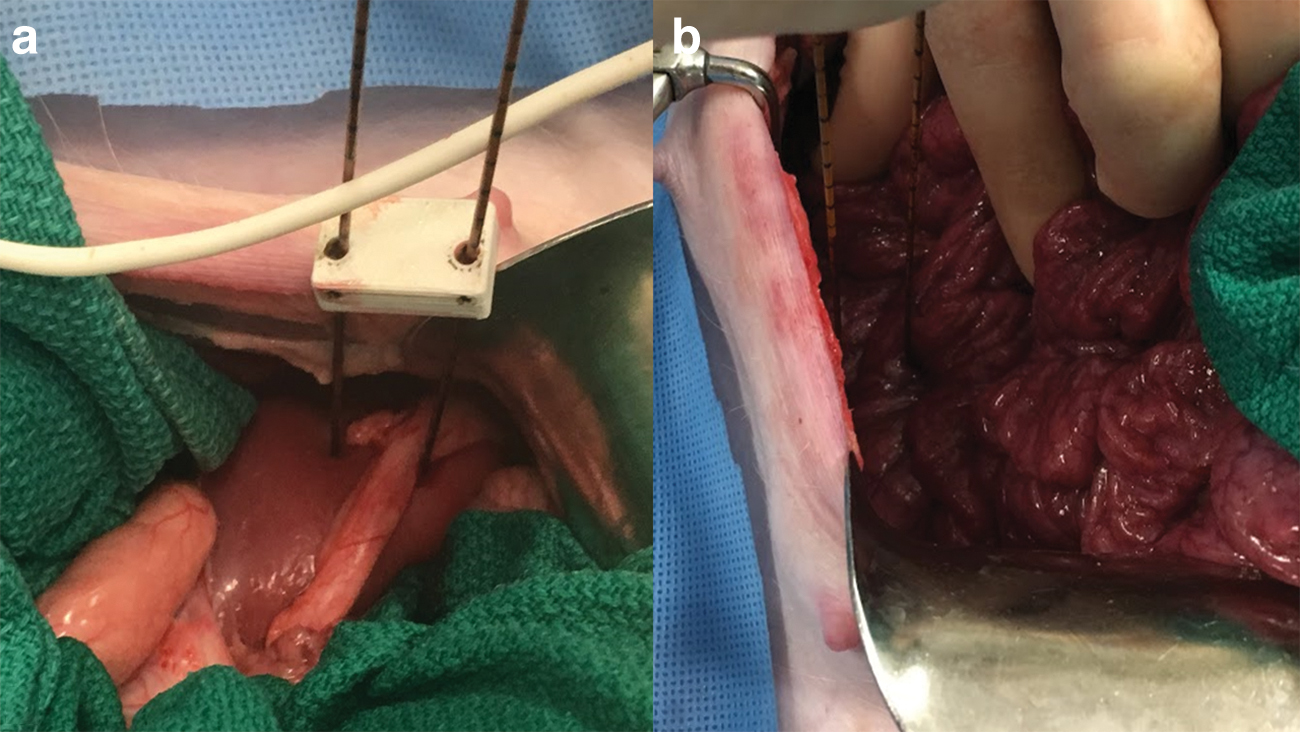
IRE was performed using the NanoKnife® system (AngioDynamics, Latham, NY). Two IRE 18-gauge monopolar probes were inserted into the kidney parenchyma in a configuration to bridge the ureter on the left kidney. The probes were distanced 1.5 cm apart using a spacer with tip exposure of 1.0 cm. Vecuronium (0.1–1 mg/kg) was administered as our paralytic agent before ablation to ensure the probes stayed in place. Once in appropriate position, the generator delivered a test pulse to assure adequate coupling between probes. Energy was then delivered at 2000 V/cm for 70 pulses, gated to the cardiac cycle obtained through electrocardiogram. The polarity of the pulses was then reversed and another 70 pulses were administered at the same voltage. Similar probe placement and ablation was performed on the contralateral kidney with IRE probes placed to bridge the bowel (Fig. 2). These settings are known to result in complete cell death within the treatment volume and are the same settings employed in clinical renal tumor ablation. 5,9 After ablation was completed, the ureter and bowel were freed from the kidney and suture was left on each to help identify the potentially injured segment.
