
Abstract
Introduction and Objectives:
The GreenLight™ MoXy® laser fiber has been used since 2010 for benign prostatic hyperplasia procedures. We tested a novel principle to increase the saline irrigation flow rates beyond the current standard of gravity drip (∼22 cc/minutes) within the fiber-attached cooling system to potentially prevent excessive tissue adherence and to eliminate the likelihood of degradation due to abnormal overheating. The objective was to assess differences between the ordinary and active pumping methods with ≥2 times flow rate after conditioning of the laser fiber.
Materials and Methods:
A controllable full, tissue-contact system was utilized for conditioning in a porcine model, applying 180 W of vaporization mode of GreenLight XPS console for 30 continuous minutes. Four groups were evaluated using different saline flow rates; the nominal flow rate (control group, 22 mL/minute), digital pump set (35 mL and 50 mL/minute), and a manual pressure cuff with hand pump set using a 3-L saline bag with pressure of 300 mmHg (35–80 mL/minute). At the end of the conditioning process, a mechanical pull force test was executed on the fiber metal cap to evaluate the bonding strength. A failed event was defined as the natural detachment of the metal cap during the conditioning process or a cap pull force smaller than 22.24 N resulting in detachment. Additional physical parameters, including fiber tip temperature information and laser beam power transmission efficiency, were analyzed.
Results:
Detachment of the cap occurred less frequently when using the 300 mmHg pressure cuff saline bag compared to the nominal flow rate (6.67% vs 50%, respectively). The average operating fiber tip temperatures were lower in the higher flow rate groups compared to nominal, measured at 315°C and 305°C. compared to 442°C. Moreover, a significantly lower FiberLife Event count and an ∼5% increase of the average final laser transmission efficiency were observed in the higher flow rate groups.
Conclusions:
Our study demonstrates superior results when using active pumping or high-pressure systems to increase saline flow rates in terms of laser fiber durability without any additional cost. More specifically, use of a manual pressure cuff with starting pressure at 300 mmHg, a system that is readily available in most operating rooms, increases MoXy fiber durability. Further studies are required to assess if this technique will improve user experience, clinical outcomes, and procedure costs.
Introduction
Novel benign prostatic hyperplasia (BPH) treatment modalities, such as GreenLight photovaporization (GL-PVP), are alternatives to the reference standard transurethral resection of the prostate (TURP). 1 Aside from comparable long-term outcomes to TURP 2 and its minimally invasive approach, benefits of GL-PVP include shorter hospitalization and catheterization times, and overall coagulation performance, which is advantageous for patients presenting with comorbidities, including cardiovascular disease, anticoagulation therapy requirements, or coagulopathies. 3,4
Nonetheless, GL-PVP presents its own inherent drawbacks. Inadvertent contact with prostate tissue during high-power vaporization leads to overheating of the laser fiber tip induced by tissue carbonization. In early generations of GL-PVP systems, the laser fibers with older designs resulted in significant decrease in power transmission due to fiber devitrification, and thus reduced working efficiency and increased operative times. 5
Working with the GreenLight XPS 180 W laser console the side firing GreenLight™ Moxy® laser fiber (Boston Scientific, Marlborough, MA) with 2.10 mm outer diameter, 750 μm core diameter features an active and continuous room temperature saline cooling channel, and a ∼14 mm stainless steel cap that mechanically protects the glass fiber tip and prevents tissue from contacting the glass cap except at the transmissive window. Separated from the irrigation for the cystoscope, gravity-fed saline flows through standard intravenous plastic tubing that connects to the fiber channel proximal to the fiber control knob. Saline travels in between the metal cap and the fiber and exits from the output window of the cap to clean/cool the fiber tip. 6
The newest iteration of the GL-PVP featuring the MoXy laser fiber has allowed for an ∼50% increase in rate of vaporization compared to its predecessor due to increased laser power and the beam irradiated area, improving the operative speed 6 with insignificant power loss during GL-PVP. 5
To avoid energy loss and overheating of the laser fiber, effective cooling is key to maintaining fiber power transmission, ensuring the reliability of the fiber delivery device and increasing longevity. One issue that still remains is occasional overheating of the metal cap resulting in its detachment, extending treatment times and increasing procedure costs as the entire laser fiber must be replaced. This is particularly true in procedures involving the treatment of larger prostate glands, in which an average of 2.6 fibers is required. 7
In the present ex vivo study, we sought to assess a novel and simple irrigation method to improve the cooling system efficacy and decrease the risk of metal cap detachment due to abnormal overheating induced by excessive tissue adherence, with hopes that this method may reduce the number of laser fibers required per procedure when translated into the clinical setting.