Two pigs were then survived and euthanized at 1 day postablation, two at 3 days postablation, and finally two at 14 days postablation. An exploratory laparotomy was performed immediately after euthanasia and the abdominal contents were examined for gross urinoma, succus, and other major injuries. The ablation zones of the kidney parenchyma were thoroughly evaluated grossly to determine success of ablation on each side. A left-side nephroureterectomy was performed and then a 4 cm segment of the potentially injured bowel was harvested. An ex vivo retrograde pyelogram (RPG) using Isovue®-300 contrast was obtained immediately after nephroureterectomy. The potentially injured segment of the ureter and bowel were fixed, embedded in paraffin, and submitted for hematoxylin and eosin staining done by an experienced pathologist in IRE.
Results
All surgeries were completed effectively without complications. The median IRE current for the left-side kidney was 30Å (range 15–30) and right side was 30Å (range 20–30). After euthanasia, abdominal contents did not reveal evidence of gross urinoma, succus, or other major injuries. The renal parenchyma ablation zones showed the expected gross appearance of an effective ablation using 2000 V/cm at the various times points after IRE. 9 RPGs did not demonstrate adverse pathology at any time points, including ureteral stricture, hydronephrosis, or urine extravasation (Fig. 3). Gross examination of the ureter demonstrated old hematoma surrounding the ureter on day 1, which resolved by day 14.

Ex vivo retrograde pyelogram did not demonstrate any evidence of stricture or hydronephrosis of left ureter at any time point. Black arrow marks the site where ureter was traversing IRE probes. Color images are available online.
Histologic analysis 1 day after IRE showed sections of ureters that demonstrated focal hemorrhage and mild acute inflammation in the periureteral adipose tissue adjacent to the areas of ablation. The urothelial mucosa and smooth muscle layers were unaffected. Three days after IRE, the peripheral aspects of the periureteral adipose tissue demonstrated reactive stromal changes with proliferation of fibroblasts, early fibrosis, neovascularization, mild chronic inflammation, and rare acute inflammatory cells (Fig. 4). Fourteen days after IRE, fibrosis and a suture granuloma were seen in the periureteral adipose tissue. Urothelial mucosa and surrounding smooth muscle layers remained unaffected with no histologic alterations identified (Fig. 5).
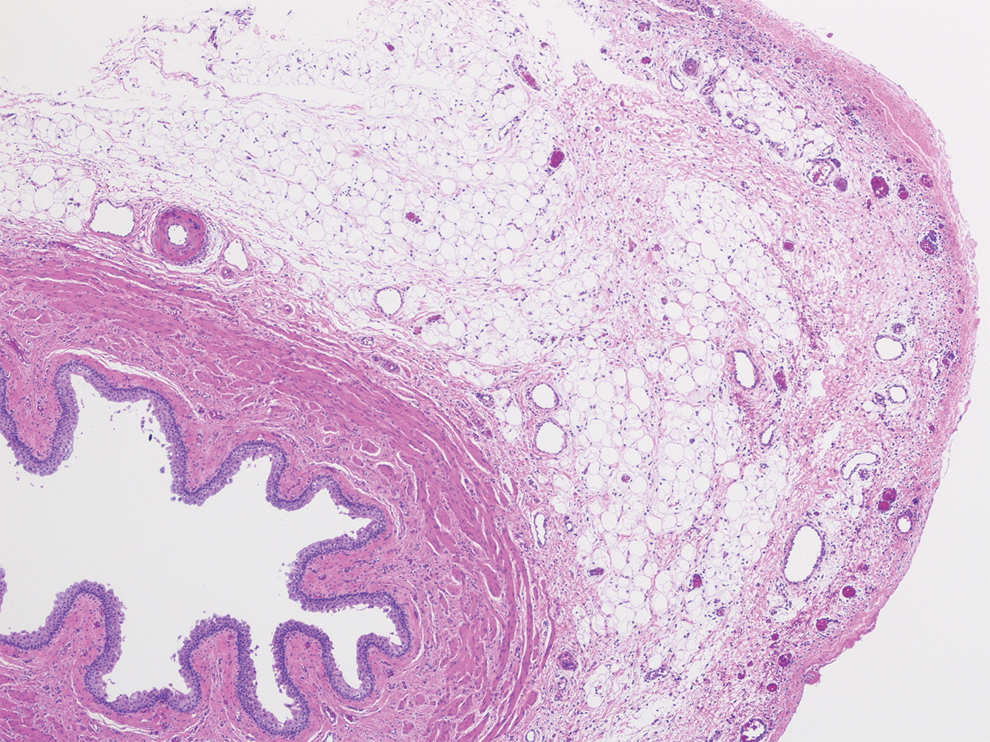
H&E stain of proximal ureter 3 days after IRE. Noted are reactive stromal changes with proliferation of fibroblasts, early fibrosis, neovascularization, mild chronic inflammation, and rare acute inflammatory cells in the periureteral adipose tissue. Color images are available online.
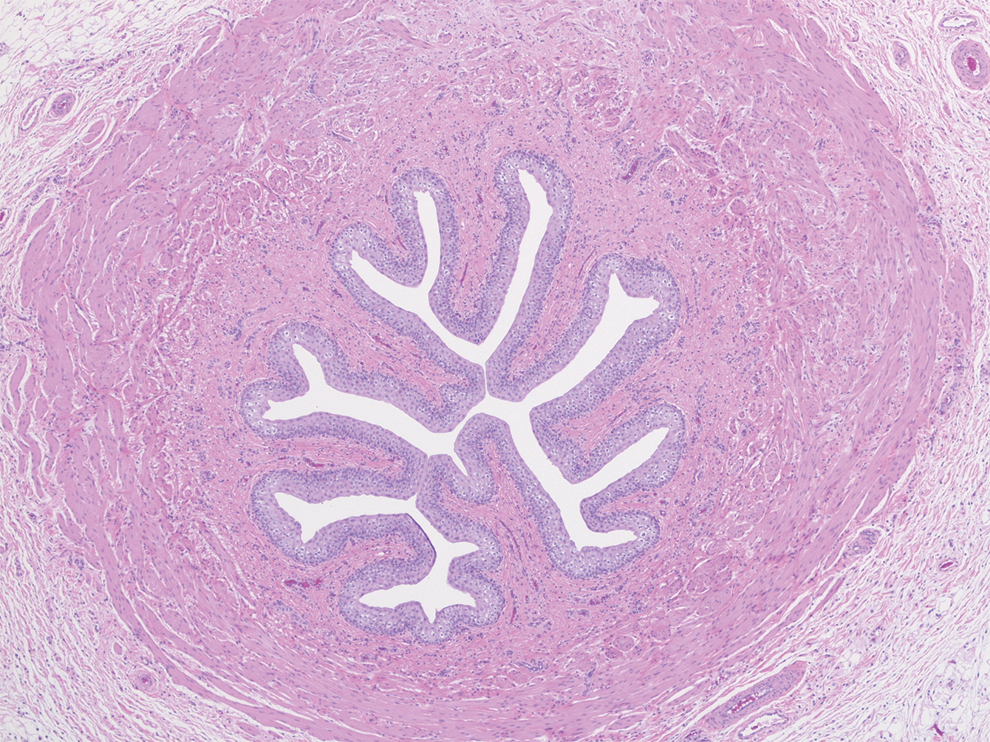
H&E stain of proximal ureter 14 days after IRE demonstrated the urothelial mucosa and surrounding smooth muscle layers remained unaffected. Color images are available online.
Clinically, all pigs were tolerating a regular diet on postoperative day 0 without emesis or change in appetite. There was no gross damage to bowel at any time points. Histologic analysis 1 day after IRE revealed sections of bowel, which demonstrated focal fibrin deposition and acute inflammation in the serosa and subserosal tissue. Three days after IRE, acute and chronic inflammation with fibroblastic stromal response was present in the serosa. R are acute inflammatory cells were seen in the muscularis. Acute inflammation, with neutrophils in the lamina propria, cryptitis, and crypt abscesses were focally present in the deep aspects of the bowel mucosa (Fig. 6). Fourteen days after IRE, there was resolution of acute inflammation in the mucosa. Both mucosal and muscularis layers did not show any pathologic alterations. The serosa demonstrated fibrosis in the area immediately adjacent to the ablation site.

H&E stains of small bowel after 3 days. Acute and chronic inflammation with fibroblastic stromal response was seen in the serosa. Rare acute inflammatory cells were seen in the muscularis. Acute inflammation, with neutrophils in the lamina propria, cryptitis, and crypt abscesses were focally present in the deep aspects of the bowel mucosa. This inflammatory response resolved on day 14. Color images are available online.
Discussion
In our porcine model, we confirm our hypothesis that IRE can be safely used to ablate kidney tissue, while avoiding major injury to adjacent ureter and bowel. Despite effective ablation of adjacent renal parenchyma, there was no evidence of ureteral stricture on RPG or bowel perforation. Although there were mild similar inflammatory changes to both ureter and bowel, these resolved by day 14. This is the first study to specifically evaluate these organ injuries after IRE for kidneys. Recently, Fritz and colleagues 10 showed effective IRE of mesenteric lymph nodes of the small bowel in 10 pigs without evidence of damage to the bowel or any other adjacent organs. In humans, a state-of-the-art article by Wagstaff and colleagues 11 on IRE did not demonstrate any major complications on any of the kidney studies reviewed. In our own clinical experience with IRE in 42 kidney tumors in 41 patients, there were no major complications and 9 (22%) Clavien grade 1 complications. 5 This study on ablations close to ureter and bowel adds to the literature on the safety of IRE.