Methods
All testing was reviewed and approved through an internal review process by Boston Scientific Corporation.
Ex vivo tissue-contact laser conditioning
A semiautomatic 3-axis control fixture was utilized for bench testing of porcine tissue at full contact throughout the process, Figure 1A. One hundred eighty watts of vaporization mode of GreenLight XPS console was applied continuously for 30 minutes to reach a delivery of 300 kJ, Figure 1B. To ensure consistent and effective vaporization, the laser testing was conducted only on unablated tissue surfaces, with new porcine tissue being used when required.
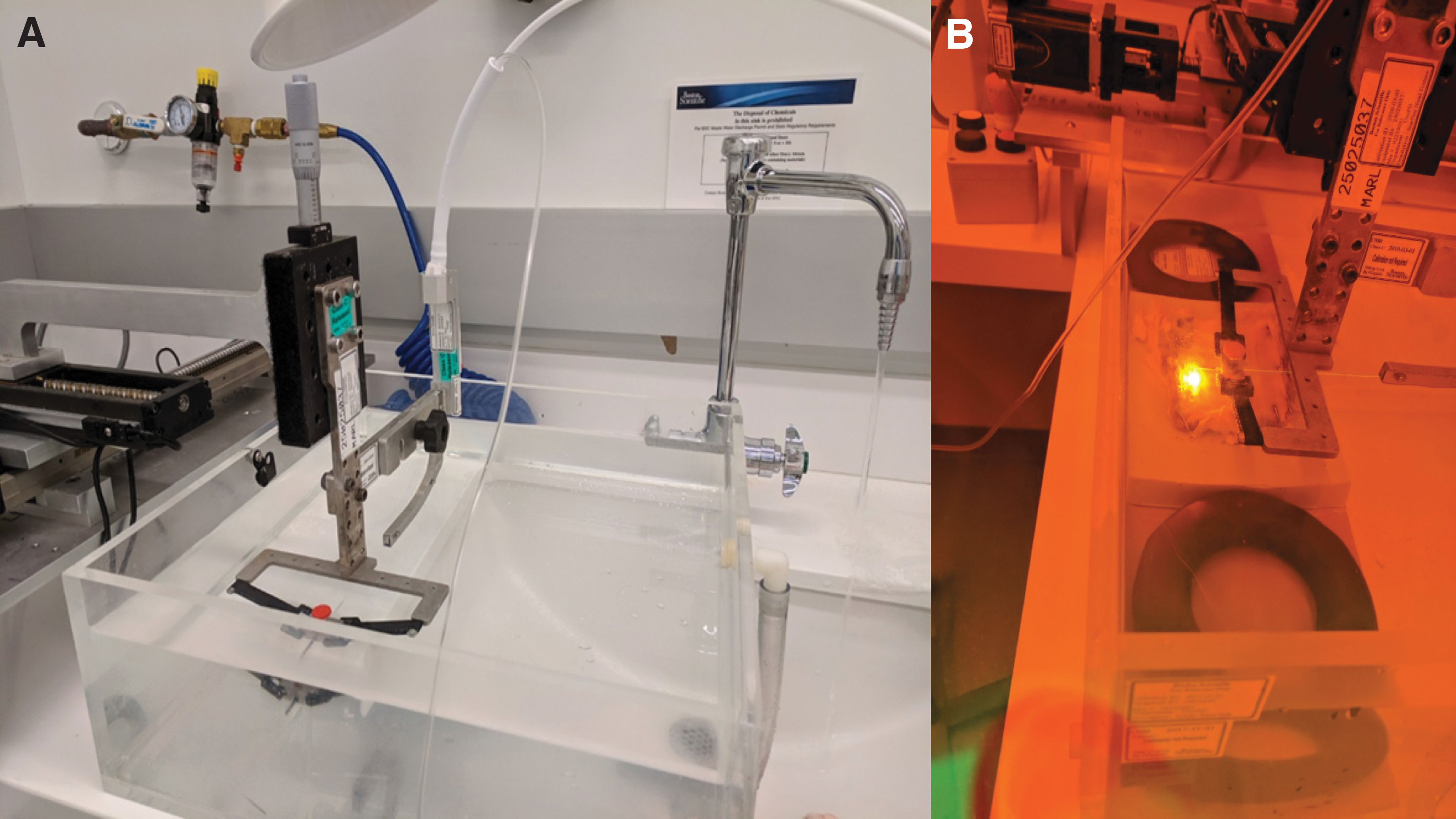
Semiautomatic 3-axis control fixture for the GreenLight XPS system.
The laser fiber automatically moved in an X-Y plane in a raster scan pattern in size of 32 by 82 mm, with a scanning speed of 2.6 mm/second. The distance between each 82 mm long line was ∼2.1 mm. The laser fiber was adjusted manually via a micrometer screw in the Z-axis with close monitoring to ensure full fiber-tissue contact. During the conditioning phase, tissue contact could be impacted by the following factors, and the laser fiber tip was adjusted accordingly: fiber tip movement resistance due to burned tissue and built up debris, light/shallow burn marks would be created if there was not enough contact, and inadvertent direct tissue contact would cause a spike in temperature.
The purpose of the conditioning process was to prepare the laser fiber in an accelerated degradation process with controllable full tissue-contact that could simulate most clinically extreme cases, before assessing the laser fiber integrity.
Tensile pull force evaluation
A mechanical pull force test (Instron 5564 Tensile Pull Tester) was executed on the fiber metal cap to evaluate the bonding strength after the previous tissue-contact conditioning process. A localized high-temperature environment was expected to be generated, with potential resultant degradation of cap bonding strength. The purpose of this step was to assess the integrity of the fiber metal cap after conditioning (Fig. 2). A failed event was defined as if the tensile pull force to achieve the cap detachment after conditioning was <22.24 N. This included any cases where the metal cap detached naturally during conditioning, as it was considered as requiring a pull force of 0 N to achieve detachment. A pull force of 22.24 N was defined as the cutoff for a failed event as it reproducibly and repeatedly resulted in an ∼50% cap failure rate when used with the usual recommended gravity-fed saline at a nominal flow rate.

Increased saline irrigation flow rate
Four groups were evaluated with different flow rate configurations during the MoXy tissue-contact conditioning, including the control nominal group (n = 16) with gravity-fed saline corresponding to a flow rate of 22 mL/minute (Saline bag height ≥106 cm per product instruction for use), and three active pumping modalities; intermediate 35 mL/minute (n = 5) and 2 × nominal flow rate 50 mL/minute (n = 15) measured by digital pump (Cole-Parmer Canada Company, Montreal, Canada), and pressure cuff with manual hand pump (TapMedic, Jacksonville) targeting 300 mmHg of pressure corresponding to a flow rate of 35–80 mL/minute (n = 15). All four groups utilized room temperature saline.
Fifteen ex vivo testing was estimated as the minimal sample size per group for the feasibility study with statistical significance. Since ≥2 × nominal flow rate was our targeted study between the active and passive pumping methods, fewer samples (n = 5) were tested at the intermediate rate of 35 mL/minute.
Three hundred mmHg was the target pressure range selected for the manual pressure cuff method with 3 L saline bag as it was the value within the middle of the safe (green) pressure range indicated by the pressure gauge used during conditioning. Notably, if no pressure readjustment was introduced, the flow rate tended to decrease during the test due to decreased saline volume and possible adherent tissue at the fiber tip, therefore the pressure cuff was readjusted to meet the target pressure during the tissue-contact laser conditioning.
Fiber tip temperature information
Thermal radiation produced at the laser fiber tip travels backward along the fiber to the FiberLife module inside the XPS laser. Heat signals at the fiber tip during the conditioning process was monitored by the module and converted into temperature information. This signal data processing utilized a Blackbody radiation calibration constant preset for the XPS laser.