Bowel and ureteral injuries can be some of the most devastating injuries after RFA or CA. 2,12 Temperatures exceeding 60°C and lower than −20°C cause lethal thermal damage during RFA and CA, respectively. 1,13 Injuries to adjacent organs are thus a direct result of thermal energy-induced tissue necrosis and, therefore, it is recommended that vital structures are kept >1 cm away from the ablation zone. Fortunately, these complications are rare with experience and proper case selection. Hydrodissection is an increasingly popular technique used to effectively prevent injuring adjacent organs and offer definitive treatment for patients not able to undergo partial nephrectomy. 14 However, this increases procedural complexity, increases time, and adds risk.
IRE can be both nonthermal and thermal depending on the generator settings. IRE ablations in porcine kidneys have shown a significant temperature rise that may occur when repetitive high-intensity pulses are applied. 15 Olweny and colleagues 16 showed that thermal IRE measured at ∼90°C in the ablation zone caused significant collecting system injury on RPG compared with no collecting system damage using nonthermal IRE measured at 50°C in a porcine model. We have previously experimented with varying IRE voltage parameters and probe exposures in a porcine model as well. Our experiments showed that voltages of 2000 V/cm caused the largest lesion size while keeping temperatures in nonthermal ranges (<60°C). 9 Given these data and our clinical experience with IRE, we chose this voltage setting for our intentional adjacent ureteral and bowel ablations.
The significance of our study is differentiating a role for IRE among the current focal ablative therapies. As traditional ablative modalities such as RFA and CA have shown similar oncologic efficacy and side effects, 6 the choice between one or the other usually is dependent on the physician's familiarity and/or institution's availability. Evaluation of IRE for SRM as an alternative ablative modality has shown several distinctions that may make it suitable or preferable for specific patient populations. Although central tumors are poor candidates for thermal ablation because of the “heat-sink” phenomenon, 1 IRE may be useful for these tumors because of its nonthermal properties. Thomson and colleagues 17 reported no major complications demonstrating the safety of IRE for central tumors. For patients with tumors lying close to body-wall musculature, IRE offers a less painful alternative to RFA by minimizing activation of adjacent nociceptive receptors in the muscle. 7,18 Our study suggests it may also have a useful specific role for medial or anterior tumors in proximity to bowel or ureter.
In comparison with extirpation and conventional thermal ablation modalities, IRE for SRM thus far has shown suboptimal oncologic efficacy. Canvasser and colleagues 5 recently reported a 2-year local recurrence-free survival of 83% in those who had biopsy confirmed renal cell carcinoma. This is modestly inferior to a recent meta-analysis demonstrating a median local recurrence-free survival of 89.3% for both RFA and CA. 6 Although the short-term oncologic results of IRE do not compare favorably with long-term favorable outcomes with established ablative modalities for SRM, IRE is still relatively novel and perhaps more experience with ablation settings will improve results. Longer follow-up is still necessary to determine the durability of this modality compared with RFA and CA.
There exist several limitations to our study. We did not measure the temperature of our ablation site and thus cannot prove this was solely nonthermal ablation. However, our ablation settings used for this experiment have been shown to be well within nonthermal ranges and result in complete cell death based on our previous study. 9 Furthermore, it would have been interesting to see the effects of different ablation settings on the ureter and bowel, as current IRE ablation settings may be suboptimal. Our intention was to keep our ablation settings as uniform as possible between our limited subjects for internal validity for this experiment. In addition, after ablations were completed, the sutures holding the ureter and bowel on the kidney were cut to not cause any postoperative obstruction. It is unclear if leaving these segments attached to the kidney would cause any injury from the subsequent inflammatory cascade within the kidney after IRE. Longer follow-up would have been desirable for effects of ablation both clinically and histologically.
Conclusions
We demonstrate that IRE does not cause significant injury to adjacent ureter or bowel in a porcine model. This suggests that renal tumors contraindicated for RFA or CA because of high-risk locations may still be amenable to focal therapy through IRE.
Footnotes
Acknowledgments
We thank Dr. Matthew Riegel and Stephanie Shaffer for their help with this project and animal care.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.