Average tip temperature was derived from real-time data during the 30-minute tissue-contact conditioning process. A baseline of 100°C was used to exclude any data points created without tissue-contact, based on a thermocouple measurement.
In cases where the laser fiber tip exceeded a preset threshold value of 825°C, a FiberLife event was triggered and recorded. In general, FiberLife is a safety feature of GreenLight XPS console that prevents the MoXy fiber tip from overheating due to direct tissue contact or inadequate saline cooling at the distal tip by briefly blocking the laser output, and further putting the console to Standby mode if required.
Laser transmission
Laser transmission efficiency was measured before and after tissue-contact laser conditioning using a separate fixture with a laser output power of 20 W with a laser energy sensor (Ophir Optronics, Jerusalem, Israel) and power meter (Coherent, CA). Tissue that became adherent to the fiber tip after conditioning was not cleaned off during these measurements.
Statistical analysis
Student's t-test was performed for the comparison between the three individual active pumping modalities compared to the control nominal group using Microsoft Excel software. All tests were two-sided with a significance level set at p = 0.05.
Results
Numbers of test performed for each flow rate group are shown in Table 1.
Tensile Pull Force Data (N) vs Flow Rate Groups
Number of failed events after tensile pull force evaluation is used to assess structural integrity of laser fiber after tissue-contact laser conditioning. A failed event was defined as if the metal cap detached naturally during conditioning or if the tensile pull force to achieve the cap detachment after conditioning was <22.24 N. Minimum and maximum tensile pull forces were documented in cases of survived samples only (>22.24 N pull force to achieve detachment).
SD = standard deviation.
Tensile pull force evaluation
Within the nominal group (22 mL/minute, n = 16), 50% of tests had failed events, which is defined as cap or tip detachment during the prior laser conditioning phase, or due to less than a 22.24 N pull force. A mean force ± standard deviation of 45.21 ± 44.21 N was required to achieve cap or tip detachment for the eight survived samples within the nominal group. In addition, at a saline irrigation rate of 50 mL/minute (n = 15), there were no failed events during the conditioning phase or the tensile pull force evaluation, and a mean pull force of 73.19 ± 22.45 N was required to achieve metal cap or tip detachment (p = 0.03, when compared to nominal group).
Notably, while using the pressure cuff set at 300 mmHg, corresponding to 35–80 mL/minute (n = 15), only 6.67% of tests had a failed event, and a mean pull force of 75.24 ± 26.09 N was required to achieve metal cap or tip detachment (p = 0.02, when compared to nominal group). Forty percent of tests had failed events during the conditioning phase or the tensile pull force evaluation for an intermediate flow rate set at 35 mL/minute (Table 1, Fig. 3). In cases of survived samples, the minimum tensile pull force required to achieve cap or tip detachment was 37.1 N in the nominal group, compared to 49.5 N in the 300 mmHg pressure cuff group.

Failed cap detachment (%) and average tensile pull force (N) during tensile pull force evaluation after 30 minutes of tissue-contact laser conditioning to achieve 300 kJ. *p < 0.05 when compared to nominal group.
Fiber tip operating temperatures
Within the nominal group, the mean recorded temperature was 442°C, compared to 315°C (p < 0.01) and 305°C (p < 0.01) in the 50 mL/minute and 300 mmHg pressure cuff group, respectively (Fig. 4). In addition, there were 108 recorded FiberLife event counts in the nominal group (when the laser fiber tip reached a threshold temperature of 825°C), compared to 22 and 27, respectively, in the 50 mL/minute and 300 mmHg pressure cuff group (Fig. 4). Finally, there was an ∼5% increase of the mean final laser transmission efficiency in the pressure bag group compared to the nominal group, although not statistically significant (p = 0.13), Figure 5.

Average FiberLife temperature (°C) recorded during the 30-minute tissue-contact laser conditioning. *p < 0.01 when compared to nominal group.
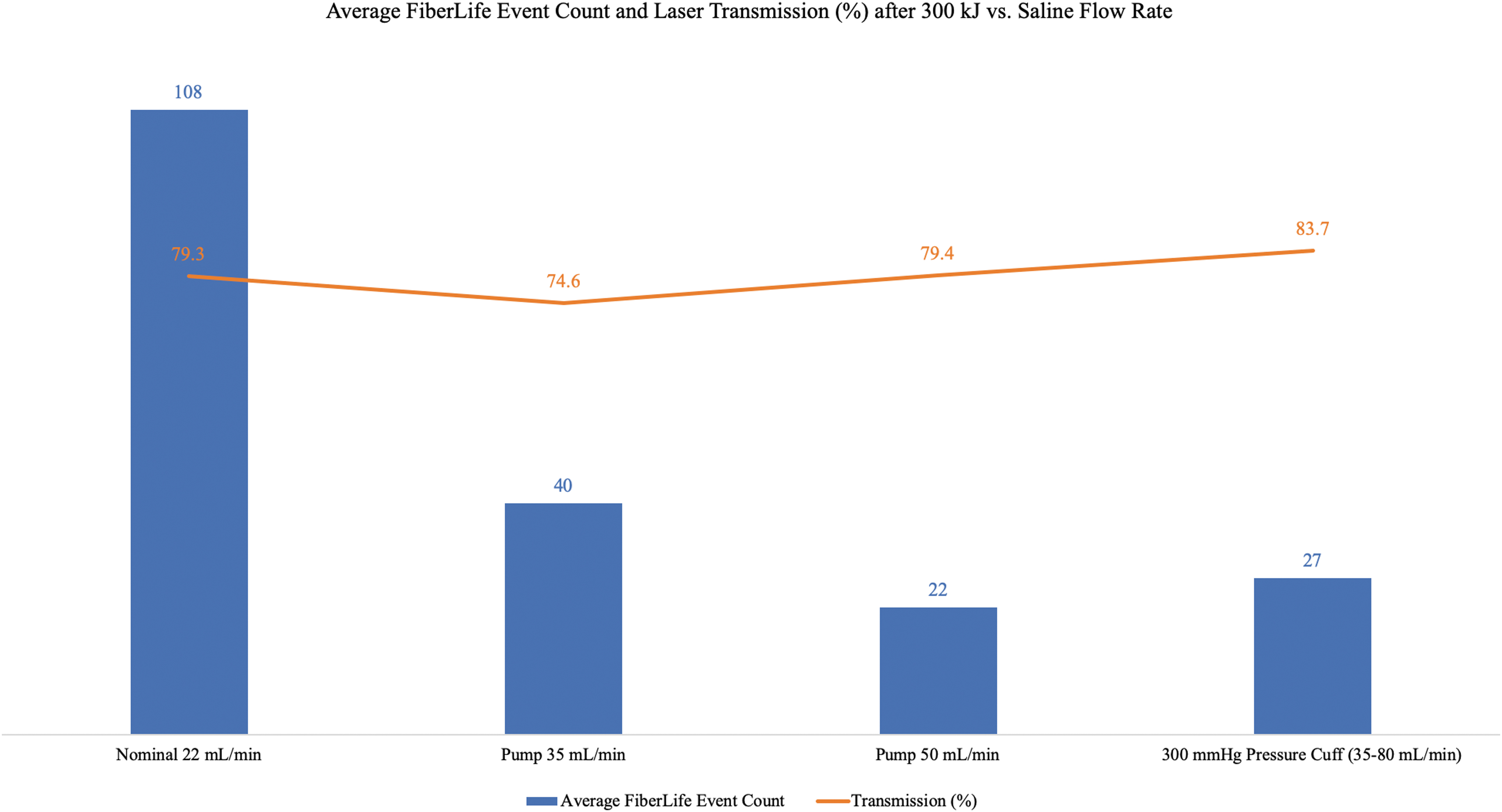
Average FiberLife event count and average laser transmission (%) recorded during the 30-minute tissue-contact laser conditioning.
Discussion
In this study, we explored whether increasing the flow rate of the liquid cooling system could further improve the efficiency and functionality of the XPS 180 W system as a pressurized saline system is readily available in most operating rooms without any additional costs.
Within the nominal group, representing the current standard of care (gravity-fed room temperature saline drip, 22 mL/minute liquid cooling), 50% of tests had failed the tensile pull force evaluation, while there were no failed evaluations in the 2 × flow rate (50 mL/minute). Moreover, when using the manual pressure cuff targeting 300 mmHg, estimated to 35–80 mL/minute, only 6.67% of tests had failed tensile pull force evaluation (Fig. 3). This is significant as manual pressure cuffs are readily available in most operating rooms and thus the increased saline flow rates can be applied in most institutions offering GL-PVP.
In addition, the increased flow rates of liquid cooling conferred improved physical integrity of the laser fiber-metal cap as evidenced by the significantly increased tensile pull force required for detachment. The highest flow rate tested within this ex vivo study was 80 mL/minute, which was documented within the 300 mmHg pressure cuff group. Practically, increasing pressures >300 mmHg resulted in the saline bag being squeezed out of the pressure cuff. As such, testing did not include flow rates >80 mL/minute.
Underlying the improvement in failed cap detachment rates between the nominal and 300 mmHg pressure bag group was likely the decrease in mean fiber tip temperature during the tissue-contact laser conditioning, at 442°C and 305°C, respectively (p < 0.05) (Fig. 4). In addition, with higher rates of liquid cooling, there were fewer FiberLife events, in which the laser had briefly worked in pulsing mode due to reaching a threshold temperature of >825°C (27 events for the pressure cuff group, compared to 105 in the nominal group, Fig. 5). FiberLife is a safety feature of the GreenLight XPS console that prevents the MoXy Fiber tip from overheating, specifically in cases of inadvertent direct tissue contact, or inadequate saline cooling at the laser fiber tip. Increasing saline flow rates extends the metal cap integrity and decreases overall fiber temperature; therefore, the number of FiberLife events was reduced. Fewer FiberLife events translates to more time spent in full vaporization mode, which is advantageous in the clinical setting and would likely contribute to improved procedural efficacy.
The overall significant decrease in average fiber tip temperature has important clinical implications. During GL-PVP, a single MoXy laser fiber can endure a recommended maximum of 650 kJ. In cases of GL-PVP where prostate volume was >80 cc, numbers of fibers used were significantly greater than in cases where prostate volume was <80 cc. 8 For prostates >200 cc, upward of three laser fibers were required to complete the procedure. 7 By maintaining an overall cooler tip temperature, we believe this would improve the overall physical integrity of the laser fiber and metal cap, reducing the need to use multiple fibers per case. In addition to potentially shortening operative times, reducing the need to use multiple laser fibers would have a large financial implication, as the cost per fiber can be upwards of $1200.00, varying by region.
Finally, we aimed to assess whether increasing liquid cooling flow rates would have a functional impact on laser transmission by comparing the absolute efficiency of laser transmission before and after the conditioning step. One potential effect of decreasing overall fiber tip temperatures through increased flow rates is a mitigation of laser fiber devitrification. We expected that the mitigations would contribute to consistency of high laser transmission efficiency. The decrease in laser transmission efficiency of the nominal group was 5% larger when compared to the 300 mmHg pressure cuff group, at 79.3% and 83.7%, respectively, although this finding was not statistically significant, Figure 5. During this evaluation, we did not remove any adherent tissue on the laser fiber tip after the conditioning process, which may have essentially reduced the laser transmission measurements. Otherwise, we may have perhaps seen an improvement in laser transmission.
Since its initial commercialization in 2000, GL-PVP has become widely accepted as a treatment modality for BPH, with advantages, including use in patients with anticoagulation requirements, decreased rates of TUR syndrome, and shorter hospitalization times. 3,4 GreenLight laser technology emits 532 nm wavelength light, to specifically target hemoglobin, leading to selective vaporization of vascularized tissue. When compared to reference standard TURP, recent studies have demonstrated that GL-PVP with the 180 W XPS system is a safe and effective BPH treatment modality, 9 and that it demonstrates noninferiority to TURP on International Prostate Symptom Score (IPSS), Qmax, freedom from complications, with similar reductions in prostate volume and prostate-specific antigen sustained over 2 years. 10
Continued use of this technology for the treatment of BPH has led to its improvement with the introduction of novel techniques such as standard PVP, anatomical PVP, 11 and GreenLight enucleation of the prostate, 12 as well as the development of three major laser iterations, the latest being the GreenLight XPS 180 W system in 2011. The early generations of GreenLight laser fibers that worked with 80 W PV and 120 W HPS GreenLight laser systems were criticized for significant power loss during the procedure due to tissue carbonization-induced fiber tip overheating. During the vaporization of prostatic tissue, tissue debris accumulated on the surface of the laser fiber. Accumulated tissue coated the fiber tip with a thin coagulum film that underwent carbonization due to the residual heat of the laser. It was this carbonization process that caused the tip of the fiber to overheat, leading to potential laser fiber fracture, compromising the fibers ability to maintain efficiency energy transmission. This would result in overall degradation and premature failure of the laser fiber, ultimately leading to prolonged operative times as well as operative costs (greater use of one fiber per case). 13,14
When compared to the earlier GL-PVP systems, the XPS 180 W system featured the MoXy laser fiber, which incorporated a stainless steel protective cap and active liquid cooling to reduce rates of fiber fracture and devitrification. 15 As a result of an overall higher maximum energy output, paired with the liquid cooling laser fiber, the XPS 180 W system demonstrated insignificant laser transmission degradation, with maintenance of its power output throughout the procedure. 5 Introduction of the new XPS 180 W system significantly improved operative times, mitigating one of the larger criticisms toward GL-PVP. 16
However, despite these important protective feature improvements to the MoXy fiber design, the MoXy fiber is sensitive for its glue attachment of the metallic cap, which was not an issue with the previous 2090 laser fiber. In addition, the changes to the design do not completely prevent fiber tip overheating and the occasional detachment of the metal cap, particularly in cases of unintentional close fiber-tissue contact (Fig. 2).
While this study clearly demonstrated that increasing saline flow rates improved metal cap integrity and decreased overall fiber temperatures, further clinical studies are required to assess if this technique will result in a reduction of laser fibers used per procedure, as well as improve user experience, clinical outcomes, and procedure costs. Furthermore, all testing performed in this ex vivo study utilized room temperature saline. It would be interesting to consider the impact of using cooled irrigation on lowering the fiber tip temperature. Notably, given that the flow rates utilized in the cooling system are in the milliliter per minute range, the advantage of water's high heat capacity may quickly diminish as it has a small volume compared to the relatively larger mass of the metal cap and fiber tip region, especially when the laser output power was set at 180 W.
Our study is subject to limitations because it is an ex vivo study. For this reason, we could not evaluate how different vaporization techniques, surgeon's skill level, and prostate volume may influence the performance and durability of the laser fiber.
Despite these limitations, to our knowledge, this is the first study to date that assesses the impact the active pumping saline cooling system has on the laser fiber performance improvement and durability.
Conclusion
Overall, this study provides an in-depth understanding of how MoXy fiber performs during an ex vivo tissue-contact test from an opto-thermal-mechanical perspective and will assist all practitioners in the field to improve their MoXy laser fiber user experience. We have developed and evaluated a low-cost highly effective technique that can significantly improve laser fiber durability. With a pressurized saline bag maintaining at a range of 300 mmHg, we have achieved a significant decrease in cap detachment after 300 kJ full tissue-contact bench testing at 180 W of GreenLight XPS vaporization mode. Our study demonstrates superior results using the high-flow-rate saline cooling system, without any additional cost, given that the recommended pressurized system is readily available in most operating rooms.
Footnotes
Disclaimer
Important Information: These materials are intended to describe common clinical considerations and procedural steps for the use of referenced technologies, but may not be appropriate for every patient or case. Decisions surrounding patient care depend on the physician's professional judgment in consideration of all available information for the individual case. Boston Scientific Corporation (BSC) does not promote or encourage the use of its devices outside their approved labeling. Case studies are not necessarily representative of clinical outcomes in all cases as individual results may vary. Testing was performed by BSC. Bench Test results may not necessarily be indicative of clinical performance.